The Project on Improvement of Health Service Through
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Evaluation of Antiretroviral Therapy Information System in Mbale Regional Referral Hospital, Uganda
EVALUATION OF ANTIRETROVIRAL THERAPY INFORMATION SYSTEM IN MBALE REGIONAL REFERRAL HOSPITAL, UGANDA. PETER OLUPOT-OLUPOT A mini-thesis submitted in partial fulfillment of the requirements for the degree of Master of Public Health in the School of Public Health, University of the Western Cape. SUPERVISOR: DR. GAVIN REAGON February 2009 1 KEY WORDS Health Information Systems HIV/AIDS ART Data Quality Timeliness Data Accuracy Data analysis Data use Use of information Availability 2 ACRONYMS AIDS Acquired Immune Deficiency Syndrome ACP AIDS Control Program ART Antiretroviral Therapy ART-IS Antiretroviral Therapy Information System ARV Antiretroviral CD4 Cluster of Differentiation 4 CDC Centers for Disease Control and Prevention EBR Electronic Based Records GFATM Global Fund to fight AIDS, Tuberculosis & Malaria GOU Government of Uganda IDC Infectious Disease Clinic IMR Infant Mortality Rate HAART Highly Active Antiretroviral Therapy HIS Health Information Systems HISP Health Information System Project HIT Health Information Technology HIV Human Immunodeficiency Virus HMIS Health Management Information Systems MAP Multi-country AIDS Program MMR Maternal Mortality Rate MOH Ministry of Health MPH Master of Public Health MRRH Mbale Regional Referral Hospital 3 NGO Non Governmental organization OI Opportunistic Infection OpenMRS Open Medical Record System PBR Paper Based Record PDA Personal Digital Assistant PEPFAR President’s (USA) Emergency Plan for AIDS Relief PLWA People Living with HIV/AIDS RHINONET Routine Health Information Network SOPH School of Public Health SSA Sub – Saharan Africa STI Sexually Transmitted Infection TASO The AIDS Support Organization TB Tuberculosis U5MR Under Five Mortality Rate UN United Nations UNAIDS United Nations Joint Program on AIDS UWC University of the Western Cape VCT Voluntary Counseling and Testing WHO World Health Organization 4 About the Evaluation The ART – IS at Mbale regional referral hospital is still an infant system which has been in operation for only 3 years. -
Annual Health Sector Performance Report
THE REPUBLIC OF UGANDA Annual Health Sector Performance Report Financial Year 2006/2007 October 2007 Blank Page Foreword The health sector in FY 2006/07 implemented the 2nd Year of the Health Sector Strategic Plan II (HSSP II). The focus has been on scaling up interventions and consolidating reforms initiated during the HSSP I and in the 1st Year of the HSSP II in order to achieve the Poverty Eradication Action Plan (PEAP) objectives and Millennium Development Goals (MDGs). The Uganda Demographic and Health Survey 2006 shows that there have been improvements in Infant Mortality Rate, Under5 Mortality Rate and Total Fertility Rate. The data is not conclusive on Maternal Mortality Ratio. These improvements in health outcomes indicate that it is indeed possible to make a difference in the life of Ugandans. The improvements in health outcomes were contributed to by different sectors; however the contribution of the health sector in terms of stewardship and advocacy, and improved coverage with good quality services for preventive, promotive and curative has been key. The AHSPR 2006/07 documents sector performance against agreed HSSP II indicators and Year II targets. The AHSPR 2006/07 indicates fairly good performance as shown by the performance against the 8 PEAP and HSSP II indicators. The sector performance for FY 2006/07 was on or above target for 3 indicators namely: Couple Years of Protection (CYP) a measure of family planning uptake; Proportion of children below 1 year that have received pentavalent vaccine 3rd dose; and New OPD attendance per capita. Sector performance was below target for 3 indicators namely: Proportion of deliveries taking place in government and PNFP health facilities; Proportion of health facilities with tracer medicines all the time (i.e. -

Environmental Consequences of Sand Mining on the Shores of Lake Victoria: a Case of Study of Kiyirira Village Katabi Sub Countø’, ~4 Akiso District
