Anterior Knee Pain Information and Advice
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Knee Pain Prevention
DOCTORS CARE OSTEOARTHRITIS PROGRAM FOR Knee Pain Prevention Our program offers a non-surgical option that is safe and effective What Is Osteoarthritis of the Knee? In most cases osteoarthritis is caused by a slow degenerative process whereby, as we age and become less active, we tend to get tighter joints and weaker muscles. This in turn causes our joints to become dysfunctional and then become inflamed. The inflammation causes decreased blood flow to the joint tissues and thus decreased production of joint fluid. This, in turn, causes wear and tear on the joint which causes more inflammation and even less nutrients to the joint tissues. As a result, range of motion and strength are further decreased causing greater dysfunction Aand Healthy greater Joint inflammation. Left untreated, this will lead to a Medialdownward collateral ligamentspiral of degeneration. Joint capsule Muscles Tendons A Healthy Joint Medial collateral ligament Joint capsule Muscles TendonsBone Cartilage Synovial uid In a healthy joint, the ends of bones are encased in smooth cartilage. Together, they are protected by a joint capsule lined with a Bonesynovial membrane thatCartilage produces synovial uid. e capsule and uid protect the cartilage, muscles, and connective tissues.Synovial uid InA aJoint healthy With joint, theSevere ends of Osteoarthritis bones are encased in smooth cartilage. Together, they are protected by a joint capsule lined with a synovial membrane that produces synovialMedial uid. collateral e capsule ligament and uid protect the cartilage, muscles, and connectiveBone spurs tissues. Muscles A Joint With Severe Osteoarthritis Tendons Medial collateral ligament Bone spurs Muscles TendonsBone Worn-away Cartilage cartilage Synovial uid fragments in uid With osteoarthritis, the cartilage becomes worn away. -

Knee Osteoarthritis
BRIGHAM AND WOMEN’S HOSPITAL Department of Rehabilitation Services Standard of Care: _Osteoarthritis of the Knee Case Type / Diagnosis: Knee Osteoarthritis. ICD-9: 715.16, 719.46 Osteoarthritis/Osteoarthrosis (OA) is the most common joint disease causing disability, affecting more than 7 million people in the United States 1. OA is a disease process of axial and peripheral joints. It is characterized by progressive deterioration and loss of articular cartilage and by reactive bone changes at the margins of the joints and in the subchondral bone. Clinical manifestations are characterized by slowly developing joint pain, stiffness, and joint enlargement with limitations of motion. Knee osteoarthritis (OA) results from mechanical and idiopathic factors that alter the balance between degradation and synthesis of articular cartilage and subchondral bone. The etiology of knee OA is not entirely clear, yet its incidence increases with age and in women. 1 The etiology may have genetic factors affecting collagen, or traumatic factors, such as fracture or previous meniscal damage. Obesity is a risk factor for the development and progression of OA. Early degenerative changes predict progression of the disease. Underlying biomechanical factors, such as varum or valgum of the tibial femoral joint may predispose people to OA. However Hunter et al 2reported knee alignment did not predict OA, but rather was a marker of the disease severity. Loss of quadriceps muscle strength is associated with knee pain and disability in OA. Clinical criteria for the diagnosis of OA of the knee has been established by Altman3 Subjects with examination finding consistent with any of the three categories were considered to have Knee OA. -

Compression Garments for Leg Lymphoedema
Compression garments for leg lymphoedema You have been fitted with a compression garment to help reduce the lymphoedema in your leg. Compression stockings work by limiting the amount of fluid building up in your leg. They provide firm support, enabling the muscles to pump fluid away more effectively. They provide most pressure at the foot and less at the top of the leg so fluid is pushed out of the limb where it will drain away more easily. How do I wear it? • Wear your garment every day to control the swelling in your leg. • Put your garment on as soon as possible after getting up in the morning. This is because as soon as you stand up and start to move around extra fluid goes into your leg and it begins to swell. • Take the garment off before bedtime unless otherwise instructed by your therapist. We appreciate that in hot weather garments can be uncomfortable, but unfortunately this is when it is important to wear it as the heat can increase the swelling. If you would like to leave off your garment for a special occasion please ask the clinic for advice. What should I look out for? Your garment should feel firm but not uncomfortable: • If you notice the garment is rubbing or cutting in, adjust the garment or remove it and reapply it. • If your garment feels tight during the day, try and think about what may have caused this. If you have been busy, sit down and elevate your leg and rest for at least 30 minutes. -

