Supplemental Information
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rhinitis and Sinusitis
Glendale Animal Hospital 623-934-7243 www.familyvet.com Rhinitis and Sinusitis (Inflammation of the Nose and Sinuses) Basics OVERVIEW Rhinitis—inflammation of the lining of the nose Sinusitis—inflammation of the sinuses The nasal cavity communicates directly with the sinuses; thus inflammation of the nose (rhinitis) and inflammation of the sinuses (sinusitis) often occur together (known as “rhinosinusitis”) “Upper respiratory tract” (also known as the “upper airways”) includes the nose, nasal passages, throat (pharynx), and windpipe (trachea) “Lower respiratory tract” (also known as the “lower airways”) includes the bronchi, bronchioles, and alveoli (the terminal portion of the airways, in which oxygen and carbon dioxide are exchanged) SIGNALMENT/DESCRIPTION OF PET Species Dogs Cats Breed Predilections Short-nosed, flat-faced (known as “brachycephalic”) cats are more prone to long-term (chronic) inflammation of the nose (rhinitis), and possibly fungal rhinitis Dogs with a long head and nose (known as “dolichocephalic dogs,” such as the collie and Afghan hound) are more prone to Aspergillus (a type of fungus) infection and nasal tumors Mean Age and Range Cats—sudden (acute) viral inflammation of the nose and sinuses (rhinosinusitis) and red masses in the nasal cavity and throat (known as “nasopharyngeal polyps”) are more common in young kittens (6–12 weeks of age) Congenital (present at birth) diseases (such as cleft palate) are more common in young pets Tumors/cancer and dental disease—are more common in older pets Foreign -

Laryngitis from Reflux: Prevention for the Performing Singer
Laryngitis from Reflux: Prevention for the Performing Singer David G. Hanson, MD, FACS Jack J. Jiang, MD, PhD Laryngitis in General Laryngitis is the bane of performers and other professionals who depend on their voice for their art and livelihood. Almost every person has experienced acute laryngitis, usually associated with a viral upper- respiratory infection. Whenever there is inflammation of the vocal fold epithelium, there is an effect on voice quality and strength. Therefore, it is important to understand the factors that can cause laryngitis, especially the preventable causes of laryngitis. Laryngitis is a generic term for inflammation or irritation of the laryngeal tissues. The inflammation can be caused by any kind of injury, including infection, smoking, contact with caustic or acidic substance, allergic reaction, or direct trauma. Inflammatory response of the tissues includes leakage of fluid from blood vessels with edema or swelling, congregation of white blood cells, which release mediators of inflammation, and engorgement of the blood vessels. Most commonly laryngitis occurs from viral infection of the laryngeal epithelial lining associated with a typical cold. The viral infection is almost always quickly conquered by the body's immune system and lasts at most a few days. This kind of acute laryngitis rarely causes any long-term problem unless the vocal folds are damaged by overuse during the illness. Examination of the larynx will show whether the vocal folds are inflamed and allows some prediction of the degree of risk for damage. Other infections of the larynx are fortunately not common but include infections with bacteria and other organisms. -

Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1
ISSN: 2572-4193 Gelpi et al. J Otolaryngol Rhinol 2018, 4:036 DOI: 10.23937/2572-4193.1510036 Volume 4 | Issue 1 Journal of Open Access Otolaryngology and Rhinology CASE REPORT Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1 1 Check for University Hospitals Cleveland Medical Center, USA updates 2Case Western Reserve University School of Medicine, USA *Corresponding author: Mark Gelpi, MD, University Hospitals Cleveland Medical Center, 11100 Euclid Avenue, Cleveland, OH 44106, USA, Tel: (216)-844-8433, Fax: (216)-201-4479, E-mail: [email protected] paranasal sinuses [1,4]. Nasal symptoms in CF patients Abstract occur early, manifesting between 5-14 years of age, and Cystic fibrosis (CF) is a multisystem disease that can have represent a life-long problem in this population [5]. Pa- significant sinonasal manifestations. Viscous secretions are one of several factors in CF that result in chronic sinona- tients with CF can develop thick nasal secretions con- sal pathology, such as sinusitis, polyposis, congestion, and tributing to chronic rhinosinusitis (CRS), nasal conges- obstructive crusting. Persistent discomfort and nasal man- tion, nasal polyposis, headaches, and hyposmia [6-8]. ifestations of this disease significantly affect quality of life. Sinonasal symptoms of CF are managed medically with Digital manipulation and removal of crusting by the patient in an attempt to alleviate the discomfort can have unfore- topical agents and antibiotics, however surgery can be seen damaging consequences. We present one such case warranted due to the chronic and refractory nature of and investigate other cases of septal damage secondary to the symptoms, with 20-25% of CF patients undergoing digital trauma, as well as discuss the importance of sinona- sinus surgery in their lifetime [8]. -

