AIDSTAR-One | CASE STUDY SERIES October 2011 Risky Business Made Safer Corridors of Hope: an HIV Prevention Program in Zambian Border and Transit Towns1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Kafue-Lions Den (Beira Corridor)
Zambia Investment Forum (2011) Kuala Lumpur, Malaysia PUBLIC PRIVATE PARTNERSHIPS FRAMEWORK IN ZAMBIA: PRESENTED BY: Mr. Hibene Mwiinga, Deputy Director of National Policy and Programme Implementation MINISTER OF FINANCE AND NATIONAL PLANNING MOFNP OUTLINE: PPP Policy and Legal Framework What is PPP Agenda in Zambia Objectives of PPPs in Zambia Background of PPP in Zambia Pipeline of PPP Projects Key elements of a PPP project Unsolicited Bids Challenges Investment Opportunities in Communications and Transport Sectors MOFNP Policy and Legal Framework PPP Policy approved in 2007 PPP Act enacted in August 2009 MOFNP What is the PPP Agenda in Zambia? To enhance Economic Development in the Country through partnerships between Govt and Private sector; To support the National Vision of the Country which is to make “Zambia to a Prosperous and Middle-Income Country by 2030”; PPPs present a Paradigm shift in way of doing business in Zambia; MOFNP Rationale of taking the PPP route in Zambia Facilitation of Government Service Delivery Public Debt Reduction Promotion of Public Sector Savings Project Cost Savings Value for Money Efficiency in Public Sector Delivery Attraction of Private Sector in Public Goods & Services Investment MOFNP Background of PPPs in Zambia • PPPs are a „recent‟ phenomena in Zambia • Old and classic examples – Zambia Railways Line (Cape-Cairo dream by Cecil Rhodes) – TAZAMA • More recent examples – Railway Systems of Zambia (RSZ) Concession – Urban Markets (BOT) – Maintenance of the Government Complex (Maintenance -

Zambia National Programme Policy Brief
UN-REDD ZAMBIA NATIONAL PROGRAMME POLICY BRIEF DRIVERS OF DEFORESTATION AND POTENTIAL FOR REDD+ INTERVENTIONS IN ZAMBIA Jacob Mwitwa, Royd Vinya, Exhildah Kasumu, Stephen Syampungani, Concilia Monde, and Robby Kasubika Background Deforestation and poor forest stewardship reduce carbon stocks and the capacity for carbon storage in Zambian forests. Forest loss is caused by a mix of factors that are not well understood, and their combined effects act to either directly drive forest cover loss or interact with other or influences. In order to understand the drivers and their interactions a study was commissioned to provide a preliminary understanding of drivers of deforestation and the potential for forest types (Fanshawe 1971; White 1983); to differ REDD+ in Zambia; to assess the extent of current substantially in the key drivers of deforestation consumption of forest products, forest production (ZFAP 1998); and have diverse cultural and socio- and development trends as well as potential future economic settings. Sample selection of districts shifts in these patterns that may affect deforestation was based on review of statistics from isolated case levels; to draw conclusions on which actions/trends studies and on analysis of land cover maps and would likely have the worst consequences in terms satellite images. of causing additional deforestation and how these could be reduced in future; and finally to outline the potential for REDD+ in these circumstances. Vegetation Types Of Zambia An interdisciplinary data gathering approach was Zambia has three major vegetation formations. The adopted which integrated literature search, policy closed forests are limited in extent, covering only level consultancy, community level consultations, about 6% of the Country. -

The Contribution of Dry Forests to Rural Poverty Reduction and to the National Economy: Zambia
The Contribution of Dry Forests to Rural Poverty Reduction and to the National Economy: Zambia Technical Report Samuel Mulenga Bwalya Department of Economics, University of Zambia, Box 32379, Lusaka Tel# 260 1 290475, [email protected] The Contribution of Dry Forests to Rural Poverty Reduction and to the National Economy: Zambia Draft summary We have shown that forests and woodland resources contribute, on average, 21% to total production and income of rural households. Aggregating forest production and income to a national levels based on sample information is challenging task and by no means likely to be very precise and accurate. But scaling up sample estimates to the national level facilitates inter-sectoral comparisons and would sharpen our insights about the importance of forests and woodland resources in rural development and poverty reduction. Sample estimates and national statistics on the number of rural households is used to scale up and estimate the contribution of forest and woodland resources to the national rural household sector. We multiply the proportion of households harvesting a particular forest product by the total number of rural households in Zambia. This gives us an estimate of the number of rural household across the country that harvest forest a given forest product both for consumption within the household and for sell to obtain cash income. This estimate is then multiplied by the average value of each forest product harvested to obtain the total contribution of the forests sector to rural household economy. Because we ignore value addition along the supply chain and other forms of income and services households derive from forests, this estimate should be seen to represent the minimum contribution of forest resources to rural household sector. -

