Metabolic Dysfunction in Hutchinson–Gilford Progeria Syndrome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

De Barsy Syndrome: Orthopedic Case Report and Literature Review
MOJ Orthopedics & Rheumatology De Barsy Syndrome: Orthopedic Case report and Literature Review Introduction Case Report Volume 7 Issue 5 - 2017 This condition was first described in 1968 by De Barsy who and degeneration of the elastic tissue of the cornea and skin, Jose de Jesus Guerra Jasso1*, Douglas reported a case of a patient with progeria, dwarfism, oligofrenia and since then, it is known as Barsy Syndrome or Barsy- Colmenares Bonilla2 and Loreett Ocampo Perez3 of progeroid aspect, cutis laxa, corneal opacity, intrauterine 1Pediatric Orthopedics, Hospital Regional de Alta Especialidad growthMoens-Dierckx retardation Syndrome. and severe This ismental defined retardation as the combination (although del Bajio, Mexico some will learn to speak, intelligence is less than normal) [1]. 2Pediatric Orthopedic Service, Hospital regional de alta especialidad del bajio The orthopedic manifestations are dysplasia of hip development, 3Fellow of Pediatric Orthopedics, Hospital Regional de Alta hyper laxity of severe joints, athetoid movements, scoliosis and Especialidad del Bajio, Mexico severe deformities of the foot. Epidemiology in Latin America is unknown because of its underdiagnosis and when confused *Corresponding author: Jesus Guerra Jasso, Hospital with other connective tissue pathologies (Hutchinson-Gilford Regional de Alta Especialidad del Bajio, Boulevard Milenio No. 130. Col, San Carlos la Roncha, C.P. 37660, Guanajuato, syndrome, gerodermic osteodiplasia, even Ehlers-Danlos), the Mexico, Tel: 477-267 2000; Ext-1403; life expectancy of these patients varies according to the degree of Email: penetrance and in the world literature, there are very few reports (about 50), so the diagnosis requires a challenge [2]. Received: January 13, 2017 | Published: March 21, 2017 Clinical Case and thick clamp. -

The Progeria Syndrome Fact Sheet
HUTCHINSON-GILFORD PROGERIA SYNDROME FREQUENTLY ASKED QUESTIONS WHAT IS PROGERIA? Hutchinson-Gilford Progeria Syndrome “Progeria” or “HGPS” is a rare, fatal genetic condition characterized by an appearance of accelerated aging in children. Its name is derived from the Greek and means "prematurely old." While there are different forms of Progeria*, the classic type is Hutchinson- Gilford Progeria Syndrome, which was named after the doctors who first described it in England: in 1886 by Dr. Jonathan Hutchinson, and in 1897 by Dr. Hastings Gilford. HOW COMMON IS PROGERIA? Progeria affects approximately 1 in 4 - 8 million newborns. It affects both sexes equally and all races. In the past 15 years, children with Progeria have been reported all over the world , including in: Algeria Cuba Ireland Peru Sweden Argentina Denmark Israel Philippines Switzerland Australia Dominican Italy Poland Turkey Austria Republic Japan Portugal United States Belgium Egypt Libya Puerto Rico Venezuela Brazil England Mexico Romania Vietnam Canada France Morocco South Africa Yugoslavia China Germany Netherlands South Korea Columbia India Pakistan Spain WHAT ARE THE FEATURES OF PROGERIA? Although they are born looking healthy, most children with Progeria begin to display many characteristics of Progeria within the first year of life. Progeria signs include growth failure, loss of body fat and hair, aged-looking skin, stiffness of joints, hip dislocation, generalized atherosclerosis, cardiovascular (heart) disease and stroke. The children have a remarkably similar appearance, despite differing ethnic backgrounds. Children with Progeria die of atherosclerosis (heart disease) at an average age of thirteen years (with a range of about 8 – 21 years). WHAT DOES PROGERIA HAVE TO DO WITH AGING? Children with Progeria are genetically predisposed to premature, progressive heart disease. -

