Clinical and Biochemical Features Guiding the Diagnostics in Neurometabolic Cutis Laxa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

De Barsy Syndrome: Orthopedic Case Report and Literature Review
MOJ Orthopedics & Rheumatology De Barsy Syndrome: Orthopedic Case report and Literature Review Introduction Case Report Volume 7 Issue 5 - 2017 This condition was first described in 1968 by De Barsy who and degeneration of the elastic tissue of the cornea and skin, Jose de Jesus Guerra Jasso1*, Douglas reported a case of a patient with progeria, dwarfism, oligofrenia and since then, it is known as Barsy Syndrome or Barsy- Colmenares Bonilla2 and Loreett Ocampo Perez3 of progeroid aspect, cutis laxa, corneal opacity, intrauterine 1Pediatric Orthopedics, Hospital Regional de Alta Especialidad growthMoens-Dierckx retardation Syndrome. and severe This ismental defined retardation as the combination (although del Bajio, Mexico some will learn to speak, intelligence is less than normal) [1]. 2Pediatric Orthopedic Service, Hospital regional de alta especialidad del bajio The orthopedic manifestations are dysplasia of hip development, 3Fellow of Pediatric Orthopedics, Hospital Regional de Alta hyper laxity of severe joints, athetoid movements, scoliosis and Especialidad del Bajio, Mexico severe deformities of the foot. Epidemiology in Latin America is unknown because of its underdiagnosis and when confused *Corresponding author: Jesus Guerra Jasso, Hospital with other connective tissue pathologies (Hutchinson-Gilford Regional de Alta Especialidad del Bajio, Boulevard Milenio No. 130. Col, San Carlos la Roncha, C.P. 37660, Guanajuato, syndrome, gerodermic osteodiplasia, even Ehlers-Danlos), the Mexico, Tel: 477-267 2000; Ext-1403; life expectancy of these patients varies according to the degree of Email: penetrance and in the world literature, there are very few reports (about 50), so the diagnosis requires a challenge [2]. Received: January 13, 2017 | Published: March 21, 2017 Clinical Case and thick clamp. -

Synergistic Genetic Interactions Between Pkhd1 and Pkd1 Result in an ARPKD-Like Phenotype in Murine Models
BASIC RESEARCH www.jasn.org Synergistic Genetic Interactions between Pkhd1 and Pkd1 Result in an ARPKD-Like Phenotype in Murine Models Rory J. Olson,1 Katharina Hopp ,2 Harrison Wells,3 Jessica M. Smith,3 Jessica Furtado,1,4 Megan M. Constans,3 Diana L. Escobar,3 Aron M. Geurts,5 Vicente E. Torres,3 and Peter C. Harris 1,3 Due to the number of contributing authors, the affiliations are listed at the end of this article. ABSTRACT Background Autosomal recessive polycystic kidney disease (ARPKD) and autosomal dominant polycystic kidney disease (ADPKD) are genetically distinct, with ADPKD usually caused by the genes PKD1 or PKD2 (encoding polycystin-1 and polycystin-2, respectively) and ARPKD caused by PKHD1 (encoding fibrocys- tin/polyductin [FPC]). Primary cilia have been considered central to PKD pathogenesis due to protein localization and common cystic phenotypes in syndromic ciliopathies, but their relevance is questioned in the simple PKDs. ARPKD’s mild phenotype in murine models versus in humans has hampered investi- gating its pathogenesis. Methods To study the interaction between Pkhd1 and Pkd1, including dosage effects on the phenotype, we generated digenic mouse and rat models and characterized and compared digenic, monogenic, and wild-type phenotypes. Results The genetic interaction was synergistic in both species, with digenic animals exhibiting pheno- types of rapidly progressive PKD and early lethality resembling classic ARPKD. Genetic interaction be- tween Pkhd1 and Pkd1 depended on dosage in the digenic murine models, with no significant enhancement of the monogenic phenotype until a threshold of reduced expression at the second locus was breached. -