Problems in Family Practice
problems in Family Practice Coughing in Childhood Hyman Sh ran d , M D Cambridge, M assachusetts Coughing in childhood is a common complaint involving a wide spectrum of underlying causes which require a thorough and rational approach by the physician. Most children who cough have relatively simple self-limiting viral infections, but some may have serious disease. A dry environment, allergic factors, cystic fibrosis, and other major illnesses must always be excluded. A simple clinical approach, and the sensible use of appropriate investigations, is most likely to succeed in finding the cause, which can allow precise management. The cough reflex as part of the defense mechanism of the respiratory tract is initiated by mucosal changes, secretions or foreign material in the pharynx, larynx, tracheobronchial Table 1. Persistent Cough — Causes in Childhood* tree, pleura, or ear. Acting as the “watchdog of the lungs,” the “good” cough prevents harmful agents from Common Uncommon Rare entering the respiratory tract; it also helps bring up irritant material from Environmental Overheating with low humidity the airway. The “bad” cough, on the Allergens other hand, serves no useful purpose Pollution Tobacco smoke and, if persistent, causes fatigue, keeps Upper Respiratory Tract the child (and parents) awake, inter Recurrent viral URI Pertussis Laryngeal stridor feres with feeding, and induces vomit Rhinitis, Pharyngitis Echo 12 Vocal cord palsy Allergic rhinitis Nasal polyp Vascular ring ing. It is best suppressed. Coughs and Prolonged use of nose drops Wax in ear colds constitute almost three quarters Sinusitis of all illness in young children. The Lower Respiratory Tract Asthma Cystic fibrosis Rt. -

SINUSITIS AS a CAUSE of TONSILLITIS. by BEDFORD RUSSELL, F.R.C.S., Surgeon-In-Charge, Throat Departmentt, St
Postgrad Med J: first published as 10.1136/pgmj.9.89.80 on 1 March 1933. Downloaded from 80 POST-GRADUATE MEDICAL JOURNAL March, 1933 Plastic Surgery: A short course of lecture-demonstrations is being arranged, to be given at the Hammersmith Hospitar, by Sir Harold Gillies, Mr. MacIndoe and Mr. Kilner. Details will be circulated shortly. Technique of Operations: A series of demonstrations is being arranged. Details will be circulated shortly. Demonstrations in (Advanced) Medicine and Surgeryi A series of weekly demonstrations is being arranged. Details will be circulated shortly. A Guide Book, giving details of how to reach the various London Hospitals by tube, tram, or bus, can be obtained from the Fellowship. Price 6d. (Members and Associates, 3d.). SINUSITIS AS A CAUSE OF TONSILLITIS. BY BEDFORD RUSSELL, F.R.C.S., Surgeon-in-Charge, Throat Departmentt, St. Bart's Hospital. ALTHOUGH the existence of sinus-infection has long since been recognized, medical men whose work lies chiefly in the treatment of disease in the nose, throat and ear are frequently struck with the number of cases of sinusitis which have escaped recognition,copyright. even in the presence of symptoms and signs which should have given rise at least to suspicion of such disease. The explanation of the failure to recognize any but the most mlianifest cases of sinusitis lies, 1 think, in the extreme youth of this branch of medicine; for although operations upon the nose were undoubtedly performed thousands of years ago, it was not uintil the adoption of cocaine about forty years ago that it was even to examine the nasal cavities really critically. -