Sports Ankle Injuries Assessment and Management
FOCUS Sports injuries Sports ankle injuries Drew Slimmon Peter Brukner Assessment and management Background Case study Lucia is a female, 16 years of age, who plays netball with the Sports ankle injuries present commonly in the general state under 17s netball team. She presents with an ankle injury practice setting. The majority of these injuries are inversion sustained at training the previous night. She is on crutches and plantar flexion injuries that result in damage to the and is nonweight bearing. Examination raises the possibility of lateral ligament complex. a fracture, but X-ray is negative. You diagnose a severe lateral Objective ligament sprain and manage Lucia with ice, a compression The aim of this article is to review the assessment and bandage and a backslab initially. She then progresses through management of sports ankle injuries in the general practice a 6 week rehabilitation program and you recommend she wear setting. an ankle brace for at least 6 months. Discussion Assessment of an ankle injury begins with a detailed history to determine the severity, mechanism and velocity of the injury, what happened immediately after and whether there is a past history of inadequately rehabilitated ankle injury. Examination involves assessment of weight bearing, inspection, palpation, movement, and application of special examination tests. Plain X-rays may be helpful to exclude a fracture. If the diagnosis is uncertain, consider second The majority of ankle injuries are inversion and plantar line investigations including bone scan, computerised flexion injuries that result in damage to the lateral tomography or magnetic resonance imaging, and referral to a ligament complex (Figure 1). -

Patellar Tendinopathy: Some Aspects of Basic Science and Clinical Management
346 Br J Sports Med 1998;32:346–355 Br J Sports Med: first published as 10.1136/bjsm.32.4.346 on 1 December 1998. Downloaded from OCCASIONAL PIECE Patellar tendinopathy: some aspects of basic science and clinical management School of Human Kinetics, University of K M Khan, N MaVulli, B D Coleman, J L Cook, J E Taunton British Columbia, Vancouver, Canada K M Khan J E Taunton Tendon injuries account for a substantial tendinopathy, and the remainder to tendon or Victorian Institute of proportion of overuse injuries in sports.1–6 tendon structure in general. Sport Tendon Study Despite the morbidity associated with patellar Group, Melbourne, tendinopathy in athletes, management is far Victoria, Australia 7 Anatomy K M Khan from scientifically based. After highlighting The patellar tendon, the extension of the com- J L Cook some aspects of clinically relevant basic sci- mon tendon of insertion of the quadriceps ence, we aim to (a) review studies of patellar femoris muscle, extends from the inferior pole Department of tendon pathology that explain why the condi- of the patella to the tibial tuberosity. It is about Orthopaedic Surgery, tion can become chronic, (b) summarise the University of Aberdeen 3 cm wide in the coronal plane and 4 to 5 mm Medical School, clinical features and describe recent advances deep in the sagittal plane. Macroscopically it Aberdeen, Scotland, in the investigation of this condition, and (c) appears glistening, stringy, and white. United Kingdom outline conservative and surgical treatment NMaVulli options. BLOOD SUPPLY Department of The blood supply has been postulated to con- 89 Medicine, University tribute to patellar tendinopathy. -

Posterior Cruciate Ligament (PCL): Reconstruction and Rehabilitation
Patient information – PCL reconstruction Posterior cruciate ligament (PCL): reconstruction and rehabilitation Introduction Posterior cruciate ligament reconstruction is an operation to replace your torn posterior cruciate ligament (PCL) and restore stability to your knee joint. This leaflet outlines what happens during and after surgery, outlines the risks and benefits, and gives advice and exercises to help you recover if you decide to go ahead with the operation. Posterior (back) view Anterior (front) view The PCL is the largest ligament in the knee and stops the shin bone from moving too far backwards, relative to your thigh bone. It is commonly injured by a significant blow to the front of the knee/upper shin. Most athletic PCL injuries occur during a fall onto the flexed (bent) knee. Hyperextension (‘over straightening’) and hyperflexion (‘bending too far’) of the knee can also cause a PCL injury and the PCL is often involved when there is injury to multiple ligaments in a knee dislocation. Not everyone who has a PCL injury will require surgery as most isolated tears (no other ligaments involved) can heal just with the early application of an appropriate splint/brace. If the ligament does not heal or there are other ligaments involved, some people can notice a ‘looseness’ and an occasional feeling of giving way. This requires a reconstruction (replacement) operation. Posterior cruciate ligament (PCL) reconstruction, August 2020 1 Posterior cruciate ligament (PCL) reconstruction Reasons for not operating To undertake this major reconstruction, you must have appropriate symptoms of instability. This is not an operation for pain. An operation is not recommended if there is any active infection in or around the knee or when there is a lot of other disease, such as arthritis, within the joint. -
Intramedullary Nailing for Femur Fracture Management a Guide for Parents
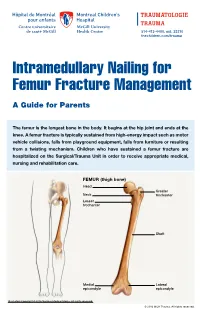
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at the knee. A femur fracture is typically sustained from high-energy impact such as motor vehicle collisions, falls from playground equipment, falls from furniture or resulting from a twisting mechanism. Children who have sustained a femur fracture are hospitalized on the Surgical/Trauma Unit in order to receive appropriate medical, nursing and rehabilitation care. FEMUR (thigh bone) Head Greater Neck trochanter Lesser trochanter Shaft Medial Lateral epicondyle epicondyle Illustration Copyright © 2016 Nucleus Medical Media, All rights reserved. © 2016 MCH Trauma. All rights reserved. FEMUR FRACTURE MANAGEMENT The pediatric Orthopedic Surgeon will assess your child in order to determine the optimal treatment method. Treatment goals include: achieving proper bone realignment, rapid healing, and the return to normal daily activities. The treatment method chosen is primarily based on the child’s age but also taken into consideration are: fracture type, location and other injuries sustained if applicable. Prior to the surgery, your child may be placed in skin traction. This will ensure the bone is in an optimal healing position until it is surgically repaired. Occasionally, traction may be used for a longer period of time. The surgeon will determine if this management is needed based on the specific fracture type and/or location. ELASTIC/FLEXIBLE INTRAMEDULLARY NAILING This surgery is performed by the Orthopedic Surgeon in the Operating Room under general anesthesia. The surgeon will usually make two small incisions near the knee joint in order to insert two flexible titanium rods (intramedullary nails) Flexible through the femur. -