Profiles of Active Civil Society Organisations in North-Western, Copperbelt and Southern Provinces of Zambia
Profiles of Active Civil Society Organisations in North-Western, Copperbelt and Southern Provinces of Zambia On behalf of Implemented by Published by: Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH Registered offices Bonn and Eschborn, Germany Address Civil Society Participation Programme (CSPP) Mpile Office Park, 3rd floor 74 Independence Avenue Lusaka, Zambia P +260 211 250 894 E [email protected] I www.giz.de/en Programme: Civil society participation in governance reform and poverty reduction Author: Isaac Ngoma, GFA Consulting Group GmbH Editor: Markus Zwenke, GFA Consulting Group GmbH, Eulenkrugstraße 82, 22359 Hamburg, Germany Design/layout: GFA Consulting Group GmbH and IE Zhdanovich Photo credits/sources: GFA Consulting Group GmbH On behalf of German Federal Ministry for Economic Cooperation and Development (BMZ) As of June, 2021 TABLE OF CONTENT ACTIVE CIVIL SOCIETY ORGANISATIONS IN NORTH-WESTERN PROVINCE � � � � � �7 Dream Achievers Academy �������������������������������������������������������������������������������������������������������������������������� 8 Anti-voter Apathy Project ���������������������������������������������������������������������������������������������������������������������������� 9 Mentra Youth Zambia . 10 The Africa Youth Initiative Network �������������������������������������������������������������������������������������������������������� 11 Radio Kabangabanga ���������������������������������������������������������������������������������������������������������������������������������� -

Zambia Anglican Council
ZAMBIA ANGLICAN COUNCIL FIRST QUARTER NETSFORLIFE® PROGRAMME REPORT, 2014 In the picture is a group of MCAs getting ready for distribution of LLITNs in Kitwe District ZAMBIA ANGLICAN COUNCIL 6 BISHOPS RD KABULONGA PO BOX 320100 LUSAKA, ZAMBIA E-mail:[email protected] LIST OF ABBREVIATION/ACRONYMS DDCC : DISTRICT DEVELOPMENT COORDINATING COMMITTEE DHO : DISTRICT HEALTH OFFICE DMTF : DISTRICT MALARIA TASK FORCE IEC : INFORMATION EDUCATION AND COMMUNICATION ITN : INSECTICIDE TREATED NET LLITNS : LONG LASTING INSECTICIDE TREATED NETS MCAs : MALARIA CONTROL AGENTS N/A : NOT APLLICABLE NDP : NATIONAL PROGRAMMES DIRECTOR NMCC : NATIONAL MALARIA CONTROL CENTRE SADC : SOUTHERN AFRICA DEVELOPMENT COMMUNITY 1.0 INTRODUCTION Malaria is still endemic in all NetsforLife Project sites in Zambia, and has continued to be a major public health concern. However, ZAC has continued to make significant progress to contribute to the reduction of the malaria morbidity and mortality in line with the Government vision of a “malaria free nation” by 2015 and ZAC has been part of this progress with support from Episcopal Relief & Development. At community level, ZAC has continued to work with Malaria control agents and also with other stakeholders in the fight against malaria. Community engagement has contributed to this success over the years. In the recent past, there have been some new strategies to combat malaria in Zambia and ZAC has adopted these strategies that are aimed at pre elimination of malaria in selected districts namely Kazungula, Sesheke, Shangombo, Livingstone, Kalabo, Senanaga and Sikongo. These strategies include the “Testing, Treating and Tracking” of each malaria case. This is complemented by active surveillance of malaria cases by use of active and passive registers that have been introduced. -

USAID/Zambia Partners in Development Book
PARTNERS IN DEVELOPMENT July 2018 Partners in Zambia’s Development Handbook July 2018 United States Agency for International Development Embassy of the United States of America Subdivision 694 / Stand 100 Ibex Hill Road P.O. Box 320373 Lusaka, Zambia 10101 Cover Photo: As part of a private -sector and youth-engagement outreach partnership, media entrepreneur and UNAIDS Ambassador Lulu Haangala Wood (l), musician and entrepreneur Pompi (c), and Film and TV producer Yoweli Chungu (r) lend their voices to help draw attention to USAID development programs. (Photo Credit: Chando Mapoma / USAID Zambia) Our Mission On behalf of the American People, we promote and demonstrate democratic values abroad, and advance a free, peaceful, and prosperous world. In support of America's foreign policy, the U.S. Agency for International Development leads the U.S. Government's international development and disaster assistance through partnerships and investments that save lives, reduce poverty, strengthen democratic governance, and help people emerge from humanitarian crises and progress beyond assistance. Our Interagency Initiatives USAID/Zambia Partners In Development 1 The United States Agency for International Development (USAID) is the lead U.S. Government agency that works to end extreme global poverty and enable resilient, democratic societies to realize their potential. Currently active in over 100 countries worldwide, USAID was born out of a spirit of progress and innovation, reflecting American values and character, motivated by a fundamental belief in helping others. USAID provides development and humanitarian assistance in Africa, Asia and the Near East, Latin America and the Caribbean, and Europe. Headquartered in Washington, D.C., USAID retains field missions around the world. -

