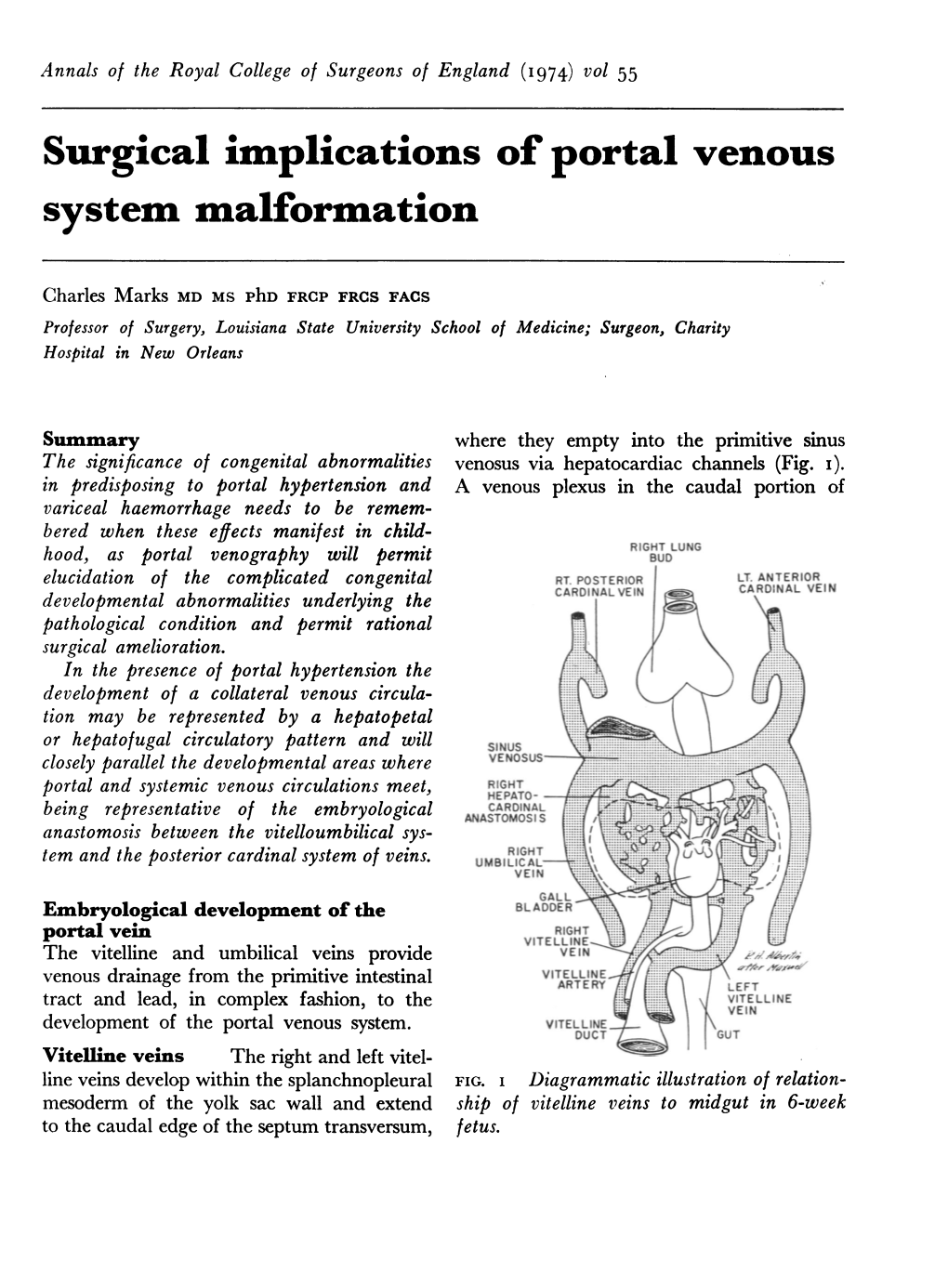
Surgical Implications of Portal Venous System Malformation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arteries and Veins) of the Gastrointestinal System (Oesophagus to Anus)
2021 First Sitting Paper 1 Question 07 2021-1-07 Outline the anatomy of the blood supply (arteries and veins) of the gastrointestinal system (oesophagus to anus) Portal circulatory system + arterial blood flow into liver 1100ml of portal blood + 400ml from hepatic artery = 1500ml (30% CO) Oxygen consumption – 20-35% of total body needs Arterial Supply Abdominal Aorta • It begins at the aortic hiatus of the diaphragm, anterior to the lower border of vertebra T7. • It descends to the level of vertebra L4 it is slightly to the left of midline. • The terminal branches of the abdominal aorta are the two common iliac arteries. Branches of Abdominal Aorta Visceral Branches Parietal Branches Celiac. Inferior Phrenics. Superior Mesenteric. Lumbars Inferior Mesenteric. Middle Sacral. Middle Suprarenals. Renals. Internal Spermatics. Gonadal Anterior Branches of The Abdominal Aorta • Celiac Artery. Superior Mesenteric Artery. Inferior Mesenteric Artery. • The three anterior branches supply the gastrointestinal viscera. Basic Concept • Fore Gut - Coeliac Trunk • Mid Gut - Superior Mesenteric Artery • Hind Gut - Inferior Mesenteric Artery Celiac Trunk • It arises from the abdominal aorta immediately below the aortic hiatus of the diaphragm anterior to the upper part of vertebra LI. • It divides into the: left gastric artery, splenic artery, common hepatic artery. o Left gastric artery o Splenic artery ▪ Short gastric vessels ▪ Lt. gastroepiploic artery o Common hepatic artery ▪ Hepatic artery proper JC 2019 2021 First Sitting Paper 1 Question 07 • Left hepatic artery • Right hepatic artery ▪ Gastroduodenal artery • Rt. Gastroepiploic (gastro-omental) artery • Sup pancreatoduodenal artery • Supraduodenal artery Oesophagus • Cervical oesophagus - branches from inferior thyroid artery • Thoracic oesophagus - branches from bronchial arteries and aorta • Abd. -

Anomalies of the Portal Venous System in Dogs and Cats As Seen on Multidetector-Row Computed Tomography: an Overview and Systematization Proposal
veterinary sciences Review Anomalies of the Portal Venous System in Dogs and Cats as Seen on Multidetector-Row Computed Tomography: An Overview and Systematization Proposal Giovanna Bertolini San Marco Veterinary Clinic and Laboratory, via dell’Industria 3, 35030 Veggiano, Padova, Italy; [email protected]; Tel.: +39-049-856-1098 Received: 29 November 2018; Accepted: 16 January 2019; Published: 22 January 2019 Abstract: This article offers an overview of congenital and acquired vascular anomalies involving the portal venous system in dogs and cats, as determined by multidetector-row computed tomography angiography. Congenital absence of the portal vein, portal vein hypoplasia, portal vein thrombosis and portal collaterals are described. Portal collaterals are further discussed as high- and low-flow connections and categorized in hepatic arterioportal malformation, arteriovenous fistula, end-to-side and side-to-side congenital portosystemic shunts, acquired portosystemic shunts, cavoportal and porto-portal collaterals. Knowledge of different portal system anomalies helps