ANTERIOR KNEE PAIN Home Exercises
ANTERIOR KNEE PAIN Home Exercises Anterior knee pain is pain that occurs at the front and center of the knee. It can be caused by many different problems, including: • Weak or overused muscles • Chondromalacia of the patella (softening and breakdown of the cartilage on the underside of the kneecap) • Inflammations and tendon injury (bursitis, tendonitis) • Loose ligaments with instability of the kneecap • Articular cartilage damage (chondromalacia patella) • Swelling due to fluid buildup in the knee joint • An overload of the extensor mechanism of the knee with or without malalignment of the patella You may feel pain after exercising or when you sit too long. The pain may be a nagging ache or an occasional sharp twinge. Because the pain is around the front of your knee, treatment has traditionally focused on the knee itself and may include taping or bracing the kneecap, or patel- la, and/ or strengthening the thigh muscle—the quadriceps—that helps control your kneecap to improve the contact area between the kneecap and the thigh bone, or femur, beneath it. Howev- er, recent evidence suggests that strengthening your hip and core muscles can also help. The control of your knee from side to side comes from the glutes and core control; that is why those areas are so important in management of anterior knee pain. The exercises below will work on a combination of flexibility and strength of your knee, hip, and core. Although some soreness with exercise is expected, we do not want any sharp pain–pain that gets worse with each rep of an exercise or any increased soreness for more than 24 hours. -