Can Design Thinking Be Used to Improve Healthcare in Lusaka Province, Zambia?
INTERNATIONAL DESIGN CONFERENCE - DESIGN 2014 Dubrovnik - Croatia, May 19 - 22, 2014. CAN DESIGN THINKING BE USED TO IMPROVE HEALTHCARE IN LUSAKA PROVINCE, ZAMBIA? C. A. Watkins, G. H. Loudon, S. Gill and J. E. Hall Keywords: ethnography, design thinking, Zambia, healthcare 1. Background ‘Africa experiences 24% of the global burden of disease, while having only 2% of the global physician supply and spending that is less than 1% of global expenditures.’ [Scheffler et al. 2008]. Every day the equivalent of two jumbo jets full of women die in Childbirth; 99% of these deaths occur in the developing world [WHO 2012]. For every death, 20 more women are left with debilitating conditions, such as obstetric fistula or other injuries to the vaginal tract [Jensen et al. 2008]. In the last 50 years, US$2.3 trillion has been spent on foreign aid [Easterly 2006]; US$1 trillion in Africa [Moyo 2009]. Despite this input, both Easterly and Moyo argue there has been little benefit. Easterly highlights that this enormous donation has not reduced childhood deaths from malaria by half, nor enabled poor families access to malaria nets at $4 each. Hodges [2007] reported that although equipment capable of saving lives is available in developing countries, more than 50% is not in service. Studies have asked why this should be so high [Gratrad et al. 2007], [Dyer et al. 2009], [Malkin et al. 2011] the majority focussing on medical equipment donation. They suggest that it is not feasible to directly donate equipment from high to low-income settings without understanding how the receiving environment differs from that which it is designed for. -
2.4 Zambia Railway Assessment
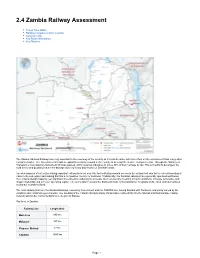
2.4 Zambia Railway Assessment Travel Time Matrix Railway Companies and Consortia Capacity Table Key Route Information Key Stations The Zambia National Railways are very important to the economy of the country as it is a bulk carrier with less effect on the environment than many other transport modes. The Government intends to expand its railway network in the country to develop the surface transport sector. Through the Ministry of Transport, a new statutory instrument (SI) was passed, which requires industries to move 30% of their carriage by rail. This is in a bid to decongest the road sector and possibly reduce the damage done by heavy duty trucks on Zambian roads. The development of rail routes linking important exit points is not only vital for facilitating smooth access to the outside but also for the overall boosting of trade in the sub-region and making Zambia a competitive country for business. Traditionally, the Zambian railways have generally operated well below their original design capacity, yet significant investment is underway to increase their volumes by investing in track conditions, increase locomotive and wagon availability and increase operating capital. The rail network remains the dominant mode of transportation for goods on the local and international routes but is under-utilized. The main railway lines are the Zambia Railways, owned by Government and the TAZARA line, linking Zambia with Tanzania, and jointly owned by the Zambian and Tanzanian governments. The opening of the Chipata-Mchinji railway link provides connectivity into the Malawi and Mozambique railway network and further connects Zambia to the port of Nacala. -

Occurrence of Cholera in Lukanga Fishing Camp, Kapiri-Mposhi District, Zambia
OUTBREAK REPORT Occurrence of cholera in Lukanga fishing camp, Kapiri-mposhi district, Zambia R Murebwa-Chirambo1, R Mwanza2, C Mwinuna3, ML Mazaba1, I Mweene-Ndumba1, J Mufunda1 1. World Health Organization, Country office, Lusaka, Zambia 2. Ministry of Health, Provincial Health Office, Kabwe, Zambia 3. Ministry of Health, District Health Office, Kapiri Mposhi, Zambia Correspondence: Rufaro Murembwa-Chirambo ([email protected]) Citation style for this article: Murebwa-Chirambo R, Mwanza R, Mwinuna C, Mazaba ML, Mweene-Ndumba I, Mufunda J. Occurrence of cholera in Lukanga fishing camp, Kapiri-mposhi district, Zambia. Health Press Zambia Bull. 2017;1(1) [Inclusive page numbers] Most of the cholera outbreaks in Zambia have been There is need to employ interventions in the area of recorded from fishing camps and peri-urban areas of water and sanitation on the Lukanga swamps in order the Copperbelt, Luapula and Lusaka provinces. to address the annual cholera outbreaks. Cholera cases have been recorded every year in the Lukanga fishing camps in the last five years. This article Introduction documents a cholera outbreak reported at the Lukanga The first outbreak of cholera in Zambia was fishing camp in Kapiri Mposhi district in September, 2016. All cases that met the cholera case definition as reported in 1977/1978, then cases appeared prescribed in the Integrated Diseases Surveillance and again in 1982/1983. The first major outbreak Response guidelines were admitted and treated using occurred in 1990 and lasted until 1993. Since WHO standard protocols. A total of 27 patients all adult except 1, 26 of whom were male were seen at the cholera then, cholera cases were registered every treatment center. -