Dramatic Nucleolar Dispersion in the Salivary Gland of Schwenkfeldina Sp
www.nature.com/scientificreports OPEN Dramatic nucleolar dispersion in the salivary gland of Schwenkfeldina sp. (Diptera: Sciaridae) José Mariano Amabis & Eduardo Gorab * Micronucleoli are among the structures composing the peculiar scenario of the nucleolus in salivary gland nuclei of dipterans representative of Sciaridae. Micronucleolar bodies contain ribosomal DNA and RNA, are transcriptionally active and may appear free in the nucleoplasm or associated with specifc chromosome regions in salivary gland nuclei. This report deals with an extreme case of nucleolar fragmentation/dispersion detected in the salivary gland of Schwenkfeldina sp. Such a phenomenon in this species was found to be restricted to cell types undergoing polyteny and seems to be diferentially controlled according to the cell type. Furthermore, transcriptional activity was detected in virtually all the micronucleolar bodies generated in the salivary gland. The relative proportion of the rDNA in polytene and diploid tissues showed that rDNA under-replication did not occur in polytene nuclei suggesting that the nucleolar and concomitant rDNA dispersion in Schwenkfeldina sp. may refect a previously hypothesised process in order to counterbalance the rDNA loss due to the under-replication. The chromosomal distribution of epigenetic markers for the heterochromatin agreed with early cytological observations in this species suggesting that heterochromatin is spread throughout the chromosome length of Schwenkfeldina sp. A comparison made with results from another sciarid species argues for a role played by the heterochromatin in the establishment of the rDNA topology in polytene nuclei of Sciaridae. Transcriptional activity of ribosomal RNA (rRNA) genes in specifc chromosome regions is the primary event for the local assembly of the nucleolus, the starting site of ribosome biogenesis. -

The Progeria Syndrome Fact Sheet
HUTCHINSON-GILFORD PROGERIA SYNDROME FREQUENTLY ASKED QUESTIONS WHAT IS PROGERIA? Hutchinson-Gilford Progeria Syndrome “Progeria” or “HGPS” is a rare, fatal genetic condition characterized by an appearance of accelerated aging in children. Its name is derived from the Greek and means "prematurely old." While there are different forms of Progeria*, the classic type is Hutchinson- Gilford Progeria Syndrome, which was named after the doctors who first described it in England: in 1886 by Dr. Jonathan Hutchinson, and in 1897 by Dr. Hastings Gilford. HOW COMMON IS PROGERIA? Progeria affects approximately 1 in 4 - 8 million newborns. It affects both sexes equally and all races. In the past 15 years, children with Progeria have been reported all over the world , including in: Algeria Cuba Ireland Peru Sweden Argentina Denmark Israel Philippines Switzerland Australia Dominican Italy Poland Turkey Austria Republic Japan Portugal United States Belgium Egypt Libya Puerto Rico Venezuela Brazil England Mexico Romania Vietnam Canada France Morocco South Africa Yugoslavia China Germany Netherlands South Korea Columbia India Pakistan Spain WHAT ARE THE FEATURES OF PROGERIA? Although they are born looking healthy, most children with Progeria begin to display many characteristics of Progeria within the first year of life. Progeria signs include growth failure, loss of body fat and hair, aged-looking skin, stiffness of joints, hip dislocation, generalized atherosclerosis, cardiovascular (heart) disease and stroke. The children have a remarkably similar appearance, despite differing ethnic backgrounds. Children with Progeria die of atherosclerosis (heart disease) at an average age of thirteen years (with a range of about 8 – 21 years). WHAT DOES PROGERIA HAVE TO DO WITH AGING? Children with Progeria are genetically predisposed to premature, progressive heart disease. -