ACR Appropriateness Criteria® Chronic Knee Pain
Revised 2018 American College of Radiology ACR Appropriateness Criteria® Chronic Knee Pain Variant 1: Adult or child greater than or equal to 5 years of age. Chronic knee pain. Initial imaging. Procedure Appropriateness Category Relative Radiation Level Radiography knee Usually Appropriate ☢ Image-guided aspiration knee Usually Not Appropriate Varies CT arthrography knee Usually Not Appropriate ☢ CT knee with IV contrast Usually Not Appropriate ☢ CT knee without and with IV contrast Usually Not Appropriate ☢ CT knee without IV contrast Usually Not Appropriate ☢ MR arthrography knee Usually Not Appropriate O MRI knee without and with IV contrast Usually Not Appropriate O MRI knee without IV contrast Usually Not Appropriate O Bone scan knee Usually Not Appropriate ☢☢☢ US knee Usually Not Appropriate O Radiography hip ipsilateral Usually Not Appropriate ☢☢☢ Variant 2: Adult or child greater than or equal to 5 years of age. Chronic knee pain. Initial knee radiograph negative or demonstrates joint effusion. Next imaging procedure. Procedure Appropriateness Category Relative Radiation Level MRI knee without IV contrast Usually Appropriate O Image-guided aspiration knee May Be Appropriate Varies CT arthrography knee May Be Appropriate ☢ CT knee without IV contrast May Be Appropriate ☢ US knee May Be Appropriate (Disagreement) O Radiography hip ipsilateral May Be Appropriate ☢☢☢ Radiography lumbar spine May Be Appropriate ☢☢☢ MR arthrography knee May Be Appropriate O MRI knee without and with IV contrast Usually Not Appropriate O CT knee with IV contrast Usually Not Appropriate ☢ CT knee without and with IV contrast Usually Not Appropriate ☢ Bone scan knee Usually Not Appropriate ☢☢☢ ACR Appropriateness Criteria® 1 Chronic Knee Pain Variant 3: Adult or child greater than or equal to 5 years of age. -
How to Self-Bandage Your Leg(S) and Feet to Reduce Lymphedema (Swelling)
Form: D-8519 How to Self-Bandage Your Leg(s) and Feet to Reduce Lymphedema (Swelling) For patients with lower body lymphedema who have had treatment for cancer, including: • Removal of lymph nodes in the pelvis • Removal of lymph nodes in the groin, or • Radiation to the pelvis Read this resource to learn: • Who needs self-bandaging • Why self-bandaging is important • How to do self-bandaging Disclaimer: This pamphlet is for patients with lymphedema. It is a guide to help patients manage leg swelling with bandages. It is only to be used after the patient has been taught bandaging by a clinician at the Cancer Rehabilitation and Survivorship (CRS) Clinic at Princess Margaret Cancer Centre. Do not self-bandage if you have an infection in your abdomen, leg(s) or feet. Signs of an infection may include: • Swelling in these areas and redness of the skin (this redness can quickly spread) • Pain in your leg(s) or feet • Tenderness and/or warmth in your leg(s) or feet • Fever, chills or feeling unwell If you have an infection or think you have an infection, go to: • Your Family Doctor • Walk-in Clinic • Urgent Care Clinic If no Walk-in clinic is open, go to the closest hospital Emergency Department. 2 What is the lymphatic system? Your lymphatic system removes extra fluid and waste from your body. It plays an important role in how your immune system works. Your lymphatic system is made up of lymph nodes that are linked by lymph vessels. Your lymph nodes are bean-shaped organs that are found all over your body. -

Back of Leg I
Back of Leg I Dr. Garima Sehgal Associate Professor “Only those who risk going too far, can possibly find King George’s Medical University out how far one can go.” UP, Lucknow — T.S. Elliot DISCLAIMER Presentation has been made only for educational purpose Images and data used in the presentation have been taken from various textbooks and other online resources Author of the presentation claims no ownership for this material Learning Objectives By the end of this teaching session on Back of leg – I all the MBBS 1st year students must be able to: • Enumerate the contents of superficial fascia of back of leg • Write a short note on small saphenous vein • Describe cutaneous innervation in the back of leg • Write a short note on sural nerve • Enumerate the boundaries of posterior compartment of leg • Enumerate the fascial compartments in back of leg & their contents • Write a short note on flexor retinaculum of leg- its attachments & structures passing underneath • Describe the origin, insertion nerve supply and actions of superficial muscles of the posterior compartment of leg Introduction- Back of Leg / Calf • Powerful superficial antigravity muscles • (gastrocnemius, soleus) • Muscles are large in size • Inserted into the heel • Raise the heel during walking Superficial fascia of Back of leg • Contains superficial veins- • small saphenous vein with its tributaries • part of course of great saphenous vein • Cutaneous nerves in the back of leg- 1. Saphenous nerve 2. Posterior division of medial cutaneous nerve of thigh 3. Posterior cutaneous -
Getting a Leg up on Land
GETTING A LEG UP in the almost four billion years since life on earth oozed into existence, evolution has generated some marvelous metamorphoses. One of the most spectacular is surely that which produced terrestrial creatures ON bearing limbs, fingers and toes from water-bound fish with fins. Today this group, the tetrapods, encompasses everything from birds and their dinosaur ancestors to lizards, snakes, turtles, frogs and mammals, in- cluding us. Some of these animals have modified or lost their limbs, but their common ancestor had them—two in front and two in back, where LAND fins once flicked instead. Recent fossil discoveries cast The replacement of fins with limbs was a crucial step in this transfor- mation, but it was by no means the only one. As tetrapods ventured onto light on the evolution of shore, they encountered challenges that no vertebrate had ever faced be- four-limbed animals from fish fore—it was not just a matter of developing legs and walking away. Land is a radically different medium from water, and to conquer it, tetrapods BY JENNIFER A. CLACK had to evolve novel ways to breathe, hear, and contend with gravity—the list goes on. Once this extreme makeover reached completion, however, the land was theirs to exploit. Until about 15 years ago, paleontologists understood very little about the sequence of events that made up the transition from fish to tetrapod. We knew that tetrapods had evolved from fish with fleshy fins akin to today’s lungfish and coelacanth, a relation first proposed by American paleontologist Edward D.