Zambia Health Sector Public Expenditure Tracking and Quantitative Service Delivery Survey
Public Disclosure Authorized Zambia Health Sector Public Expenditure Tracking and Quantitative Service Delivery Survey Public Disclosure Authorized Collins Chansa Thulani Matsebula Moritz Piatti Dale Mudenda Chitalu Miriam Chama-Chiliba Bona Chitah Oliver Kaonga Chris Mphuka Public Disclosure Authorized April 2019 Public Disclosure Authorized © 2019 International Bank for Reconstruction and Development / The World Bank 1818 H Street NW, Washington, DC 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some rights reserved 1 2 3 4 19 18 17 16 This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immunities of The World Bank, all of which are specifically reserved. Rights and Permissions This work is available under the Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) http://creativecommons.org/licenses/by/3.0/igo. Under the Creative Commons Attribution license, you are free to copy, distribute, transmit, and adapt this work, including for commercial purposes, under the following conditions: Attribution—Please cite the work as follows: World Bank. -

Information About Gender-Based Violence for People with Disabilities. Places to Get Help in Zambia
Information about Gender-Based Violence for People with Disabilities Places to get help in Zambia In Zambia there is a law called the Anti-Gender Based Violence Act. It says you can get help if someone does very bad things to you. There are places called one stop centers that give you help with your health and the law all in one place. Police stations have special police men and women to help you. They work in the Victim Support Unit at your local police station. Free helplines you can call at any time in the day or night Name What it does Number CHAMP Hot-line They can give you Hotline: 999 information and support about your health. Lifeline They help adults. Hotline: 933 They can help you if someone is hurting you or doing bad things to you. They help children CHILD-LINE who need any kind of help. Hotline: 116 They can help you quickly if you need it. 1 Groups that help with the law Name What they do Address, Number Legal Aid Board They can give you 1st Floor, New Kent Zambia free information and support Building. with the law. Haile Selassie Ave, P.O Box 32761 Lusaka Zambia Telephone: +260 211 256 453; +260 211 256 454 National Legal Aid They give information Musonda Ngosa Road Clinic for Women and support to women 110A/150 Villa and children. Elizabetha, Lusaka Telephone: +260 211 220 595 Legal Resources They can help you Woodgate House Foundation with paying for things Cairo Road, Lusaka like going to court. -

ZAMSTAR TB Prevalence Survey Monde Muyoyeta ZAMBART Project Primary Objective
ZAMSTAR TB Prevalence Survey Monde Muyoyeta ZAMBART Project Primary Objective Measure the effect of the ZAMSTAR interventions on TB prevalence by comparing the prevalence of TB across study arms Secondary Objectives Determine the prevalence of culture positive tuberculosis in the study sites Measure the prevalence of risk factors for TB (HIV, diabetes, smoking, indoor air pollution, alcohol & SES) Determine the prevalence of people with current TB (self-reported) Determine health care seeking behavior of people with respiratory symptoms ZAMSTAR: The Zambia/South Africa TB and AIDS Reduction Study-Overview A study designed to find out whether combinations of community based interventions aimed at increasing case finding of TB and implementing packages of combined TB/HIV care can reduce TB Interventions were implemented for 3 years from 2006-2009 Prevalence of TB across study arms is one of the end points Study Setting ZAMSTAR ZAMSTAR Sites in Zambia Sites Luapula Mansa District-Senama, Central Copperbelt Ndola District-Chifubu and Chipulukusu Kitwe District-Chimwemwe, Ndeke Central Province Kabwe District-Makululu, Ngungu/Bwacha Lusaka Province Lusaka District-Chawama, Kanyama, Chipata, George Southern Province Choma District-Pemba and Shempande Livingstone District- Maramba and Dambwa Prevalence Survey -Sample Size & Enumeration 24 sites, 16 in Zambia and 8 in Western Cape- SA Sample size – 80 000 Zambia – 40 000 Western cape Enumeration – SEA are randomly visited – Every HH in the SEA is visited and enumerated MAPS with SEAS numbered