Asthma Exacerbation Management
CLINICAL PATHWAY ASTHMA EXACERBATION MANAGEMENT TABLE OF CONTENTS Figure 1. Algorithm for Asthma Exacerbation Management – Outpatient Clinic Figure 2. Algorithm for Asthma Management – Emergency Department Figure 3. Algorithm for Asthma Management – Inpatient Figure 4. Progression through the Bronchodilator Weaning Protocol Table 1. Pediatric Asthma Severity (PAS) Score Table 2. Bronchodilator Weaning Protocol Target Population Clinical Management Clinical Assessment Treatment Clinical Care Guidelines for Treatment of Asthma Exacerbations Children’s Hospital Colorado High Risk Asthma Program Table 3. Dosage of Daily Controller Medication for Asthma Control Table 4. Dosage of Medications for Asthma Exacerbations Table 5. Dexamethasone Dosing Guide for Asthma Figure 5. Algorithm for Dexamethasone Dosing – Inpatient Asthma Patient | Caregiver Education Materials Appendix A. Asthma Management – Outpatient Appendix B. Asthma Stepwise Approach (aka STEPs) Appendix C. Asthma Education Handout References Clinical Improvement Team Page 1 of 24 CLINICAL PATHWAY FIGURE 1. ALGORITHM FOR ASTHMA EXACERBATION MANAGEMENT – OUTPATIENT CLINIC Triage RN/MA: • Check HR, RR, temp, pulse ox. Triage level as appropriate • Notify attending physician if patient in severe distress (RR greater than 35, oxygen saturation less than 90%, speaks in single words/trouble breathing at rest) Primary RN: • Give oxygen to keep pulse oximetry greater than 90% Treatment Inclusion Criteria 1. Give nebulized or MDI3 albuterol up to 3 doses. Albuterol dosing is 0.15 to 0.3mg/kg per 2007 • 2 years or older NHLBI guidelines. • Treated for asthma or asthma • Less than 20 kg: 2.5 mg neb x 3 or 2 to 4 puffs MDI albuterol x 3 exacerbation • 20 kg or greater: 5 mg neb x 3 or 4 to 8 puffs MDI albuterol x 3 • First time wheeze with history consistent Note: For moderate (dyspnea interferes with activities)/severe (dyspnea at rest) exacerbations you with asthma can add atrovent to nebulized albuterol at 0.5mg/neb x 3. -
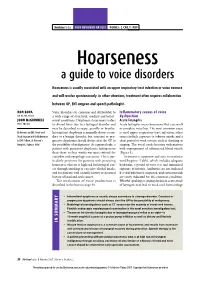
Hoarseness a Guide to Voice Disorders
MedicineToday PEER REVIEWED ARTICLE POINTS: 2 CPD/1 PDP Hoarseness a guide to voice disorders Hoarseness is usually associated with an upper respiratory tract infection or voice overuse and will resolve spontaneously. In other situations, treatment often requires collaboration between GP, ENT surgeon and speech pathologist. RON BOVA Voice disorders are common and attributable to Inflammatory causes of voice MB BS, MS, FRACS a wide range of structural, medical and behav- dysfunction JOHN McGUINNESS ioural conditions. Dysphonia (hoarseness) refers Acute laryngitis FRCS, FDS RCS to altered voice due to a laryngeal disorder and Acute laryngitis causes hoarseness that can result may be described as raspy, gravelly or breathy. in complete voice loss. The most common cause Dr Bova is an ENT, Head and Intermittent dysphonia is normally always secon - is viral upper respiratory tract infection; other Neck Surgeon and Dr McGuinness dary to a benign disorder, but constant or pro- causes include exposure to tobacco smoke and a is ENT Fellow, St Vincent’s gressive dysphonia should always alert the GP to short period of vocal overuse such as shouting or Hospital, Sydney, NSW. the possibility of malignancy. As a general rule, a singing. The vocal cords become oedematous patient with persistent dysphonia lasting more with engorgement of submucosal blood vessels than three to four weeks warrants referral for (Figure 3). complete otolaryngology assessment. This is par- Treatment is supportive and aims to maximise ticularly pertinent for patients with persisting vocal hygiene (Table), which includes adequate hoarseness who are at high risk for laryngeal can- hydration, a period of voice rest and minimised cer through smoking or excessive alcohol intake, exposure to irritants. -

