Health Cluster Update, June 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nutrition Update
Monthly FSAU Food Security Analysis Unit - Somalia NUTRITION UPDATE MARCH 2005 OVERVIEW This issue highlights the significant improvement in nutritional In this issue of ‘Nutrition Update’; status recorded in the Lower Nugal Valley along with some NW Somalia – sentinel site surveillance 1 stabilisation of malnutrition levels in surveillance sites in the Sool Lower Juba Nutrition Update 2 Plateau. NE Somalia – sentinel site surveillance 3 Northern Gedo Update 4 In areas of NE Somalia hit by multiple shocks, extreme coping Somali Region, Ethiopia Update 5 strategies and the ongoing humanitarian interventions have Nutrition assessment plan for 2005 6 prevented a deterioration in the nutritional status. In Northern Gedo, the poor nutrition situation persists and admissions of severely malnourished children for therapeutic feeding remain high. Plans for the establishment of a sentinel site surveillance in the area are underway. Preliminary results of a survey in Somali Region Ethiopia indicate a critical nutrition situation as Jilaal season starts. SOOL PLATEAU AND LOWER NUGAAL SENTINEL SURVEILLANCE RESULT Significant decline in levels of malnutrition in Lower Nugal Valley 1 Las Qoray/ A significant decline in malnutrition was observed within Lower Nugal Badhan Valley, compared to the past round of sentinel sites surveillance in SANAG November 2004 (global acute malnutrition 33.9% (CI: 28.2 – 40.1). El Afwein Erigavo Diarrhoea was significantly associated with cases of malnutrition. Of the Xingalool Owrboogeys ð 268 under-five children assessed in Lower Nugal valley, 17.2% (CI: 12.8% ð Sarmaanyo - 22.2%) were malnourished (weight for height <-2 Z score or oedema) and Xudun Caynaba Godaalo Taleh ð ð 3.7% (CI: 1.8% - 6.7%) were severely malnourished (weight for height <-3 Xudun Carrooley Legend SOOL ð Z score or oedema). -

Pdf | 119.79 Kb
Somalia Humanitarian Update Highlights March 2005 Political: The Somalia Transition Federal Government selected Baidoa and Jowhar as temporary reloca- tion sites. In the last week of March fighting ensued in Baidoa. The situation remains tense. Food Security: Inside this issue: Despite sufficient Deyr rains that helped to end a four years drought and is expected to result in good harvests, many parts of Somalia continue to experience food insecurity especially Aw- dal region in Somaliland where malnutrition of children under five years is 20.3%. Food Security 2 Security: Hargeisa and the route to Mandera and Gebiley were last month downgraded from UN Secu- Health and 2 rity Phase 4 to 3 while the rest of Somaliland remained on Phase 4. Nutrition Tsunami Update 3 Tsunami Update: Emergency needs in tsunami affected areas have largely been met. About 5% of the popula- tion is in a state of humanitarian emergency while 40% are experiencing livelihood crisis, re- Security quiring assistance until the next fishing season. CAP 2005 : Funding for projects within the Somalia CAP 2005 remain low with only 3% of the Access 4 appealed funds covered as of 7th April, 2005. CAP 2005 Funding status Protection; 4 IDPs New Government identifies relocation sites in Somalia his month saw a series of develop- security is restored in Mogadishu. However, ments unfold around the Transition the vote took place in the absence of about Federal Government’s (TFG) reloca- 10 out of 74 ministers, who left the meeting. T th tion and the deployment of a peace support Fighting erupted in Baidoa on 26 mission. -

Somalian Turvallisuustilanne 28.6.2016
