Ebola Virus Disease (EVD) Outbreak
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
GUINEE - PREFECTURE DE NZEREKORE Carte De La Population Et Des Structures Sanitaires 10 Mars 2021
GUINEE - PREFECTURE DE NZEREKORE Carte de la population et des structures sanitaires 10 mars 2021 BEYLA KOUANKAN BOOLA Boola Kognea Maghana Lomou Ouinzou Kogbata FOUMBADOU SEREDOU Boma Nord Gbana KOROPARA Lomou Gounangalaye Saouro Kpamou Koni Koropara Lokooua Alaminata Foozou Nyema Nord Kabieta Bassa´ta Koroh Keleta Ouleouon WOMEY Pampara Suobaya Bowe Nord NZEBELA Keorah Womey kerezaghaye Zenemouta Beneouli Selo MACENTA Loula Yomata Koule Komata KOULE Pale Yalakpala Tokpata Goueke Voumou LAINE Tamoe Niaragbaleye Kpoulo Pouro Kolata Maoun Wouyene PALE Zogbeanta GOUECKE Dapore Soulouta SOULOUTA Konipara Gouh Nona Banzou Tamoe Kola Kpagalaye Nyenh Koronta Youa Gbouo Kelemanda Zogotta Mahouor Koloda KOBELA KOYAMAH Kpaya Souhoule Kelouenta Poe KOKOTA Filikoele Koola Yleouena Batoata Gbadiou Niambara LOLA SAMOE Niema Komou Niarakpale Gbamba Banota Kpaya YALENZOU Boma Samoe Moata Kounala LOLA CTRE Koule Sud Boma Sud Horoya BOWE NZEREKORE CTRE Dorota Nyalakpale Bangoueta Gonia Nyen Commercial Toulemou Nzerekore Konia Kotozou Wessoua Aviation Mohomuo YOMOU Gbottoye Yalenzou Secteur zaapa Zao Yalenzou Kerema Gbenemou Lomou Centre centre Toulemou POPULATION PAR SOUS-PREFECTURE NZOO Gbenedapah SOUS-PREFECTURE POPULATION 2021 Foromopa BOSSOU Teyeouon Bounouma 27 605 Bounouma Kankore Gouecke 24 056 centre DISTANCES DES DISTRICTS SANITAIRES DE NZEREKORE Kobela 19 080 Centre de santé Distance N’Zérékoré_CS Poste de santé Distance CS_PS Koropara 23 898 KOULE SUD 9KM NYEMA 10 KM Sehipa Koule 23 756 C S SAMOE 12 KM NYAMPARA PELA 9 KM BOUNOUMA Thuo centre -

Guinea : Reference Map of N’Zérékoré Region (As of 17 Fev 2015)
Guinea : Reference Map of N’Zérékoré Region (as of 17 Fev 2015) Banian SENEGAL Albadariah Mamouroudou MALI Djimissala Kobala Centre GUINEA-BISSAU Mognoumadou Morifindou GUINEA Karala Sangardo Linko Sessè Baladou Hérémakono Tininkoro Sirana De Beyla Manfran Silakoro Samala Soromaya Gbodou Sokowoulendou Kabadou Kankoro Tanantou Kerouane Koffra Bokodou Togobala Centre Gbangbadou Koroukorono Korobikoro Koro Benbèya Centre Gbenkoro SIERRA LEONE Kobikoro Firawa Sassèdou Korokoro Frawanidou Sokourala Vassiadou Waro Samarami Worocia Bakokoro Boukorodou Kamala Fassousso Kissidougou Banankoro Bablaro Bagnala Sananko Sorola Famorodou Fermessadou Pompo Damaro Koumandou Samana Deila Diassodou Mangbala Nerewa LIBERIA Beindou Kalidou Fassianso Vaboudou Binemoridou Faïdou Yaradou Bonin Melikonbo Banama Thièwa DjénédouKivia Feredou Yombiro M'Balia Gonkoroma Kemosso Tombadou Bardou Gberékan Sabouya Tèrèdou Bokoni Bolnin Boninfé Soumanso Beindou Bondodou Sasadou Mama Koussankoro Filadou Gnagbèdou Douala Sincy Faréma Sogboro Kobiramadou Nyadou Tinah Sibiribaro Ouyé Allamadou Fouala Regional Capital Bolodou Béindou Touradala Koïko Daway Fodou 1 Dandou Baïdou 1 Kayla Kama Sagnola Dabadou Blassana Kamian Laye Kondiadou Tignèko Kovila Komende Kassadou Solomana Bengoua Poveni Malla Angola Sokodou Niansoumandou Diani District Capital Kokouma Nongoa Koïko Frandou Sinko Ferela Bolodou Famoîla Mandou Moya Koya Nafadji Domba Koberno Mano Kama Baïzéa Vassala Madina Sèmèkoura Bagbé Yendemillimo Kambadou Mohomè Foomè Sondou Diaboîdou Malondou Dabadou Otol Beindou Koindou -