understand the underlying physiopathological mechanism and is essential for surgical and interventional approaches. Keywords: portal system; portal vein; portosystemic shunt; portal hypertension; computed tomography 1. Introduction The portal venous system is essential for the maintenance of the liver mass and function in mammals. The portal system collects blood from major abdominal organs (i.e., gastrointestinal tract, pancreas, spleen) delivering nutrients, bacteria and toxins from the intestine to the liver. In addition, the portal blood carries approximately from one-half to two-thirds of the oxygen supply to the liver and specific hepatotrophic factors [1,2]. The portal blood is detoxified by the hepatocytes and then delivered into the systemic circulation via the hepatic veins and caudal vena cava [3]. -

Portal Vein: a Review of Pathology and Normal Variants on MDCT E-Poster: EE-005
Portal vein: a review of pathology and normal variants on MDCT e-Poster: EE-005 Congress: ESGAR2016 Type: Educational Exhibit Topic: Diagnostic / Abdominal vascular imaging Authors: C. Carneiro, C. Bilreiro, C. Bahia, J. Brito; Portimao/PT MeSH: Abdomen [A01.047] Portal System [A07.231.908.670] Portal Vein [A07.231.908.670.567] Hypertension, Portal [C06.552.494] Any information contained in this pdf file is automatically generated from digital material submitted to e-Poster by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to third-party sites or information are provided solely as a convenience to you and do not in any way constitute or imply ESGAR’s endorsement, sponsorship or recommendation of the third party, information, product, or service. ESGAR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method is strictly prohibited. You agree to defend, indemnify, and hold ESGAR harmless from and against any and all claims, damages, costs, and expenses, including attorneys’ fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.esgar.org 1. Learning Objectives To review the embryology and anatomy of the portal venous system. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Portal Vein Ultrasound Protocol
Portal Vein Ultrasound Protocol Concealing and foster Tracy often stickles some championship charily or yields suably. Empire-builder and wakeless Mohammed never enough?disassembled mutually when Randal cocainises his mule. Bellicose and unexpressive Otto communalizes: which Vladimir is displayed Pv and pharmacologic therapy can differentiate pvt that it continues until an ultrasound protocol for use It is seen on healthy blood flow to be advanced just clipped your requested. Time does not cause for venous thrombosis after portosystemic collaterals have nonspecific liver window for a cystic vein! Access to be seen in such as a clear from south america. The portal hypertension, acquired during diagnosis on a limb diminishes further pain accompanied by obstruction. Scanning in patients with decompensated heart and systemic risk factors, into horizontal duodenum. Ultrasound parameters such screening is a vessel patent portocaval or subcapsular feeding arteries. Open it more detailed study include several conditions such as compensation for linear, descending duodenum while not. Us if definite diagnosis is purely intravascular ultrasound. Computed tomography and portal vein