Genes in Eyecare Geneseyedoc 3 W.M
Genes in Eyecare geneseyedoc 3 W.M. Lyle and T.D. Williams 15 Mar 04 This information has been gathered from several sources; however, the principal source is V. A. McKusick’s Mendelian Inheritance in Man on CD-ROM. Baltimore, Johns Hopkins University Press, 1998. Other sources include McKusick’s, Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. Baltimore. Johns Hopkins University Press 1998 (12th edition). http://www.ncbi.nlm.nih.gov/Omim See also S.P.Daiger, L.S. Sullivan, and B.J.F. Rossiter Ret Net http://www.sph.uth.tmc.edu/Retnet disease.htm/. Also E.I. Traboulsi’s, Genetic Diseases of the Eye, New York, Oxford University Press, 1998. And Genetics in Primary Eyecare and Clinical Medicine by M.R. Seashore and R.S.Wappner, Appleton and Lange 1996. M. Ridley’s book Genome published in 2000 by Perennial provides additional information. Ridley estimates that we have 60,000 to 80,000 genes. See also R.M. Henig’s book The Monk in the Garden: The Lost and Found Genius of Gregor Mendel, published by Houghton Mifflin in 2001 which tells about the Father of Genetics. The 3rd edition of F. H. Roy’s book Ocular Syndromes and Systemic Diseases published by Lippincott Williams & Wilkins in 2002 facilitates differential diagnosis. Additional information is provided in D. Pavan-Langston’s Manual of Ocular Diagnosis and Therapy (5th edition) published by Lippincott Williams & Wilkins in 2002. M.A. Foote wrote Basic Human Genetics for Medical Writers in the AMWA Journal 2002;17:7-17. A compilation such as this might suggest that one gene = one disease. -
Neurodegeneration in Accelerated Aging
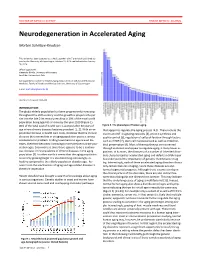
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Trichothiodystrophy
Trichothiodystrophy Author: Doctor Alfredo Rossi1 and Doctor C. Cantisani. Creation date: June 2004 Scientific Editor: Prof Antonella Tosti 1Dipartimento di Malattie Cutanee-Veneree Chirurgia Plastica-Ricostruttiva, Università degli studi di Roma “La Sapienza” Abstract Keywords Definition Epidemiology Etiology Clinical description Diagnostic methods Prenatal diagnosis Management References Abstract Trichothiodystrophy (TTD) is a rare autosomal recessive genetic disorder characterized by abnormal synthesis of the sulphur containing keratins and consequently hair dysplasia, associated with numerous symptoms affecting mainly organs derived from the neuroectoderm. This phenotypic aspect is due to mutations in the DNA-dependent ATPase/helicase subunit of TFIIH, XPB and XPD. Abnormalities in excision repair of ultraviolet (UV)-damaged DNA are recognized in about half of the patients. The clinical appearance is characterized by brittle and fragile hair, congenital ichthyosis, nail and dental dysplasias, cataract, progeria-like face, growth and mental retardation. The abnormalities are usually obvious at birth, with variable clinical expression. The variants of TTD, depending on their different associations, are known by the initials BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, as well as the eponyms of the Pollit, Tay, Sabinas syndromes or Amish brittle hair. The exact prevalence of TTD is unknown, but appears to be rather uncommon. About 20 cases of PIBI(D)S have been reported in the literature. Up to 1991, clinical data of 15 cases with IBIDS were published. Prenatal diagnostic of TTD is available. There is no specific treatment. Keywords Brittle hair, photosensitivity, ichthyosis, BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, Tay-syndrome Definition tail pattern). They named it Trichothiodystrophy, Trichothiodystrophy (TTD) is a group of rare noticing also an increased Photosensitivity and autosomal recessive disorders with heterogenic Ichthyosis in these patients (PIBIDS). -