Environmental Consequences of Sand mining on the shores of Lake Victoria: A case of study of Kiyirira Village Katabi Sub CountØ’, ~4 akiso District By LUUTU IVAN BEM/0993/21 /DU Supervised by DR. TWAHA BASAMBA ALl A research Report submitted in partial fulfillment of thep ward of the degree in Bachelor of En~ ironmental management of Kampala International University SEPTEMBER 2005 DECLARA ION I, Luutu Ivan, I declare that, this work is original and has not been submitted in part or whole, to any institution of higher learning or any University for any degree or other award. The s~urces of information quoted in here have been duly acknowledged. Signature~~~ Date ~OtO5 LUUTU IVAN This dissertation has been submitted with ñiy a~proval as the University supervisor. Signature.. Date..9— DR. TWAHA BASAMBA ALT DEDICAnON This work is dedicated to my Lord, Jesus Christ~ my dear family especially my mother, Ms. Nakalinzi Sarah who toiled to see me through my academic, arena and my late grandfather, Mr. Mukasa Joseph. 4 II ACNowLEJ~EME~ I acknowledge with sincere apprecia~joj and gratitude the assistance given to me by various people. Special thanks are extended to my supervi~ i.e. Dr. Twaha Basamba Au, Miss Tumushabe Ann and Mrs. Abesiga Nancy for their guidance, suggestio~ and encouragement through out the study. Lastly, am also grateful to my father, Mr. ICizito George, my brother and sisters, ICayizzi Henry, Namubiru Flavta, Namutebi Diana Vicky, my uncles, aunties as well as my grandmothe~~ I cannot also forget my colleagues who assisted me in one way or another when I needed their suppoft and encouragement especially, Ireri, Ammon, I4adija, Gibson, Peter, Henry, Opira and the rest. -

Vol. CX No. 25 5Th May, 2017
THE REPUBLIC OF UGANDA THE REPUBLIC OF UGANDA Registered at the — General Past Officefor transmission within East Africa as a Newspaper Hiettiuedl ty Vol. CX No. 25 5th May, 2017 Price: Shs. 5,000 yr CONTENTS PAGE General Notice No. 348 of 2017. The Marriage Act—Notice... ae sais 433 The Companies Act—Notices.. F wise 433 THE COMPANIES ACT, LAWS OF UGANDA,2000. The Electoral Commission Act—Notices ... 434-436 (Cap. 110). The Bank of Uganda Act—Notices_... .. 437-438 The Electricity ‘Act—Notices 439-440 NOTICE. The Trademarks Act— Registration of Applications 440-446 PURSUANT to Section 40(4) of the Companies Act, (No. Advertisements.. w. 446-452 SUPPLEMENTS 1/2012) Laws of Uganda, 2000, notice is hereby given that Statutory Instruments KIKAGATE SERVICE STATION LIMITED,has been by a No. 21—The Non-Governmental Organisations (Fees) special resolution passed on 14th March, 2017, and with the Regulations, 2017. approval of the Registrar of Companies, changed in nameto No. 22—The Non-Governmental Organisations Regulations, EDDIES' SERVICE STATION LIMITED, and that such 2017. No, 23—The Electoral Commission (Appointment of Date of new name has been entered in myRegister. Completion of Update of Voters' Register in Tororo Dated at Kampala, this 15th day of March, 2017. District) Instrument, 2017. AYALO VIVIENNE, CORRIGENDUM Assistant Registrar of Companies. Take notice that General Notice No. 276 of 2017, was erroneously advertised in The Uganda Gazette Vol. CX, No. 20 of 5th April, 2017. The name was wrongly typeset as General Notice No. 349 of 2017. Namusoke Rose instead of NAMUKOSE ROSE, the THE COMPANIES ACT, LAWS OF UGANDA,2000. -

Buwate Sports Academy
Buwate Sports Academy Date: Prepared by: October 31, 2018 Naku Charles Lwanga I. Demographic Information 1. City & Province: Buwate, Uganda 2. Organization: Real Medicine Foundation Uganda (www.realmedicinefoundation.org) Mother Teresa Children’s Foundation (www.mtcf-uk.org/) 3. Project Title: Buwate Sports Academy 4. Reporting Period: July 1, 2018 – September 30, 2018 5. Project Location (region & city/town/village): Buwate Village, Kira Town Council, Wakiso District, Kampala, Uganda 6. Target Population: The children and population of Buwate II. Project Information 7. Project Goal: Develop the youth advancement and economic components of our humanitarian work through games, sports training, vocational training, and other educational opportunities. 