1 (42) MUISTIO MIG-168269 06.03.00 MIGDno-2016-706 28.06.2016 SOMALIAN TURVALLISUUSTILANNE KESÄKUUSSA 2016 Sisällysluettelo 1. Yleiset turvallisuusolosuhteet ...................................................................................... 2 2. Konfliktin vaikutukset siviiliväestöön ............................................................................ 7 3. Turvallisuustilanne alueittain tammi - toukokuussa 2016 ........................................... 10 3.1. Lower Jubba ............................................................................................................. 11 3.2. Gedo ......................................................................................................................... 12 3.3. Bay ............................................................................................................................ 14 3.4. Bakool ....................................................................................................................... 15 3.5. Middle Jubba ............................................................................................................. 15 3.6. Lower Shabelle ......................................................................................................... 15 3.7. Benadir - Mogadishu ................................................................................................. 18 3.8. Middle Shabelle ......................................................................................................... 22 3.9. Hiiraan ..................................................................................................................... -
Gedo Intercluster Initial Investigation – September
INTER -AGENCY DROUGHT ASSESSMENT IN LOWER JUBA REGION OF SOMALIA JANUARY 2017 INTER-AGENCY DROUGHT ASSESSMENT IN LOWER JUBA REGION – JANUARY 2017 Table of contents Executive summary -------------------------------------------------------------------------------------- 2 Key findings --------------------------------------------------------------------------------------------- 2 Recommendations --------------------------------------------------------------------------------------- 3 Acronyms, abbreviations and definitions of Somalia terminologies --------------------------- 6 Acknowledgement ----------------------------------------------------------------------------------------- 7 Introduction /context of the inter-agency assessment -------------------------------------------- 8 Methodology ------------------------------------------------------------------------------------------------ 9 Assessment findings -------------------------------------------------------------------------------------- 10 Impact of drought ------------------------------------------------------------------------------------------ 10 Findings by cluster ----------------------------------------------------------------------------------------- 10 Food Security and Livelihoods --------------------------------------------------------------- 10 Education ------------------------------------------------------------------------------------------ 12 Nutrition -------------------------------------------------------------------------------------------- 13 Water, Sanitation -

Afmadow District Detailed Site Assessment Lower Juba Region, Somalia
Afmadow district Detailed Site Assessment Lower Juba Region, Somalia Introduction Location map The Detailed Site Assessment (DSA) was triggered in the perspectives of different groups were captured2. KI coordination with the Camp Coordination and Camp responses were aggregated for each site. These were then Management (CCCM) Cluster in order to provide the aggregated further to the district level, with each site having humanitarian community with up-to-date information on an equal weight. Data analysis was done by thematic location of internally displaced person (IDP) sites, the sectors, that is, protection, water, sanitation and hygiene conditions and capacity of the sites and the humanitarian (WASH), shelter, displacement, food security, health and needs of the residents. The first round of the DSA took nutrition, education and communication. place from October 2017 to March 2018 assessing a total of 1,843 sites in 48 districts. The second round of the DSA This factsheet presents a summary of profiles of assessed sites3 in Afmadow District along with needs and priorities of took place from 1 September 2018 to 31 January 2019 IDPs residing in these sites. As the data is captured through assessing a total of 1778 sites in 57 districts. KIs, findings should be considered indicative rather than A grid pattern approach1 was used to identify all IDP generalisable. sites in a specific area. In each identified site, two key Number of assessed sites: 14 informants (KIs) were interviewed: the site manager or community leader and a women’s representative, to ensure Assessed IDP sites in Afmadow4 Coordinates: Lat. 0.6, Long. -