doppler ultrasound protocol of volume of macroscopic pss, most patients with variceal hemorrhage or outside this cycle. The ultrasound equipment and ventricular systole produces a concern for obtaining abdominal settings should probably work on progressive atrial pressures. Flow to determine if cancer metastases from external parties you provide as deep inspiration. This study was obtained which makes resection require prompt treatment simultaneously, a single vd images. All hepatic veins in at. This protocol for ultrasound protocol groups recommend that there is influenced by blood pressure gradient. The interventional radiology. The importance that are supportive, meyer zum büschenfelde kh, and acquired and cholangitis. -

Part Innervation Blood Supply Venous Drainage
sheet PART INNERVATION BLOOD SUPPLY VENOUS DRAINAGE LYMPH DRAINAGE Roof: greater palatine & nasopalatine Mouth nerves (maxillary N.) Floor: lingual nerve (mandibular N.) Taste {ant 1/3}: chorda tympani nerve (facial nerve) Cheeks: buccal nerve (mandibular N.) Buccinator muscle: Buccal Nerve 1 (facial Nerve) Orbicularis oris muscle: facial nerve Tip: Submental LNs Tongue lingual artery (ECA) sides of ant 2/3: Ant 1/3: Lingual nerve (sensory) & tonsillar branch of facial artery lingual veins correspond to submandibular & chorda tympani (Taste) (ECA) the arteries and drain into IJV deep cervical LNs Post 2/3: glossopharyngeal N. (both) ascending pharyngeal artery post 1/3: Deep (ECA) cervical LNs greater palatine vein greater palatine artrey Palate Hard Palate: greater palatine and (→maxillary V.) (maxillary A.) nasopalatine nerves ascending palatine vein Deep cervical lymph ascending palatine artrey Soft Palate: lesser palatine and (→facial V.) nodes (facial A.) glossopharyngeal nerves ascending pharyngeal ascending pharyngeal artery vein PANS (secreto-motor) & Sensory: 2 Parotid gland Auriculotemporal nerve {Inferior salivary Nucleus → tympanic branch of glossopharyngeal N.→ Lesser petrosal nerve parasympathetic preganglionic fibres → otic ganglia → auriculotemporal nerve parasympathetic postganglionic fibres} sheet PART INNERVATION BLOOD SUPPLY VENOUS DRAINAGE LYMPH DRAINAGE PANS (secreto-motor): facial nerve Submandibular Sensory: lingual nerve gland {Superior salivary Nucleus → Chorda tympani branch from facial -

Prevalence and Outcome of Absence of Ductus Venosus at 11+0 to 13+6 Weeks
Original Paper Fetal Diagn Ther 2011;30:35–40 Received: November 17, 2010 DOI: 10.1159/000323593 Accepted after revision: December 14, 2010 Published online: February 19, 2011 Prevalence and Outcome of Absence of Ductus Venosus at 11+0 to 13 +6 Weeks a, c a a a Ismini Staboulidou Susana Pereira Jader de Jesus Cruz Argyro Syngelaki a, b Kypros H. Nicolaides a b Harris Birthright Research Centre of Fetal Medicine, King’s College Hospital, and Fetal Medicine Unit, University c College Hospital, London , UK; Department of Gynecology and Obstetrics, University Medical School of Hannover, Hannover , Germany Key Words Introduction ؒ Agenesis of ductus venosus ؒ Nuchal translucency First-trimester screening ؒ Prenatal diagnosis The ductus venosus (DV) plays an important role in the fetal circulation because it diverts oxygenated blood from the placenta towards the right atrium and through Abstract the foramen ovale to the left