Sitrep Ndeg 95 Epidemie De
RAPPORT DE SITUATION Nom de la maladie Maladie à Virus Ebola (MVE) Date de notification du 1er cas confirmé 13/02/2021 Date du rapport 19/05/2021 SitRep N°95 I. Points saillants ➢ J (-32) du compte à rebours des 42 jours ➢ 156 alertes reportées, 32 investiguées, 124 en cours d’investigation ➢ 90 nouvelles alertes dont 4 à Lola dont 38 investiguées • 29 alertes validées (7 décès, 2 swabés), 22 cas suspects (2 Hôpital, 3 sokoura, 2 Gonia, 4 Samoé, 5 Gouécké, 1 Mohomou, 1 Koropara, 1 Palé, 2 soulouta, 1 Koulé) • 3 Cas transférés aux CT-Epi (2 N’Zérékoré et 1 Gouécké) • 2 prélèvements à l’hôpital régional • 19 cas de Refus (2 Hôpital, 2 sokoura, 1 Gonia, 4 Samoé, 4 Gouécké, 1 Mohomou, 1 Koropara, 1 Palé, 2 soulouta, 1 Koulé) COU-SP en mode Réponse : 622 46 94 98/620 12 21 38 ; email : [email protected] Page 1 II. Dynamique de l’épidémie Tableau I. Répartition des cas dans le district sanitaire à la date du 19/05/2021, Description CU de N’Zérékoré Gouécké Soulouta Total Districts sanitaires Nouveau Cumul Nouveau Cumul Nouveau Cumul Nouveau Cumul Cas Suspects 17 17 5 5 0 0 22 22 Cas Confirmés 0 11 0 3 0 2 0 16* Cas Probables 0 4 0 0 0 3 0 7 *1 cas confirmé au CT-Epi de Nongo Tableau II. Situation des patients dans les centres de traitement épidémiologique et des décès à la date du 19/05/2021, Description N’Zérékoré Gouécké Total Districts sanitaires Nouveau Cumul Nouveau Cumul Nouveau Cumul Hospitalisés à Suspects 2 4 1 5 3 9 date Confirmés 0 0 0 0 0 0 Sortie non cas 4 90 1 21 5 111 Sorties guéris 0 9 0 0 0 9 Décès hospitaliers( CT-Epi) 0 5 0 0 0 5 Décès communautaires 7 473* 0 15 7 488 *1 cas pris en charge au CT-Epi de Conakry et 14 au CT-Epi de N’Zérékoré et 1 cas évadé *7 cas probables, 2 cas confirmés et 306 non cas, 113 décès non swabés Tableau III. -

A Methodology for Complex Agricultural Development Projects
Systemic Impact Evaluation: A Methodology for Complex Agricultural Development Projects. The Case of a Contract Farming Project in Guinea Jocelyne Delarue, Hubert Cochet To cite this version: Jocelyne Delarue, Hubert Cochet. Systemic Impact Evaluation: A Methodology for Complex Agri- cultural Development Projects. The Case of a Contract Farming Project in Guinea. The European Journal of Development Research, 2013, 25 (5), p.778-796. 10.1057/ejdr.2013.15. halshs-01374496 HAL Id: halshs-01374496 https://halshs.archives-ouvertes.fr/halshs-01374496 Submitted on 7 May 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Original Article Systemic Impact Evaluation: A Methodology for Complex Agricultural Development Projects. The Case of a Contract Farming Project in Guinea Jocelyne Delaruea and Hubert Cochetb aAgence Française de Développement, Evaluation and Capitalization Unit, Paris, France. E-mail: [email protected] bAgro Paris Tech, Comparative Agriculture and Agricultural Development Research Unit, Paris, France. E-mail: [email protected] Abstract This article presents a mixed-method approach used to analyse the impact of a complex agricultural development project, the SOGUIPAH (Guinean Oil Palms and Rubber Company) project designed to promote oil palm and rubber cultivation in Guinea. -