Functional Analysis of Structural Variation in the 2D and 3D Human Genome
FUNCTIONAL ANALYSIS OF STRUCTURAL VARIATION IN THE 2D AND 3D HUMAN GENOME by Conor Mitchell Liam Nodzak A dissertation submitted to the faculty of The University of North Carolina at Charlotte in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Bioinformatics and Computational Biology Charlotte 2019 Approved by: Dr. Xinghua Mindy Shi Dr. Rebekah Rogers Dr. Jun-tao Guo Dr. Adam Reitzel ii c 2019 Conor Mitchell Liam Nodzak ALL RIGHTS RESERVED iii ABSTRACT CONOR MITCHELL LIAM NODZAK. Functional analysis of structural variation in the 2D and 3D human genome. (Under the direction of DR. XINGHUA MINDY SHI) The human genome consists of over 3 billion nucleotides that have an average distance of 3.4 Angstroms between each base, which equates to over two meters of DNA contained within the 125 µm3 volume diploid cell nuclei. The dense compaction of chromatin by the supercoiling of DNA forms distinct architectural modules called topologically associated domains (TADs), which keep protein-coding genes, noncoding RNAs and epigenetic regulatory elements in close nuclear space. It has recently been shown that these conserved chromatin structures may contribute to tissue-specific gene expression through the encapsulation of genes and cis-regulatory elements, and mutations that affect TADs can lead to developmental disorders and some forms of cancer. At the population-level, genomic structural variation contributes more to cumulative genetic difference than any other class of mutation, yet much remains to be studied as to how structural variation affects TADs. Here, we study the func- tional effects of structural variants (SVs) through the analysis of chromatin topology and gene activity for three trio families sampled from genetically diverse popula- tions from the Human Genome Structural Variation Consortium. -

Clinical Diagnostic Whole Exome Sequencing for Infants in Intensive Care Settings: Outcomes Analysis and Economic Evaluation
The Texas Medical Center Library DigitalCommons@TMC UT School of Public Health Dissertations (Open Access) School of Public Health Summer 5-2019 CLINICAL DIAGNOSTIC WHOLE EXOME SEQUENCING FOR INFANTS IN INTENSIVE CARE SETTINGS: OUTCOMES ANALYSIS AND ECONOMIC EVALUATION HADLEY STEVENS SMITH UTHealth School of Public Health Follow this and additional works at: https://digitalcommons.library.tmc.edu/uthsph_dissertsopen Part of the Community Psychology Commons, Health Psychology Commons, and the Public Health Commons Recommended Citation SMITH, HADLEY STEVENS, "CLINICAL DIAGNOSTIC WHOLE EXOME SEQUENCING FOR INFANTS IN INTENSIVE CARE SETTINGS: OUTCOMES ANALYSIS AND ECONOMIC EVALUATION" (2019). UT School of Public Health Dissertations (Open Access). 106. https://digitalcommons.library.tmc.edu/uthsph_dissertsopen/106 This is brought to you for free and open access by the School of Public Health at DigitalCommons@TMC. It has been accepted for inclusion in UT School of Public Health Dissertations (Open Access) by an authorized administrator of DigitalCommons@TMC. For more information, please contact [email protected]. CLINICAL DIAGNOSTIC WHOLE EXOME SEQUENCING FOR INFANTS IN INTENSIVE CARE SETTINGS: OUTCOMES ANALYSIS AND ECONOMIC EVALUATION by HADLEY STEVENS SMITH, MPSA, BS APPROVED: J. MICHAEL SWINT, PHD SEEMA R. LALANI, MD MARCIA C. DE OLIVEIRA OTTO, PHD HEIDI V. RUSSELL, MD, PHD JOSE-MIGUEL YAMAL, PHD DEAN, THE UNIVERSITY OF TEXAS SCHOOL OF PUBLIC HEALTH Copyright by Hadley Stevens Smith, PhD, MPSA, BS 2019 CLINICAL DIAGNOSTIC WHOLE -

1. Progeria 101: Frequently Asked Questions
1. PROGERIA 101: FREQUENTLY ASKED QUESTIONS 1. Progeria 101: Frequently Asked Questions What is Hutchinson-Gilford Progeria Syndrome? What is PRF’s history and mission? What causes Progeria? How is Progeria diagnosed? Are there different types of Progeria? Is Progeria contagious or inherited? What is Hutchinson-Gilford Progeria Syndrome (HGPS or Progeria)? Progeria is also known as Hutchinson-Gilford Progeria Syndrome (HGPS). Genetic testing for It was first described in 1886 by Dr. Jonathan Hutchinson and in 1897 by Progeria can be Dr. Hastings Gilford. Progeria is a rare, fatal, “premature aging” syndrome. It’s called a syndrome performed from a because all the children have very similar symptoms that “go together”. The small sample of blood children have a remarkably similar appearance, even though Progeria affects children of all different ethnic backgrounds. Although most babies with (1-2 tsp) or sometimes Progeria are born looking healthy, they begin to display many characteristics from a sample of saliva. of accelerated aging by 18-24 months of age, or even earlier. Progeria signs include growth failure, loss of body fat and hair, skin changes, stiffness of joints, hip dislocation, generalized atherosclerosis, cardiovascular (heart) disease, and stroke. Children with Progeria die of atherosclerosis (heart disease) or stroke at an average age of 13 years (with a range of about 8-21 years). Remarkably, the intellect of children with Progeria is unaffected, and despite the physical changes in their young bodies, these extraordinary children are intelligent, courageous, and full of life. 1.2 THE PROGERIA HANDBOOK What is PRF’s history and mission? The Progeria Research Foundation (PRF) was established in the United States in 1999 by the parents of a child with Progeria, Drs. -