8. Project Objectives: • Provide funding to assist the operations and growth of Buwate Sports Academy. • Provide funding to allow children from surrounding slums to attend school. • Provide funding for vocational training opportunities, etc. 9. Summary of RMF/MTCF-sponsored activities carried out during the reporting period under each project objective (note any changes from original plans): • School fees were paid for 85 children in Buwate Sports Academy, with funds from RMF. • Buwate Sports Academy organized and held holiday sports programs for the academy children, and welcomed children back to school with serious training for the categories of under-3, under-9, under-11, under-13, and under-16. • Buwate Sports Academy participated in the under-16 category in the Airtel Rising Stars national tournament, held at the Villa Park Nsambya sports grounds in Kampala. Buwate children won with a score of 2-0 against Nsambya Soccer Academy, thus making it to the district tournament level. -

Psychiatric Hospitals in Uganda
Psychiatric hospitals in Uganda A human rights investigation w www.mdac.org mentaldisabilityadvocacy @MDACintl Psychiatric hospitals in Uganda A human rights investigation 2014 December 2014 ISBN 978-615-80107-7-1 Copyright statement: Mental Disability Advocacy Center (MDAC) and Mental Health Uganda (MHU), 2014. All rights reserved. Contents Foreword ...................................................................................................................................................................................................... 4 Executive summary ......................................................................................................................................................................................................... 6 1. Introduction, torture standards and hospitals visited.............................................................................................................................. 9 1(A). The need for human rights monitoring........................................................................................................................................................... 9 1(B). Uganda country profile .................................................................................................................................................................................... 10 1(C). Mental health ................................................................................................................................................................................................... -

3.3 Current Situation and Key Issues of the Public Transport Sector in Gkma
Final Report The Study on Greater Kampala Road Network and Transport Improvement in the Republic of Uganda November 2010 3.3 CURRENT SITUATION AND KEY ISSUES OF THE PUBLIC TRANSPORT SECTOR IN GKMA 3.3.1 OVERVIEW OF THE PUBLIC TRANSPORT The privately owned Uganda Transport Company (UTC) held the exclusive franchise for bus services in Kampala until its nationalization in 1972. At that time, its only competition came from shared taxis which are saloon or estate cars. Following its nationalization, UTC contracted and focused more closely on its long-distance services. As a result, the market for urban transport services in Kampala became open to private sector operators using small minibus vehicles. In 1994 a commercial vehicle distributor established City Link as a private-sector large bus operation with some 40 vehicles in service. However, UTODA was able to organize an effective competition to this initiative. City Link meanwhile did not succeed by operating similar to that of minibus services based on fill-and-run principle, rather than operating based on scheduled services. Thus, the company shortly collapsed. Feedback from these results indicates that although City Link was popular, its operations were too thinly spread over the network and were not able to provide a reliable service. Public transport passengers within Kampala have very limited choice such as minibus services or motorcycle services with the majority as minibus services locally called taxis. 3.3.2 TAXI/MINIBUS Main supply of public transport in Kampala is now by minibuses, which are known locally as taxi (photographs bellow). KCC estimated that in 2003, there were nearly 7,000 minibuses based in the GKMA. -