Parent's Guide to a Sore Throat
Contact your GP (or call 111) Useful contacts: again Your GP surgery on:....................................... Although in most cases the sore throat (Please insert surgery number here) improves in few days, please contact the GP if any of the following occurs: GP Out of Hours: (After 6.30pm and before 8am). Ring 111 and you can speak to a 1. Your child persistently refuses oral fl uids doctor. If necessary, your child can be seen and has not passed urine for over 18 at one of their centres. Parent’s guide hours. Bristol City Walk-in Centre at Broadmead 2. The fever does not settle within four or to a sore throat Medical Centre located in Boots fi ve days. (Mon-Sat 8am-8pm, Sundays and Bank Holidays 11am-5pm) on: 0117 954 9828 3. Your child develops diffi culty in swallowing despite regular paracetamol South Bristol NHS Community Hospital or ibuprofen. Urgent Care Centre (Every day 8am-8pm) on: 0117 342 9692 4. Your child starts drooling because they Visit www.nhs.uk to fi nd your nearest cannot swallow their saliva. centre. Call 999 If your child is seriously ill, you may be asked to attend the Children’s Hospital If your child develops severe breathing emergency department. diffi culties For further copies of this leafl et, or if you would like it in other formats or languages, please contact 0117 900 2384. Produced in partnership with Bristol Clinical Commissioning Group, North Bristol NHS Trust and University Hospitals Bristol NHS Foundation Trust. End date: June 2016 Your child has been diagnosed with a sore What is the treatment of a sore throat which is very common in children. -

Allergic Bronchopulmonary Aspergillosis: a Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2
Review Allergy Asthma Immunol Res. 2016 July;8(4):282-297. http://dx.doi.org/10.4168/aair.2016.8.4.282 pISSN 2092-7355 • eISSN 2092-7363 Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India 2Department of Respiratory Medicine, Mata Chanan Devi Hospital, New Delhi, India This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. In susceptible individuals, inhalation of Aspergillus spores can affect the respiratory tract in many ways. These spores get trapped in the viscid spu- tum of asthmatic subjects which triggers a cascade of inflammatory reactions that can result in Aspergillus-induced asthma, allergic bronchopulmo- nary aspergillosis (ABPA), and allergic Aspergillus sinusitis (AAS). An immunologically mediated disease, ABPA, occurs predominantly in patients with asthma and cystic fibrosis (CF). A set of criteria, which is still evolving, is required for diagnosis. Imaging plays a compelling role in the diagno- sis and monitoring of the disease. Demonstration of central bronchiectasis with normal tapering bronchi is still considered pathognomonic in pa- tients without CF. Elevated serum IgE levels and Aspergillus-specific IgE and/or IgG are also vital for the diagnosis. Mucoid impaction occurring in the paranasal sinuses results in AAS, which also requires a set of diagnostic criteria. Demonstration of fungal elements in sinus material is the hall- mark of AAS. -