Progerinin, an Optimized Progerin-Lamin a Binding Inhibitor
ARTICLE https://doi.org/10.1038/s42003-020-01540-w OPEN Progerinin, an optimized progerin-lamin A binding inhibitor, ameliorates premature senescence phenotypes of Hutchinson-Gilford progeria syndrome 1234567890():,; So-mi Kang1,7, Min-Ho Yoon1,7, Jinsook Ahn2, Ji-Eun Kim3, So Young Kim4, Seock Yong Kang4, Jeongmin Joo4, Soyoung Park1, Jung-Hyun Cho1, Tae-Gyun Woo1, Ah-Young Oh1, Kyu Jin Chung3, So Yon An5, ✉ Tae Sung Hwang5, Soo Yong Lee6, Jeong-Su Kim6, Nam-Chul Ha2, Gyu-Yong Song3 & Bum-Joon Park 1 Previous work has revealed that progerin-lamin A binding inhibitor (JH4) can ameliorate pathological features of Hutchinson-Gilford progeria syndrome (HGPS) such as nuclear deformation, growth suppression in patient’s cells, and very short life span in an in vivo mouse model. Despite its favorable effects, JH4 is rapidly eliminated in in vivo pharmaco- kinetic (PK) analysis. Thus, we improved its property through chemical modification and obtained an optimized drug candidate, Progerinin (SLC-D011). This chemical can extend the life span of LmnaG609G/G609G mouse for about 10 weeks and increase its body weight. Progerinin can also extend the life span of LmnaG609G/+ mouse for about 14 weeks via oral administration, whereas treatment with lonafarnib (farnesyl-transferase inhibitor) can only extend the life span of LmnaG609G/+ mouse for about two weeks. In addition, progerinin can induce histological and physiological improvement in LmnaG609G/+ mouse. These results indicate that progerinin is a strong drug candidate for HGPS. 1 Department of Molecular Biology, College of Natural Science, Pusan National University, Busan, Korea. 2 Department of Food Science, College of Agricultural Science, Seoul National University, Seoul, Korea. -