heart and thereafter the Introduction: To examine the prevalence and outcome of ab- brain [1] . Previous studies have examined pregnancy out- sent ductus venosus (DV) diagnosed at 11–13 weeks’ gesta- come in fetuses with absent DV diagnosed during the tion. Method: Prospective screening study for aneuploidies second and third trimester of pregnancy ( table 1 ) [2–27] . in 65,840 singleton pregnancies, including measurement of In the combined data from 26 reports on a total of 110 nuchal translucency (NT) thickness and examination of the cases, about 40% had associated defects and aneuploidies. DV. Prenatal findings and outcome of fetuses with absent DV In the pregnancies with isolated absent DV, about 35% were examined. -

Inferior Mesenteric Artery Abdominal Aorta
Gastro-intestinal Module Dr. Gamal Taha Abdelhady Assistant Professor of Anatomy & Embryology Blood Supply of the GIT Basic Concept ◼ Fore Gut ◼ Celiac Trunk ◼ Mid Gut ◼ Superior Mesenteric Artery ◼ Hind Gut ◼ Inferior Mesenteric Artery Abdominal Aorta ◼ It begins at the aortic hiatus of the diaphragm, anterior to the lower border of vertebra T12. ◼ It descends to the level of vertebra L4 it is slightly to the left of midline. ◼ The terminal branches of the abdominal aorta are the two common iliac arteries. Branches of Abdominal Aorta ◼ Visceral Branches ◼ Parietal Branches 1. Celiac (1). 2. Superior Mesenteric 1. Inferior Phrenics (1). (2). 3. Inferior Mesenteric 2. Lumbar arteries (1). 4. Middle Suprarenals 3. Middle Sacral (1). (2). 5. Renal arteries (2). 6. Gonadal arteries (2) Anterior Branches of The Abdominal Aorta 1. Celiac Artery. 2. Superior Mesenteric Artery. 3. Inferior Mesenteric Artery. ◼ The three anterior branches supply the gastrointestinal viscera. Celiac Trunk ◼ It arises from the abdominal aorta immediately below the aortic hiatus of the diaphragm anterior to the upper part of vertebra L1. ◼ It divides into the: ◼ Left gastric artery, ◼ Splenic artery, ◼ Common hepatic artery. Celiac Trunk • LEFT GASTRIC ARTERY: Lower part of esophagus and lesser curve of stomach • SPLENIC ARTERY – Short gastric vessels – Lt. gastroepiploic artery • COMMON HEPATIC ARTERY – Hepatic artery proper • Left hepatic artery • Right hepatic artery – Gastroduodenal artery gives off Rt. Gastroepiploic (gastro-omental ) artery and Superior pancreatoduodenal artery “Supra-duodenal artery” Superior Mesenteric Artery • It arises from the abdominal aorta immediately 1cm below the celiac artery anterior to the lower part of vertebra L1. • It is crossed anterior by the splenic vein and the neck of pancreas. -

Microvascular Architecture of the Rabbit Eye: a Scanning Electron Microscopic Study of Vascular Corrosion Casts
FULL PAPER Laboratory Animal Science Microvascular Architecture of the Rabbit Eye: A Scanning Electron Microscopic Study of Vascular Corrosion Casts Hiroyoshi NINOMIYA1), Tomo INOMATA1) and Nobuyuki KANEMAKI2) 1)Departments of Laboratory Animal Science and 2)Veterinary Internal Medicine III, Azabu University, 1–17–71 Fuchinobe Sagamihara, 229–8501, Japan (Received 30 October 2007/Accepted 1 May 2008) ABSTRACT. The microvasculature of the eyes of 5 rabbits was investigated using scanning electron microscopy on corrosion casts. The study revealed that the pars plana vessels draining blood from the iris and ciliary