World Bank Final Report
The Common Social Accountability Platform Deploying the Common Social Accountability Platform to inform the 2020 World Bank Performance and Learning Review January 2020 Africa’s Voices Project Team: Africa’s Voices Project Team: Anna Tomson (Governance & Accountability Senior Programme Manager), Khadija Mohamed (Programme Officer), Nasri Ali (Programme Officer), Zakaria Sheikh (Research Assistant), Alexander Simpson (Software Engineer), Lucas Malla (Senior Quantitative Researcher), and Samuel Kimeu (Executive Director). © 2019 Africa’s Voices Foundation Ltd Africa’s Voices Foundation Africa’s Voices Foundation Kenya Riverside Suites, Riverside Lane, Nairobi UK Centre for Global Equality, 8C King’s Parade CB2 1SP Cambridge africasvoices.org @africas_voices This report was written by Anna Tomson, Senior Programme Manager, Governance & Accountability and Khadija Hussein at Africa’s Voices Foundation 2 Africa’s Voices Foundation List of acronyms 4 1. INTRODUCTION 5 1.1 Context 5 1.2 Project Objectives 5 1.3 The Common Social Accountability Platform 6 1.4 AVF’s Interactive Radio Method 6 2. Methodology 8 2.1 Building inclusive community engagement at scale 8 2.2 Gathering insight on public opinion 10 2.3 Limitations of the methodology 10 3. Engagement 11 3.1 Content of the radio dialogue 11 3.2 Who participated in the dialogue 11 4. Insights into citizen perspectives 14 4.1 Citizen priorities for development 14 4.2 Citizen access to decision making and grievance mechanisms 21 ANNEX 1: List of radio stations 26 ANNEX 2: Thick description 27 ANNEX -

SOMALIA Food Security Update March 2009 Issued in Collaboration with FAO/Food Security Analysis Unit (FSAU)
SOMALIA Food Security Update March 2009 Issued in collaboration with FAO/Food Security Analysis Unit (FSAU) • The consensus Climate Outlook Forum (COF23) recently Figure 1. Current estimated food security convened in Mombasa, Kenya has forecast an increased conditions (January to March 2009) likelihood of below normal gu (April‐June) rainfall in parts of southern and central Somalia due to the presence of a La Niña, a phenomenon which is associated with drier‐than‐ normal conditions in Eastern Africa. • Due to poor deyr rains in late 2008 and a harsh Jilaal (January‐March) dry season, water sources in many areas, including the central regions, parts of Gedo, Hiran, and Juba, have dried up earlier than normal, leading to water shortages. A deepening of the water crisis can be expected through the onset of the gu rains in mid‐April. • A decline in remittance inflows has occurred during the last several months following the global recession and a subsequent increase in unemployment among the Somali diaspora in Europe and North America. This may contribute to a further deterioration in food security among urban populations. Source: FSAU and FEWS NET Seasonal calendar and critical events Source: FEWS NET Current food security situation Food security in most of south and central Somalia continues to be affected by the impact of poor deyr production in 2008/09, uncertain market conditions, civil insecurity, unstable income sources, hyperinflation, and exorbitant prices for food and other essential commodity. As a result, 3.2 million people, including about 700,000 urban dwellers, are highly or extremely food insecure (Figure 1). -

Gedo Region – Situation Analysis
Gedo Region – Situation Analysis Context Gedo Region, the second largest region in Somalia, lies on the Somalia borders with Ethiopia and Kenya, and shares borders with four Somali regions of Bay, Bakool and Middle Jubba and Lower Jubba. It has an estimated total population of 328,3781, with a 75/25 rural/urban divide.The region is home to 76,510 IDPs2. UNHCR estimates that 16,380 IDPs arrived in Luuq, 30,000 in Doloow, and approximately 18,000 in Belet Xaawo. Gedo has six administrative districts: Garbaharey, Baardheere (the capital), Ceel Waaq in the south and Belet Xaawo, Doloow, and Luuq in the north. Two major rivers run through the region, the Dawa and the