Alterations in Mitosis and Cell Cycle Progression Caused by a Mutant Lamin a Known to Accelerate Human Aging
Alterations in mitosis and cell cycle progression caused by a mutant lamin A known to accelerate human aging Thomas Dechat*, Takeshi Shimi*, Stephen A. Adam*, Antonio E. Rusinol†, Douglas A. Andres‡, H. Peter Spielmann‡§¶, Michael S. Sinensky†, and Robert D. Goldman*ʈ *Department of Cell and Molecular Biology, Feinberg School of Medicine, Northwestern University, 303 East Chicago Avenue, Chicago, IL 60611; †Department of Biochemistry and Molecular Biology, James H. Quillen College of Medicine, East Tennessee State University, Box 70581, Johnson City, TN 37614; and Departments of ‡Molecular and Cellular Biochemistry and §Chemistry and ¶Kentucky Center for Structural Biology, University of Kentucky, 741 South Limestone, Lexington, KY 40536 Communicated by Francis S. Collins, National Institutes of Health, Bethesda, MD, February 2, 2007 (received for review December 19, 2006) Mutations in the gene encoding nuclear lamin A (LA) cause the DNA repair defects, changes in histone methylation, and loss of premature aging disease Hutchinson–Gilford Progeria Syndrome. heterochromatin (5, 17–19). However, the impact of LA⌬50/ The most common of these mutations results in the expression of progerin on mitosis and its consequences for daughter cells a mutant LA, with a 50-aa deletion within its C terminus. In this entering G1 have not been determined. An initial insight into study, we demonstrate that this deletion leads to a stable farne- changes in early G1 came from studies of HeLa cells expressing sylation and carboxymethylation of the mutant LA (LA⌬50/prog- GFP-LA⌬50/progerin, in which this mutant protein is abnor- erin). These modifications cause an abnormal association of LA⌬50/ mally retained in cytoplasmic structures after nuclear assembly progerin with membranes during mitosis, which delays the onset is completed (5). -
Neurodegeneration in Accelerated Aging
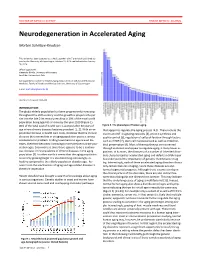
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Trichothiodystrophy
Trichothiodystrophy Author: Doctor Alfredo Rossi1 and Doctor C. Cantisani. Creation date: June 2004 Scientific Editor: Prof Antonella Tosti 1Dipartimento di Malattie Cutanee-Veneree Chirurgia Plastica-Ricostruttiva, Università degli studi di Roma “La Sapienza” Abstract Keywords Definition Epidemiology Etiology Clinical description Diagnostic methods Prenatal diagnosis Management References Abstract Trichothiodystrophy (TTD) is a rare autosomal recessive genetic disorder characterized by abnormal synthesis of the sulphur containing keratins and consequently hair dysplasia, associated with numerous symptoms affecting mainly organs derived from the neuroectoderm. This phenotypic aspect is due to mutations in the DNA-dependent ATPase/helicase subunit of TFIIH, XPB and XPD. Abnormalities in excision repair of ultraviolet (UV)-damaged DNA are recognized in about half of the patients. The clinical appearance is characterized by brittle and fragile hair, congenital ichthyosis, nail and dental dysplasias, cataract, progeria-like face, growth and mental retardation. The abnormalities are usually obvious at birth, with variable clinical expression. The variants of TTD, depending on their different associations, are known by the initials BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, as well as the eponyms of the Pollit, Tay, Sabinas syndromes or Amish brittle hair. The exact prevalence of TTD is unknown, but appears to be rather uncommon. About 20 cases of PIBI(D)S have been reported in the literature. Up to 1991, clinical data of 15 cases with IBIDS were published. Prenatal diagnostic of TTD is available. There is no specific treatment. Keywords Brittle hair, photosensitivity, ichthyosis, BIDS, IBIDS, PIBIDS, SIBIDS, ONMRS, Tay-syndrome Definition tail pattern). They named it Trichothiodystrophy, Trichothiodystrophy (TTD) is a group of rare noticing also an increased Photosensitivity and autosomal recessive disorders with heterogenic Ichthyosis in these patients (PIBIDS). -

1. Progeria 101: Frequently Asked Questions
1. PROGERIA 101: FREQUENTLY ASKED QUESTIONS 1. Progeria 101: Frequently Asked Questions What is Hutchinson-Gilford Progeria Syndrome? What is PRF’s history and mission? What causes Progeria? How is Progeria diagnosed? Are there different types of Progeria? Is Progeria contagious or inherited? What is Hutchinson-Gilford Progeria Syndrome (HGPS or Progeria)? Progeria is also known as Hutchinson-Gilford Progeria Syndrome (HGPS). Genetic testing for It was first described in 1886 by Dr. Jonathan Hutchinson and in 1897 by Progeria can be Dr. Hastings Gilford. Progeria is a rare, fatal, “premature aging” syndrome. It’s called a syndrome performed from a because all the children have very similar symptoms that “go together”. The small sample of blood children have a remarkably similar appearance, even though Progeria affects children of all different ethnic backgrounds. Although most babies with (1-2 tsp) or sometimes Progeria are born looking healthy, they begin to display many characteristics from a sample of saliva. of accelerated aging by 18-24 months of age, or even earlier. Progeria signs include growth failure, loss of body fat and hair, skin changes, stiffness of joints, hip dislocation, generalized atherosclerosis, cardiovascular (heart) disease, and stroke. Children with Progeria die of atherosclerosis (heart disease) or stroke at an average age of 13 years (with a range of about 8-21 years). Remarkably, the intellect of children with Progeria is unaffected, and despite the physical changes in their young bodies, these extraordinary children are intelligent, courageous, and full of life. 1.2 THE PROGERIA HANDBOOK What is PRF’s history and mission? The Progeria Research Foundation (PRF) was established in the United States in 1999 by the parents of a child with Progeria, Drs. -