MCHIP Guinea End-Of-Project Report October 2010–June 2014
MCHIP Guinea End-of-Project Report October 2010–June 2014 Submitted on: September 15, 2014 Submitted to: United States Agency for International Development under Coooperative Agreement # GHS-A-00-08-00002-000 Submitted by: Yolande Hyjazi, Rachel Waxman and Bethany Arnold 1 The Maternal and Child Health Integrated Program (MCHIP) is the USAID Bureau for Global Health’s flagship maternal, neonatal and child health (MNCH) program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria, nutrition, and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. MCHIP brings together a partnership of organizations with demonstrated success in reducing maternal, newborn and child mortality rates and malnutrition. Each partner will take the lead in developing programs around specific technical areas: Jhpiego, as the Prime, will lead maternal health, family planning/reproductive health, and prevention of mother-to-child transmission of HIV (PMTCT); JSI—child health, immunization, and pediatric AIDS; Save the Children—newborn health, community interventions for MNCH, and community mobilization; PATH—nutrition and health technology; JHU/IIP—research and evaluation; Broad Branch—health financing; PSI—social marketing; and ICF International—continues support for the Child Survival and Health Grants Program (CSHGP) and the Malaria Communities Program (MCP). This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. -

Interim Report Government of Japan COUNTERING EPIDEMIC-PRONE
Government of Japan COUNTERING EPIDEMIC-PRONE DISEASES ALONG BORDERS AND MIGRATION ROUTE IN GUINEA Interim Report Project Period: 30 March 2016 – 29 March 2017 Reporting Period: 30 March 2016-31 August 2016 Funds: 2.000.000 USD Executing Organization: International Organization for Migration (IOM) Guinea October 2016 Interim Report to Government of Japan COUNTERING EPIDEMIC-PRONE DISEASES ALONG BORDERS AND MIGRATION ROUTES IN GUINEA Project Data Table Executing Organization: International Organization for Migration (IOM) Project Identification and IOM Project Code: MP.0281 Contract Numbers: Contract number: NI/IOM/120 Project Management Site Management Site: Conakry, CO, GUINEA and Relevant Regional Regional Office: Dakar, RO, SENEGAL Office: Project Period: 30 March 2016 – 29 March 2017 Geographical Coverage: Guinea Communal / Sub Prefectural / Prefectural / Regional Health authorities and Project Beneficiaries: Community members in Guinea Ministry of Health, National Health Security Agency, US Agency for international development (USAID), U.S. Office of Foreign Disaster Assistance Project Partner(s): (OFDA), Centre for Disease Control and Prevention (CDC), World Health Organization (WHO), International Medical Corps (IMC), Research triangle institute (RTI), Premieres Urgences (PU) Reporting Period: 30 March 2016 – 31 August 2017 Date of Submission: 30 October 2016 Total Confirmed 2,000,000 USD Funding: Total Funds Received to 2,000,000 USD Date: Total Expenditures: 439,761 USD Headquarters 17 route des Morillons • C.P. 71 • CH-1211 -