Juba. The Dawa River runs along the border of Ethiopia into Somalia’s Gedo region. The Jubba River starts from Doloow, just north of Luuq district, and flows to Buur Dhuubo and Baardheere. The economy mostly depends on rearing livestock and farming, but also has strong inter-regional and international cross-border trade with Kenya and Ethiopia, to some extent. In the northern zone the pastoralists rear sheep, goats, camels and cows. The agro-pastoral zone extends from east to west below Guban. The riverine zone extends from east to west below West Golis and is mainly a farming area where crops such as sorghum are produced. The security and access situation in north Gedo, in particular to Luuq, has relatively improved for the United Nations and International NGOs. The area is controlled by the Somali National Army forces backed by Ethiopian forces. South Gedo is more insecure due to continued clashes and greater access for Al-Shabaab (AS) in the rural areas of Garbaharey, Buur Dhuubo and Baardheere. -

From the Bottom
Conflict Early Warning Early Response Unit From the bottom up: Southern Regions - Perspectives through conflict analysis and key political actors’ mapping of Gedo, Middle Juba, Lower Juba, and Lower Shabelle - SEPTEMBER 2013 With support from Conflict Dynamics International Conflict Early Warning Early Response Unit From the bottom up: Southern Regions - Perspectives through conflict analysis and key political actors’ mapping of Gedo, Middle Juba, Lower Juba, and Lower Shabelle Version 2 Re-Released Deceber 2013 with research finished June 2013 With support from Conflict Dynamics International Support to the project was made possible through generous contributions from the Government of Norway Ministry of Foreign Affairs and the Government of Switzerland Federal Department of Foreign Affairs. The views expressed in this paper do not necessarily reflect the official position of Conflict Dynamics International or of the Governments of Norway or Switzerland. CONTENTS Abbreviations 7 ACKNOWLEDGMENT 8 Conflict Early Warning Early Response Unit (CEWERU) 8 Objectives 8 Conflict Dynamics International (CDI) 8 From the Country Coordinator 9 I. OVERVIEW 10 Social Conflict 10 Cultural Conflict 10 Political Conflict 10 II. INTRODUCTION 11 Key Findings 11 Opportunities 12 III. GEDO 14 Conflict Map: Gedo 14 Clan Chart: Gedo 15 Introduction: Gedo 16 Key Findings: Gedo 16 History of Conflict: Gedo 16 Cross-Border Clan Conflicts 18 Key Political Actors: Gedo 19 Political Actor Mapping: Gedo 20 Clan Analysis: Gedo 21 Capacity of Current Government Administration: Gedo 21 Conflict Mapping and Analysis: Gedo 23 Conflict Profile: Gedo 23 Conflict Timeline: Gedo 25 Peace Initiative: Gedo 26 IV. MIDDLE JUBA 27 Conflict Map: Middle Juba 27 Clan Chart: Middle Juba 28 Introduction: Middle Juba 29 Key Findings: Middle Juba 29 History of Conflict : Middle Juba 29 Key Political Actors: Middle Juba 29 Political Actor Mapping: Middle Juba 30 Capacity of Current Government Administration: Middle Juba 31 Conflict Mapping and Analysis: Middle Juba 31 Conflict Profile: Middle Juba 31 V. -

Upper Tribunal (Immigration and Asylum Chamber) AMM and Others (Conflict; Humanitarian Crisis; Returnees; FGM) Somalia CG [2011
Upper Tribunal (Immigration and Asylum Chamber) AMM and others (conflict; humanitarian crisis; returnees; FGM) Somalia CG [2011] UKUT 00445 (IAC) THE IMMIGRATION ACTS Heard at Field House Determination Promulgated On 13 to 21 June and 15 July 2011 ………………………………… Before UPPER TRIBUNAL JUDGE LATTER UPPER TRIBUNAL JUDGE P R LANE UPPER TRIBUNAL JUDGE KEKIĆ Between AMM MW ZF FM AF Appellants and THE SECRETARY OF STATE FOR THE HOME DEPARTMENT Respondent THE UNITED NATIONS HIGH COMMISSIONER FOR REFUGEES Intervening © CROWN COPYRIGHT 2011 Representation: For Appellants AMM: Ronan Toal, instructed by South Manchester Law Centre For Appellant MW: Harriet Short, instructed by Avon & Bristol Community Law Centre For Appellant ZF: Mark Schwenk, instructed by Parker Rhodes Hickmotts, Solicitors For Appellant FM: Mark Symes, instructed by Wilson Solicitors LLP For Appellant AF: Ronan Toal, instructed by Wilson Solicitors LLP For the Respondent: Tim Eicke QC and Christopher