Interstitial Lung Disease
Interstitial Lung Disease Nitin Bhatt, MD Assistant Professor of Internal Medicine Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine Ohio State University Medical Center Interstitial Lung Disease Jim Allen, MD Professor of Internal Medicine Division of Pulmonary & Critical Care Medicine Ohio State University Medical Center 1 Case #1 Case #1 • 57 y.o. WM with a history of shortness of breath and cough that has been present for 1 year • Initially worse with walking, moderate exertion. No resting symptoms. • Now activity limiting • Associated with a dry, nonproductive cough • Negative cardiac evaluation • PMHx: HTN • Meds: HCTZ • SOCHx: 30 pack year smoking history, quit 10 years ago 2 Case #1 • PE: HR 78, BP 138/67, sats 96% on room air • Lungs with bibasilar dry crackles • Ext with clubbing • PFTs: • FVC 69% predicted • FEV1 72% • TLC 62% • DLCO 53% • 6 Minute walk: Walks 1100 feet with an initial sat of 96% dropping to 79% on room air Case #1 • CT scan • Subpleural fibrosis 3 Case #1 • CT scan • TtibTraction bronchi hitiectasis • • Honeycombing Case #1 • Lunggpy biopsy • Interstitial thickening • Temporal heterogeneity • Fibroblastic foci 4 Idiopathic Pulmonary Fibrosis • Most common ILD of unknown etiology • MilMainly aff fftects peopl e > >50 50 yo, mos t are over the age of 60 yo • Incidence is estimated at 7.4-10.7 cases per 100,000 per year • Prevalence of IPF is estimated at 13-20/100,000 • Most are current or former smokers • Potential risk factors for developing IPF include cigarette smoking, occupational/environmental -
Frequently Asked Questions About Sinusitis Table of Contents
FREQUENTLY ASKED QUESTIONS ABOUT SINUSITIS TABLE OF CONTENTS Chapter 1: Do I have acute sinusitis or chronic sinusitis? 3 Chapter 2: Do I need antibiotics for my acute sinusitis? 4 Chapter 3: What kind of chronic sinusitis do I have? 5 Chapter 4: Why do I have chronic sinusitis? 7 Chapter 5: What are my treatment options for chronic sinusitis? 9 Chapter 6: When should I consider surgery? 11 Chapter 7: Are my allergies causing my chronic sinusitis? 12 Chapter 8: Is there a connection between chronic sinusitis and asthma? 13 Chapter 9: What can I do to keep my chronic sinusitis under control? 14 Chapter 10: About Metropolitan ENT & Facial Plastic Surgery 15 DISCLAIMER: This information is for educational and informational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this e-book. While all attempts have been made to verify information provided in this publication, the Publisher assumes no responsibility for errors, omissions, or contrary interpretation of the subject matter herein. The content of this e-book was developed and published by eos Healthcare Partners, LLC. Accordingly the information and material in this book is copyright, 2015 © eos Healthcare Partners, LLC.Therefore no part of this book may in any form be reproduced, stored, broadcast, sold or transmitted without the prior permission of the publisher, eos Healthcare Partners, LLC. -

Defective Regulation of Immune Responses in Croup Due to Parainfluenza Virus
716 WELLIVER ET AL. Science 221: 1067-1070 20. Mawhinney TP, Feather MS, Martinez JR, Barbero GJ 1979 The chronically 17. Quissell DO 1980 Secretory response of dispersed rat submandibular cells: I. reserpinized rat as an animal model for cystic fibrosis: acute effect of Potassium release. Am J Physiol 238:C90-C98 isoproterenol and pilocarpine upon pulmonary lavage fluid. Pediatr Res 18. Lowry OH, Rosebrough NF, Farrar AL, Randall RJ 195 1 Protein measurement 13:760-763 with the Folin phenol reagent. J Biol Chem 193:265-268 21. Frizzell RA, Fields M, Schultz SG 1979 Sodium-coupled chloride transport by 19. Perlmutter J, Martinez JR 1978 The chornically reserpinized rat as a possible epithelial tissues. Am J Physiol 236:FI-F8 model for cystic fibrosis: VII. Alterations in the secretory response to secretin 22. Welsh M 1983 Inhibition of chloride secretion by furosemide in canine tracheal and to cholecystokinin from the pancreas in vivo. Pediatr Res 12: 188- 194 epithelium. J Memb Biol71:219-226 003 1-3998/85/1907-07 16$02.00/0 PEDIATRIC RESEARCH Vol. 19, No. 7, 1985 Copyright O 1985 International Pediatric Research Foundation, Inc. Printed in U.S.A. Defective Regulation of Immune Responses in Croup Due to Parainfluenza Virus ROBERT C. WELLIVER, MARTHA SUN, AND DEBORAH RINALDO Department ofPediatrics, State University of New York at Buffalo, and Division of Infectious Diseases, Children S Hospital, Buffalo, New York 14222 ABSTRACT. In order to determine if defects in regulation Croup is a common respiratory illness of childhood, yet fairly of immune responses play a role in the pathogenesis of little is known about its pathogenesis.