Expression of Progerin Does Not Result in an Increased Mutation Rate
bioRxiv preprint doi: https://doi.org/10.1101/047506; this version posted April 6, 2016. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Expression of progerin does not result in an increased mutation rate. Emmanuelle Deniaud1, Shelagh Boyle1 and Wendy A. Bickmore1* 1 MRC Human Genetics Unit, MRC Institute of Genetics and Molecular Medicine at the University of Edinburgh, Crewe Road, Edinburgh EH4 2XU, UK *Correspondence to: Wendy Bickmore, MRC Human Genetics Unit, IGMM, Crewe Road, Edinburgh EH4 2XU, UK Email:[email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/047506; this version posted April 6, 2016. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Abstract In the premature ageing disease Hutchinson-Gilford progeria syndrome (HGPS) the underlying genetic defect in the lamin A gene leads to accumulation at the nuclear lamina of progerin – a mutant form of lamin A that cannot be correctly processed. This has been reported to result in defects in the DNA damage response and in DNA repair, leading to the hypothesis that, as in normal ageing and in other progeroid syndromes caused by mutation of genes of the DNA repair and DNA damage response pathways, increased DNA damage may be responsible for the premature ageing phenotypes in HGPS patients. -

Inhibiting Farnesylation Reverses the Nuclear Morphology Defect in a Hela Cell Model for Hutchinson–Gilford Progeria Syndrome
Inhibiting farnesylation reverses the nuclear morphology defect in a HeLa cell model for Hutchinson–Gilford progeria syndrome Monica P. Mallampalli*, Gregory Huyer*, Pravin Bendale†, Michael H. Gelb†, and Susan Michaelis*‡ *Department of Cell Biology, Johns Hopkins University School of Medicine, Baltimore, MD 21205; and †Departments of Chemistry and Biochemistry, University of Washington, Seattle, WA 98195 Edited by Carol W. Greider, Johns Hopkins University School of Medicine, Baltimore, MD, and approved August 23, 2005 (received for review May 6, 2005) Hutchinson–Gilford progeria syndrome (HGPS) is a devastating event between Y646 and L647 mediated by zinc metalloprotease premature aging disease resulting from a mutation in the LMNA Ste24 (Zmpste24) removes the C-terminal 15 aa, including the gene, which encodes nuclear lamins A and C. Lamin A is synthe- farnesyl and carboxylmethyl CaaX modifications (Fig. 1A, step sized as a precursor (prelamin A) with a C-terminal CaaX motif that 4) (8–10). Zmpste24 is a protease in the endoplasmic reticulum undergoes farnesylation, endoproteolytic cleavage, and carboxyl- membrane and was first identified in budding yeast, where it methylation. Prelamin A is subsequently internally cleaved by the catalyzes aaXing (in which it is functionally redundant with zinc metalloprotease Ste24 (Zmpste24) protease, which removes Rce1) and an internal cleavage in the a-factor mating phero- the 15 C-terminal amino acids, including the CaaX modifications, to mone, as also occurs in prelamin A (11–13). Lamin B, like lamin yield mature lamin A. HGPS results from a dominant mutant form A, undergoes CaaX modifications; however, notably, lamin B is of prelamin A (progerin) that has an internal deletion of 50 aa near not internally cleaved. -

Werner and Hutchinson–Gilford Progeria Syndromes: Mechanistic Basis of Human Progeroid Diseases
REVIEWS MECHANISMS OF DISEASE Werner and Hutchinson–Gilford progeria syndromes: mechanistic basis of human progeroid diseases Brian A. Kudlow*¶, Brian K. Kennedy* and Raymond J. Monnat Jr‡§ Abstract | Progeroid syndromes have been the focus of intense research in part because they might provide a window into the pathology of normal ageing. Werner syndrome and Hutchinson–Gilford progeria syndrome are two of the best characterized human progeroid diseases. Mutated genes that are associated with these syndromes have been identified, mouse models of disease have been developed, and molecular studies have implicated decreased cell proliferation and altered DNA-damage responses as common causal mechanisms in the pathogenesis of both diseases. Progeroid syndromes are heritable human disorders with therefore termed segmental, as opposed to global, features that suggest premature ageing1. These syndromes progeroid syndromes. Among the segmental progeroid have been well characterized as clinical disease entities, syndromes, the syndromes that most closely recapitu- and in many instances the associated genes and causative late the features of human ageing are Werner syndrome mutations have been identified. The identification of (WS), Hutchinson–Gilford progeria syndrome (HGPS), genes that are associated with premature-ageing-like Cockayne syndrome, ataxia-telangiectasia, and the con- syndromes has increased our understanding of molecu- stitutional chromosomal disorders of Down, Klinefelter lar pathways that protect cell viability and function, and -