Werner and Hutchinson–Gilford Progeria Syndromes: Mechanistic Basis of Human Progeroid Diseases
REVIEWS MECHANISMS OF DISEASE Werner and Hutchinson–Gilford progeria syndromes: mechanistic basis of human progeroid diseases Brian A. Kudlow*¶, Brian K. Kennedy* and Raymond J. Monnat Jr‡§ Abstract | Progeroid syndromes have been the focus of intense research in part because they might provide a window into the pathology of normal ageing. Werner syndrome and Hutchinson–Gilford progeria syndrome are two of the best characterized human progeroid diseases. Mutated genes that are associated with these syndromes have been identified, mouse models of disease have been developed, and molecular studies have implicated decreased cell proliferation and altered DNA-damage responses as common causal mechanisms in the pathogenesis of both diseases. Progeroid syndromes are heritable human disorders with therefore termed segmental, as opposed to global, features that suggest premature ageing1. These syndromes progeroid syndromes. Among the segmental progeroid have been well characterized as clinical disease entities, syndromes, the syndromes that most closely recapitu- and in many instances the associated genes and causative late the features of human ageing are Werner syndrome mutations have been identified. The identification of (WS), Hutchinson–Gilford progeria syndrome (HGPS), genes that are associated with premature-ageing-like Cockayne syndrome, ataxia-telangiectasia, and the con- syndromes has increased our understanding of molecu- stitutional chromosomal disorders of Down, Klinefelter lar pathways that protect cell viability and function, and -

DNA Replication Timing Alterations Identify Common Markers Between Distinct Progeroid Diseases
DNA replication timing alterations identify common PNAS PLUS markers between distinct progeroid diseases Juan Carlos Rivera-Muliaa, Romain Despratb, Claudia Trevilla-Garciaa, Daniela Cornacchiac, Hélène Schwererd, Takayo Sasakia, Jiao Simaa, Tyler Fellsa, Lorenz Studerc, Jean-Marc Lemaitreb,d,1, and David M. Gilberta,e,1 aDepartment of Biological Science, Florida State University, Tallahassee, FL 32306; bPlateforme de Reprogrammation Cellulaire (SAFE-iPSC) Stem Cell Core Facility, Infrastructure Nationale d’Ingénierie des Cellules Souches Pluripotentes et Cellules Différenciées (INGESTEM), Centres Hospitaliers Universitaires de Montpellier, Hopital Saint Eloi, F3400 Montpellier, France; cThe Center for Stem Cell Biology, Memorial Sloan-Kettering Institute, New York, NY 10065; dInstitute of Regenerative Medicine and Biotherapies, U1183 INSERM, Université de Montpellier, F3400 Montpellier, France; and eCenter for Genomics and Personalized Medicine, Florida State University, Tallahassee, FL 32306 Edited by Terry L. Orr-Weaver, Whitehead Institute, Cambridge, MA, and approved November 8, 2017 (received for review June 30, 2017) Progeroid syndromes are rare genetic disorders that phenotypi- the mechanisms linking the cellular defects to pathophysiological cally resemble natural aging. Different causal mutations have been manifestations of the disease. identified, but no molecular alterations have been identified that Previously, we demonstrated that the temporal order of ge- are in common to these diseases. DNA replication timing (RT) is a