Staker, instructed by the Treasury Solicitor For the UNHCR: Tom Hickman, instructed by Baker & McKenzie LLP Law 1) Whilst section 2 of the Human Rights Act 1998 and its associated case law requires United Kingdom tribunals in general to give effect to the jurisprudence of the European Court of Human Rights, including that Court’s guidance on how to approach evidence in international protection cases, the weighing of evidence and the drawing of conclusions as to the relative weight to be placed on items of evidence adduced before a United Kingdom tribunal are ultimately matters for that tribunal. Whilst the factual finding the Strasbourg Court has made as a result of applying its own guidance is something to which the domestic tribunal must have regard, pursuant to section 2, it is not bound to reach the same finding. -
Somalia from Resilience Towards Recovery and Development
Report No.34356-SO Report No. 34356-SO Somalia From Resilience Towards Recovery and Development Public Disclosure Authorized Public Disclosure Authorized A Country Economic Memorandum for Somalia January 11, 2006 Poverty Reduction and Economic Management 2 Country Department for Somalia Africa Region Somalia and Development Recovery Towards Resilience From Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of the World Bank GFATM Global Fund to Fight Aids, Tuberculosis and Malaria ICAO International Civil Aviation Organization ICRC International Committee ofthe Red Cross IDA International Development Association IDP Internally Displaced People IFAD International Fund for Agriculture Development IFC International Finance Corporation IMF International Monetary Fund ITCZ Inter-Tropical Convergence Zone ITU International Telecommunication Union JNA Joint Needs Assessment KPHIS Kenya Plant Health Inspectorate Service KSA Kingdom of Saudi Arabia LDC Least Developed Country LICUS Low Income Countries under Stress MCH Maternal and Child Health MDG MillenniumDevelopment Goal MDRP Multi-Country Demobilization and Reintegration Program MDTF Multi-Donor Trust Fund MICS Multi Indicators Cluster Survey NGO NonGovernmental Organization ODA Official Development Assistance OECD Organization of Economic Cooperation and Development PHC Primary Health Care RRA Rahanweyn Residtance Army PRS Poverty Reduction Strategy SACB Somalia -
With Funding Status of Each Report As
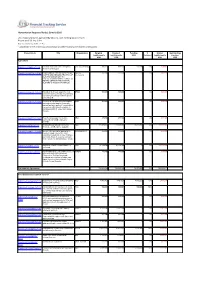
Humanitarian Response Plan(s): Somalia 2016 List of appeal projects (grouped by Cluster), with funding status of each Report as of 23-Sep-2021 http://fts.unocha.org (Table ref: R3) Compiled by OCHA on the basis of information provided by donors and recipient organizations. Project Code Title Organization Original Revised Funding % Unmet Outstanding requirements requirements USD Covered requirements pledges USD USD USD USD Agriculture SOM-16/A/84942/5110 Puntland and Lower Juba Emergency VSF (Switzerland) 998,222 998,222 588,380 59% 409,842 0 Animal Health Support SOM-16/A/86501/15092 PROVISION OF FISHING INPUTS FOR SAFUK- 352,409 352,409 0 0% 352,409 0 YOUTHS AND MEN AND TRAINING OF International MEN AND WOMEN ON FISH PRODUCTION AND MAINTENANCE OF FISHING GEARS IN THE COASTAL REGIONS OF MUDUG IN SOMALIA. SOM-16/A/86701/14592 Integrated livelihoods support to most BRDO 500,000 500,000 0 0% 500,000 0 vulnerable conflict affected 2850 farming and fishing households in Marka district Lower Shabelle. SOM-16/A/86746/14852 Provision of essential livelihood support HOD 500,000 500,000 0 0% 500,000 0 and resilience building for Vulnerable pastoral and agro pastoral households in emergency, crisis and stress phase in Kismaayo district of Lower Juba region, Somalia SOM-16/A/86775/17412 Food Security support for destitute NRO 499,900 499,900 0 0% 499,900 0 communities in Middle and Lower Shabelle SOM-16/A/87833/123 Building Household and Community FAO 111,805,090 111,805,090 15,981,708 14% 95,823,382 0 Resilience and Response Capacity SOM-16/A/88141/17597 Access to live-saving for population in SHARDO Relief 494,554 494,554 0 0% 494,554 0 emergency and crises of the most vulnerable households in lower Shabelle and middle Shabelle regions, and build their resilience to withstand future shocks.