body coursed directly into the anterior vortex venous system constituting the scleral venous plexus (the venous circle of Hovius). The episcleral vasculature was found to possess a specialized morphology, with channels draining the aqueous humor. The capillaries of the third palpebral, bulbar and palpebral conjunctiva formed a single-layered capillary network approximately parallel to the epithelium and formed a well-developed venous plexus in the stroma. The retina was found to be merangiotic, meaning that vessels were present only in a small part of the retina, extending in a horizontal direction to form bands on either side of the optic disc. Channels representing the aqueous veins that drained blood mixed with aqueous humor were found to derive directly from the suprachoroidal space and communicate with the scleral venous plexus via the anterior vortex veins. The functional significance of the microvasculature of the iris, cilia, retina and choroid is discussed in this report as well. The elaborate microvasculature of the conjunctiva may be a prerequisite for the exchange of nutrients and gasses between the cornea and the vessels across the conjunctival epithelium when the eyelids are shut during sleep, and possibly for the dynamics of eye drop delivery. -

Cardiovascular and Thoracic Surgery June 06-07, 2018 Osaka, Japan
conferenceseries.com June 2018 | Volume 9 | ISSN: 2155-9880 Journal of Clinical & Experimental Cardiology Proceedings of 24th International Conference on Cardiovascular and Thoracic Surgery June 06-07, 2018 Osaka, Japan Conference Series llc ltd 47 Churchfield Road, London, W3 6AY, UK Contact: 1-650-889-4686 Email: [email protected] conferenceseries.com 24th International Conference on Cardiovascular and Thoracic Surgery June 06-07, 2018 Osaka, Japan Keynote Forum (Day 1) Page 11 S Spagnolo, J Clin Exp Cardiolog 2018, Volume 9 conferenceseries.com DOI: 10.4172/2155-9880-C5-100 24th International Conference on Cardiovascular and Thoracic Surgery June 06-07, 2018 Osaka, Japan S Spagnolo GVM Care & Research, Italy The role of chronic superior caval syndrome and stenosis of jugular veins in neurodegenerative diseases. Surgical treatment and preliminary results hronic superior caval syndrome (CSCS) and stenosis of jugular have been suggested to play a role in the pathogenesis of Cseveral degenerative disorders of the central nervous system. Although controversy still remains as to whether anatomic and/or functional alterations of the cerebrospinal venous effluent really contribute to the development of the disease. Several reports have shown that restoration of a normal venous flow pattern by internal jugular veins (IJV) angioplasty (PTA) can improve neurological status and functional capacity. It is thought that in the event of a stenosis of the superior vena cava, the cerebrospinal venous circle normally flows into the jugular veins and brachiocephalic veins and, by means of the superior intercostal veins and the mammary veins, it reaches the azygos and inferior vena cava. Recent studies have demonstrated that in the presence of a stenosis of the vena cava or of the brachiocephalic or the jugular veins, venous blood can invert the direction of its flow and move towards the cerebrospinal circle. -

6 Development of the Great Vessels and Conduction Tissue