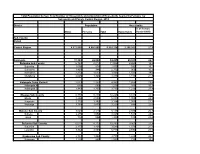
Population by Parish
Total Population by Sex, Total Number of Households and proportion of Households headed by Females by Subcounty and Parish, Central Region, 2014 District Population Households % of Female Males Females Total Households Headed HHS Sub-County Parish Central Region 4,672,658 4,856,580 9,529,238 2,298,942 27.5 Kalangala 31,349 22,944 54,293 20,041 22.7 Bujumba Sub County 6,743 4,813 11,556 4,453 19.3 Bujumba 1,096 874 1,970 592 19.1 Bunyama 1,428 944 2,372 962 16.2 Bwendero 2,214 1,627 3,841 1,586 19.0 Mulabana 2,005 1,368 3,373 1,313 21.9 Kalangala Town Council 2,623 2,357 4,980 1,604 29.4 Kalangala A 680 590 1,270 385 35.8 Kalangala B 1,943 1,767 3,710 1,219 27.4 Mugoye Sub County 6,777 5,447 12,224 3,811 23.9 Bbeta 3,246 2,585 5,831 1,909 24.9 Kagulube 1,772 1,392 3,164 1,003 23.3 Kayunga 1,759 1,470 3,229 899 22.6 Bubeke Sub County 3,023 2,110 5,133 2,036 26.7 Bubeke 2,275 1,554 3,829 1,518 28.0 Jaana 748 556 1,304 518 23.0 Bufumira Sub County 6,019 4,273 10,292 3,967 22.8 Bufumira 2,177 1,404 3,581 1,373 21.4 Lulamba 3,842 2,869 6,711 2,594 23.5 Kyamuswa Sub County 2,733 1,998 4,731 1,820 20.3 Buwanga 1,226 865 2,091 770 19.5 Buzingo 1,507 1,133 2,640 1,050 20.9 Maziga Sub County 3,431 1,946 5,377 2,350 20.8 Buggala 2,190 1,228 3,418 1,484 21.4 Butulume 1,241 718 1,959 866 19.9 Kampala District 712,762 794,318 1,507,080 414,406 30.3 Central Division 37,435 37,733 75,168 23,142 32.7 Bukesa 4,326 4,711 9,037 2,809 37.0 Civic Centre 224 151 375 161 14.9 Industrial Area 383 262 645 259 13.9 Kagugube 2,983 3,246 6,229 2,608 42.7 Kamwokya -

Office of the Auditor General the Republic of Uganda
OFFICE OF THE AUDITOR GENERAL THE REPUBLIC OF UGANDA REPORT OF THE AUDITOR GENERAL ON THE FINANCIAL STATEMENTS OF MBALE REGIONAL REFERRAL HOSPITAL FOR THE YEAR ENDED 30TH JUNE 2016 Table of Contents LIST OF ACROYNMS ................................................................................................................................................. 2 1.0 INTRODUCTION ............................................................................................................................................ 5 2.0 AUDIT OBJECTIVES ..................................................................................................................................... 5 3.0 AUDIT PROCEDURES PERFORMED .......................................................................................................... 6 4.0 ENTITY FINANCING ..................................................................................................................................... 6 5.0 FINDINGS ....................................................................................................................................................... 7 5.1 Categorization of Findings ............................................................................................................................... 7 5.2 Summary of Findings ....................................................................................................................................... 7 6.0 DETAILED AUDIT FINDINGS .................................................................................................................... -

Vote:752 Entebbe Municipal Council Quarter2
Local Government Quarterly Performance Report FY 2017/18 Vote:752 Entebbe Municipal Council Quarter2 Terms and Conditions I hereby submit Quarter 2 performance progress report. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:752 Entebbe Municipal Council for FY 2017/18. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Accounting Officer, Entebbe Municipal Council Date: 29/08/2019 cc. The LCV Chairperson (District) / The Mayor (Municipality) 1 Local Government Quarterly Performance Report FY 2017/18 Vote:752 Entebbe Municipal Council Quarter2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Ushs Thousands Approved Budget Cumulative Receipts % of Budget Received Locally Raised Revenues 4,313,592 2,705,669 63% Discretionary Government Transfers 6,002,056 766,052 13% Conditional Government Transfers 7,609,309 3,043,100 40% Other Government Transfers 30,000 5,751,205 19171% Donor Funding 0 0 0% Total Revenues shares 17,954,957 12,266,026 68% Overall Expenditure Performance by Workplan Ushs Thousands Approved Cumulative Cumulative % Budget % Budget % Releases Budget Releases Expenditure Released Spent Spent Planning 124,414 45,109 61,869 36% 50% 137% Internal Audit 47,230 22,879 22,879 48% 48% 100% Administration 1,609,033 872,146 872,146 54% 54% 100% Finance 1,049,758 1,051,096 1,051,096 100% 100% 100% Statutory Bodies 1,122,556 664,327 664,327 -

Assessment Form
Local Government Performance Assessment Tororo District (Vote Code: 554) Assessment Scores Accountability Requirements % Crosscutting Performance Measures 61% Educational Performance Measures 76% Health Performance Measures 82% Water & Environment Performance Measures 79% 554 Accountability Requirements 2019 Tororo District Definition of No. Summary of requirements Compliance justification Compliant? compliance Annual performance contract 1 Yes LG has submitted an annual • From MoFPED’s The LG submitted an Annual performance contract of the inventory/schedule of LG Performance Contract on 7/7/2019 forthcoming year by June 30 on the submissions of through the on line platform basis of the PFMAA and LG Budget performance contracts, [email protected] and received by guidelines for the coming financial check dates of MoFPED on the same day. A year. submission and Physical Copy was also submitted to issuance of receipts and: MoFPED, on 17th July 2019 vide submission letter dated 15th July o If LG submitted 2019 reference CR/213/12 before or by due date, then state ‘compliant’ o If LG had not submitted or submitted later than the due date, state ‘non- compliant’ • From the Uganda budget website: www.budget.go.ug, check and compare recorded date therein with date of LG submission to confirm. Supporting Documents for the Budget required as per the PFMA are submitted and available 2 Yes LG has submitted a Budget that • From MoFPED’s The LG submitted a Budget for FY includes a Procurement Plan for the inventory of LG budget 2019/2020 on 7/07/2019 through the forthcoming FY by 30th June (LG submissions, check on line platform [email protected] PPDA Regulations, 2006). -
3Rd Annual Report 3.9.22.1248:3Rd Annual Report
The Power of Partnerships: The President’s Emergency Plan for AIDS Relief Third Annual Report to Congress The Power of Partnerships: The President’s Emergency Plan for AIDS Relief Third Annual Report to Congress Cover Photo Through HIV counseling and testing for couples at the U.S.-supported Kericho District Hospital, Joyce and David found out they are infected with HIV. Joyce was four months pregnant with her second child at the time of diagnosis. Thanks to the clinic’s program to prevent mother-to-child HIV transmission, Joyce delivered a baby boy who is HIV-negative. After a year of antiretroviral treatment, David has also gained weight and feels healthy – enabling him to provide for his family. Photo by Doug Shaffer This report was prepared by the Office of the United States Global AIDS Coordinator in collaboration with the United States Departments of State (including the United States Agency for International Development), Defense, Commerce, Labor, Health and Human Services (including the Centers for Disease Control and Prevention, the Food and Drug Administration, the Health Resources and Services Administration, the National Institutes of Health, the Substance Abuse and Mental Health Services Administration, and the Office of Global Health Affairs), and the Peace Corps. 2 ❚ The Power of Partnerships: The President’s Emergency Plan for AIDS Relief CONTENTS Acronyms and Abbreviations . 5 Overview – The Power of Partnerships . 9 Chapter 1 – Critical Intervention in the Focus Countries: Prevention. 27 Chapter 2 – Critical Intervention in the Focus Countries: Treatment . .55 Chapter 3 – Critical Intervention in the Focus Countries: Care . .79 Chapter 4 – Building Capacity: Partnerships for Sustainability .