Key Considerations: 2021 Outbreak of Ebola in Guinea, the Context of N’Zérékoré
KEY CONSIDERATIONS: 2021 OUTBREAK OF EBOLA IN GUINEA, THE CONTEXT OF N’ZÉRÉKORÉ This brief summarises key considerations about the social, political and economic context shaping the outbreak of Ebola in the N’Zérékoré prefecture, Guinea, as of March 2021. The outbreak was declared on 14 February 2021, two weeks after the death of the first known case, a health agent (Agent Technique de Santé) from Gouécké. Gouécké is located 40km north of N’Zérékoré via the paved Route Nationale 2. The nurse sought care at a health centre in Gouécké, a clinic and then a traditional healer in N’Zérékoré. She died in N’Zérékoré on 28 January.1 When they became sick, the relatives of the first known case referred themselves to N’Zérékoré regional hospital, where the disease was transmitted to healthcare workers. Although the potential for transmission in rural areas of the Gouécké subprefecture was high, to date, most cases have been reported in the urban setting of N’Zérékoré, which is the focus of this brief. At the time of writing (22 March), the total number of cases was 18 (14 confirmed, four probable), with nine deaths and six recoveries. The last new case was reported on 4 March. N’Zérékoré city is the administrative capital of N’Zérékoré prefecture and N’Zérékoré region, and the largest urban centre of the Guinée Forestière area of south-east Guinea. It has an estimated population of 250,000, and is an important commercial, economic and transportation hub connecting Guinée Forestière to neighbouring Sierra Leone, Liberia and Côte d’Ivoire. -
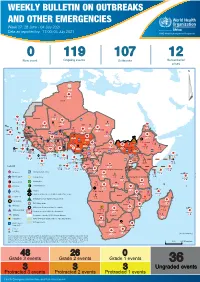
04 July 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 27: 28 June - 04 July 2021 Data as reported by: 17:00; 04 July 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 119 107 12 New event Ongoing events Outbreaks Humanitarian crises 64 0 141 471 3 755 Algeria ¤ 1 008 0 6 116 181 Mauritania 14 449 527 48 0 110 0 43 768 1 174 Niger 21 076 489 6 088 25 Mali 21 0 9 0 Cape Verde 6 471 16 4 951 174 Chad Eritrea Senegal 5 506 194 Gambia 66 0 32 705 287 1 414 8 Guinea-Bissau 847 17 Burkina Faso 2 060 56 276 435 4 331 167 859 2 121 Guinea 13 494 168 13 0 3 881 69 2 2 Benin 198 0 Nigeria 1 189 4 61 0 30 0 Ethiopia 13 2 6 995 50 556 5 872 15 Sierra Leone Togo 626 0 80 858 1 324 Ghana 7 141 98 Côte d'Ivoire 10 879 117 19 000 304 81 0 45 0 Liberia 17 0 South Sudan Central African Republic 1 313 2 0 25 0 50 14 0 96 317 796 6 738 221 Cameroon 23 807 294 3 0 48 594 315 35 173 196 7 0 58 0 199 2 1 411 30 9 1 620 1 185 868 3 675 2 0 168 0 1 1 5 748 104 14 069 131 2 0 8 759 122 Equatorial Guinea Uganda 867 2 827 9 Sao Tome and Principe 4 0 4 520 133 78 394 903 Kenya Gabon Legend Congo 3 307 90 305 26 Rwanda 8 199 104 2 376 37 42 585 470 25 076 159 Democratic Republic of the Congo 12 790 167 Burundi Measles Humanitarian crisis 5 521 8 Seychelles 42 181 960 435 0 693 57 Monkeypox Yellow fever United Republic of Tanzania 197 0 16 259 57 Meningitis Lassa fever 509 21 241 1 6 257 229 Leishmaniasis Cholera 95 703 913 164 282 2 443 Comoros Plague 304 3 cVDPV2 Angola Malawi Diarrhoeal disease in children under five years 36 926 1 208 726 0 3 -