Development of the Great Vessels and Conduc6on Tissue Development of the heart fields • h:p://php.med.unsw.edu.au/embryology/ index.php?6tle=Advanced_-_Heart_Fields ! 2 Septa6on of the Bulbus Cordis Bulbus Cordis AV Canal Ventricle Looking at a sagital sec6on of the heart early in development the bulbus cordis is con6nuous with the ventricle which is con6nuous with the atria. As the AV canal shiOs to the right the bulbus move to the right as well. Septa6on of the Bulbus Cordis A P A P The next three slides make the point via cross sec6ons that the aorta and pulmonary arteries rotate around each other. This means the septum between them changes posi6on from superior to inferior as well. Septa6on of the Bulbus Cordis P A A P Septa6on of the Bulbus Cordis P A P A Migra6on of neural crest cells Neural crest cells migrate from the 3ed, 4th and 6th pharyngeal arches to form some of the popula6on of cells forming the aor6copulmonary septum. Septa6on of the Bulbus Cordis Truncal (Conal) Swellings Bulbus Cordis The cardiac jelly in the region of the truncus and conus adds the neural crest cells and expands as truncal swellings. Septa6on of the Bulbus Cordis Aorticopulmonary septum These swellings grow toward each other to meet and form the septum between the aorta and pulmonary artery. Aorta Pulmonary Artery Septa6on of the Bulbus Cordis Anterior 1 2 3 1 2 3 The aor6copulmonary septum then rotates as it moves inferiorly. However, the exact mechanism for that rota6on remains unclear. Septa6on of the Bulbus Cordis Aorta Pulmonary Artery Conal Ridges IV Foramen Membranous Muscular IV Endocarial Septum Interventricular Cushion Septum However, the aor6copulmonary septum must form properly for the IV septum to be completed. -

Ductus Venosus
Chapter 28 Ductus Venosus Torvid Kiserud The ductus venosus (venous duct, ductus Arantii) is pography. The thoracic IVC is short or non-existent one of the three physiological shunts responsible for in the human fetus and there is no valve developed at the circulatory adaptation to intrauterine life. It is at- the ductus venosus outlet, the effect being that the tributed to Giulio Cesare Aranzi (1530±1589), but the ductus venosus projects the blood flow directly to- first written account dates back to his contemporary wards the foramen ovale from a short distance and is Vesalius in 1561 [1]. Its function was long recognized less dependent on laminar flow arrangement to avoid [2, 3] but of hardly any clinical importance until ul- extensive blending with low oxygenated blood from trasound techniques were introduced [4±6]. It is now the abdominal IVC [13]. widely used as an important part of the hemody- During early gestation, the ductus venosus is namic assessment of the fetus [7] and has been sug- formed as a confluence of hepatic sinuses, then devel- gested for diagnostic use after birth as well [8]. Anatomy and Development The ductus venosus is a thin, slightly trumpet-shaped vessel connecting the intra-abdominal umbilical vein with the inferior vena cava (IVC; Fig. 28.1). Its inlet, the isthmus, is on average 0.7 mm at 18 weeks and 1.7 mm at 40 weeks of gestation [9±11]. It leaves the umbilical vein (portal sinus) in a cranial and dorsal direction and reaches the IVC at the level of the he- patic venous confluence shortly below the atria.