DNA Replication Timing Alterations Identify Common Markers Between Distinct Progeroid Diseases
DNA replication timing alterations identify common PNAS PLUS markers between distinct progeroid diseases Juan Carlos Rivera-Muliaa, Romain Despratb, Claudia Trevilla-Garciaa, Daniela Cornacchiac, Hélène Schwererd, Takayo Sasakia, Jiao Simaa, Tyler Fellsa, Lorenz Studerc, Jean-Marc Lemaitreb,d,1, and David M. Gilberta,e,1 aDepartment of Biological Science, Florida State University, Tallahassee, FL 32306; bPlateforme de Reprogrammation Cellulaire (SAFE-iPSC) Stem Cell Core Facility, Infrastructure Nationale d’Ingénierie des Cellules Souches Pluripotentes et Cellules Différenciées (INGESTEM), Centres Hospitaliers Universitaires de Montpellier, Hopital Saint Eloi, F3400 Montpellier, France; cThe Center for Stem Cell Biology, Memorial Sloan-Kettering Institute, New York, NY 10065; dInstitute of Regenerative Medicine and Biotherapies, U1183 INSERM, Université de Montpellier, F3400 Montpellier, France; and eCenter for Genomics and Personalized Medicine, Florida State University, Tallahassee, FL 32306 Edited by Terry L. Orr-Weaver, Whitehead Institute, Cambridge, MA, and approved November 8, 2017 (received for review June 30, 2017) Progeroid syndromes are rare genetic disorders that phenotypi- the mechanisms linking the cellular defects to pathophysiological cally resemble natural aging. Different causal mutations have been manifestations of the disease. identified, but no molecular alterations have been identified that Previously, we demonstrated that the temporal order of ge- are in common to these diseases. DNA replication timing (RT) is a -

Progeria Syndromes and Ageing: What Is the Connection?
REVIEWS Progeria syndromes and ageing: what is the connection? Christopher R. Burtner* and Brian K. Kennedy*‡§ Abstract | One of the many debated topics in ageing research is whether progeroid syndromes are really accelerated forms of human ageing. The answer requires a better understanding of the normal ageing process and the molecular pathology underlying these rare diseases. Exciting recent findings regarding a severe human progeria, Hutchinson–Gilford progeria syndrome, have implicated molecular changes that are also linked to normal ageing, such as genome instability, telomere attrition, premature senescence and defective stem cell homeostasis in disease development. These observations, coupled with genetic studies of longevity, lead to a hypothesis whereby progeria syndromes accelerate a subset of the pathological changes that together drive the normal ageing process. Ageing studies have long shown that organismal lifespan model systems and those associated with progerias in is a modifiable parameter. The classical example is diet mammals have at best limited overlap (FIG. 1). ary restriction1,2, which extends longevity in a growing In this Review, we combine recent developments in number of organisms, including yeast (Saccharomyces the branch of ageing research that focuses on lifespan cerevisiae)3–5, worms (Caenorhabditis elegans)6, fruit flies extension of diseasefree individuals with advancements (Drosophila melanogaster)7,8, rodents9 and, most recently, made towards understanding the pathology of human rhesus monkeys (Macaca mulatta)10. This suggests that progerias, particularly regading Hutchinson–Gilford molecular events contributing to the pathophysiology of progeria syndrome (HGPS). This Review is not exhaus cellular ageing are shared to some degree among widely tive with respect to these complex topics, but rather is diverse systems, an assertion verified in a direct quantita directed towards describing the essentials while point tive comparison between two disparate invertebrates11.