Ecologically Sensitive Sites in Africa. Volume 1
Ecologically Sites in Africa Volume I: Occidental and Central Africa Benin Cameroon Central African Republic Congo Cdte d'lvoire Eq uatorlil^lllpvea aSon Guinea Complled'by the World Conservation Monitoring Centre For TK^^o^d Bdnk Ecologically Sensitive Sites in Africa Volume I: Occidental and Central Africa WORLD CONSERVATION! MONITORING CENTRE 2 4 MAY 1995 Compiled by PROTECTED AREAS | World Conservation Monitoring Centre Cambridge, UK for The World Bank Washington DC, USA The World Bank 1993 Published by The World Bank, Washington, DC, USA. Prepared by the World Conservation Monitoring Centre (WCMC), 219 Huntingdon Road, Cambridge, CB3 ODL, UK. WCMC is a joint venture between the three partners who developed The World Conservation Strategy and its successor Caring for the Earth: lUCN-World Conservation Union, UNEP-United Nations Environment Programme, and WWF- World Wide Fund for Nature. Its mission is to provide an information, research and assessment service on the status, security and management of the Earth's biological diversity as the basis for its conservation and sustainable use. Copyright: 1993 The World Bank Reproduction of this publication for educational or other non-commercial purposes is authorised without prior permission from the copyright holder. Reproduction for resale or other commercial purposes is prohibited without the prior written permission of the copyright holder. Citation: World Bank (1993). Ecologically Sensitive Sites in Africa. Volume I: Occidental and Central Africa. Compiled by the World Conservation Monitoring Centre for The World Bank, Washington, DC, USA. Printed by: The Burlington Press, Cambridge, UK. Cover illustration: Nairobi City Skyline with Kongoni and Grant's Gazelles, RIM Campbell. -

Guinea: Reference Map of N'zérékoré Prefecture
Guinea:ReferenceReference MapMap ofof NZérékoréN’Zérékoré Prefecture Prefecture(as (as of of 2612 MarchFev 2015)2015) Boola Mazana Kpamou Ouota LÖMOU CENTRE GOUNAGALAYE CENTRE KONI CENTRE Kognea Saadou Kpeïda MAKPOZOU CENTRE Founbandou Lokoa Koropara Lamineta FOOZOU CENTRE BOMA-NORD CENTRE Yessila Gbana Bahaïta Ouleoun KÔRÔH CENTRE KABIETA Kelèta KOLIWATA CENTRE Suokpayai PAMPARA CENTRE NYEMA-NORD CENTRE Gbohileta Bhoita BOWE NORD TOKPATA CENTRE Laine Zebela KEORAH CENTRE Womey KEREZAGAYE CENTRE Beneouli Göta ZENEMOUD CENTRE Nyonta GBEANTA CENTRE Seloh Loula KOYAH CENTRE Koule OUEYE CENTRE YOMATA CENTRE Oulela KOMATA CENTRE Bapet GOUECKE CENTRE Gouecke Vomou TAMOE CENTRE PAMPORE CENTRE Gnanakpalaye KPAI CENTRE Nyineta Guelagbozou BANZOU CENTRE KPOULO CENTRE ZOGBEANTA CENTRE Dapoloye Kpaya Gbonoma Yarakpara Soulouta Konia Benoita KPAGALAYE CENTRE Youwa NONA CENTRE MAOUON CENTRE KEREMANDA CENTRE Koronta GBOUO CENTRE ZOGOTA CENTRE Gbagonaye Belefanaye Koliyapoulou Powai SOUHOULE centre Kokota WEYA SUD Gouh GBAMBA CENTRE NIENH CENTRE Kpatié Yelewena Kobela NIAMPARA CENTRE Teaye Banzou Sud Kpeliyewoun 2 Batouata Woroyé Kpeliyewoun 1 NYEMA SUD CENTRE KONIPARA CENTRE Gbaita Duala GBILI CENTRE Nyalakpale GALAKPAYE CENTRE Ninguekpoye KOMOU CENTRE Weya Nord Domou 2 Samoi Domou 1 GBAYA CENTRE Lola KONIA AVIATION CENTRE Guela Boma Sud Bowe LOULE NORD KONALA CENTRE GBOTTOYE CENTRE MOATA CENTRE KOULE SUD CENTRE BANGOUETA CENTRE Galaye NYENSOKOURA 2 KARANA CENTRE KOLEYEBA NYEN 1 GONIA 3 BELLE VUE Zogoya MOHOMOU Lamou Wezou GBOYEBA Nzerekore NZAO CENTRE -

I. Points Saillants
RAPPORT DE SITUATION Nom de la maladie Maladie à Virus Ebola (MVE) Date de notification du 1er cas confirmé 13/02/2021 Date du rapport 27/05/2021 SitRep N°103 I. Points saillants ➢ J (-23) du compte à rebours des 42 jours ➢ 115 reports dont 30 investiguées 85 en cours d'investigations ➢ 122 Nouvelles alertes dont 4 décès de Lola avec 81 investiguées ; • 63 alertes validées (10 décès dont 7 swabées), 53 suspects (4 Hôpital, 10 Samoé,2 Sokoura, 5 Gouécké, 3 Dorota, 6 Mohomou, 3 Soulouta, 2 Bounouma, 1 Horoya, 1 Gonia, 4 Womey, 1 commercial, 2 Boma, 7 Yalenzou et 2 Koropara) ; • 4 Transférés aux CT-Epi (2 Gouécké et 2 Nzérékoré) ; • 4 Prélèvements à l'hôpital Régional de N'zérékoré ; • 49 cas de refus au transfert (4 Hôpital, 9 Samoé, 2 Sokoura, 3 Gouécké, 2 Dorota, 6 Mohomou, 3 Soulouta, 2 Bounouma, 1 Horoya, 1 Gonia, 4 Womey, 1 commercial, 2 Boma, 7 Yalenzou et 2 Koropara); COU-SP en mode Réponse : 622 46 94 98/620 12 21 38 ; email : [email protected] Page 1 II. Dynamique de l’épidémie Tableau I. Répartition des cas dans le district sanitaire à la date du 27/05/2021, Description CU de N’Zérékoré Gouécké Soulouta Total Districts sanitaires Nouveau Cumul Nouveau Cumul Nouveau Cumul Nouveau Cumul Cas Suspects 45 45 5 5 3 3 53 53 Cas Confirmés 0 11 0 3 0 2 0 16* Cas Probables 0 4 0 0 0 3 0 7 *1 cas pris en charge au CT-Epi de Conakry et 14 au CT-Epi de N’Zérékoré et 1 cas évadé Tableau II. -

Page 1 GE.18-20123 (E) 100119 Committee on the Rights of The
United Nations CRC/C/GIN/Q/3-6/Add.1 Convention on the Distr.: General 23 November 2018 Rights of the Child English Original: French English, French and Spanish only Committee on the Rights of the Child Eightieth session 14 January–1 February 2019 Item 4 of the provisional agenda Consideration of reports of States parties List of issues in relation to the combined third to sixth periodic reports of Guinea Addendum Replies of Guinea to the list of issues* [Date received: 16 November 2018] * The present document is being issued without formal editing. GE.18-20123 (E) 100119 CRC/C/GIN/Q/3-6/Add.1 Part One 1. Please indicate whether the necessary steps have been taken to expedite the revision of national legislation, particularly the Children’s Code and the Civil Code, with a view to making it fully compliant with the principles and provisions of the Convention. 1. Necessary measures have been taken in the context of the revision of national legislation, including in relation to the Children’s Code. It has already been considered once by the Council of Ministers; subsequently, an interministerial committee was established to address the concerns of the other departments concerned and the amendments suggested by the Council of Ministers. It was transmitted to the General Secretariat of the Government for consideration, adoption and submission to the National Assembly by the end of 2018. 2. As for the Civil Code, it is already before the National Assembly and its consideration has begun; it is due to be voted on and adopted shortly.