View PDF Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The New Right
W&M ScholarWorks Dissertations, Theses, and Masters Projects Theses, Dissertations, & Master Projects 1984 The New Right Elizabeth Julia Reiley College of William & Mary - Arts & Sciences Follow this and additional works at: https://scholarworks.wm.edu/etd Part of the Political Science Commons Recommended Citation Reiley, Elizabeth Julia, "The New Right" (1984). Dissertations, Theses, and Masters Projects. Paper 1539625286. https://dx.doi.org/doi:10.21220/s2-mnnb-at94 This Thesis is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Dissertations, Theses, and Masters Projects by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. THE NEW RIGHT 'f A Thesis Presented to The Faculty of the Department of Sociology The College of William and Mary in Virginia In Partial Fulfillment Of the Requirements for the Degree of Master of Arts by Elizabeth Reiley 1984 This thesis is submitted in partial fulfillment of the requirements for the degree of Master of Arts Elizabeth Approved, May 1984 Edwin H . Rhyn< Satoshi Ito Dedicated to Pat Thanks, brother, for sharing your love, your life, and for making us laugh. We feel you with us still. Presente! iii. TABLE OF CONTENTS Page ACKNOWLEDGEMENTS ........................... v ABSTRACT.................................... vi INTRODUCTION ................................ s 1 CHAPTER I. THE NEW RIGHT . '............ 6 CHAPTER II. THE 1980 ELECTIONS . 52 CHAPTER III. THE PRO-FAMILY COALITION . 69 CHAPTER IV. THE NEW RIGHT: BEYOND 1980 95 CHAPTER V. CONCLUSION ............... 114 BIBLIOGRAPHY .................................. 130 ACKNOWLEDGMENTS The writer wishes to express her appreciation to all the members of her committee for the time they gave to the reading and criticism of the manuscript, especially Dr. -

CE02487 Project
Date Printed: 06/16/2009 JTS Box Number: IFES 76 Tab Number: 74 Document Title: Project V.O.T.E Document Date: May-96 Document Country: United States -- Texas Document Language: English IFES ID: CE02487 Project o o o Voters of Tomorrow through Education I May/June 1996, Vol. 6, No.2 !'\ Message from ~he~ecretary Honorary Board Members ~ '\ Has it Teal~ been a ;~'{T? That's the ques- Kay Bailey Hutchison tion I'm asking rilyself as I sil-down to write this u.s. Senalor column. Yes, anpther school ye1u-, is drawing t.o a _".,." .•,,,-,, •• ·/7 cl0:-e. Tea~hers;md students are aI~:ady making . ,.""",_w,,'- / theIr vacauon plans. But before we'tum out the.~...... 'George W. Bush/ classroom lights~or the summer, I wa'riuo·take;;' Governor ,/ moment to revietv what has happened during the / course of this f995-96 school year. And for i' Project V.Q.T:E:, what a year it's been! Dan Mo.?,es ".,..,.",.,.~""" Attorney/General T he biggestne~;'~::es with regard to the continued growth of // our program'. Ten new charter sites were added this year. Let's welcome Mi'''ch' I M 0.""'- ."' ae oses ":th\t.~ewestmembers of the Project V.O.T.E. family: Temple ISO, Clear Commissioner of Educalion CreeJ(·'ISD,.~vin ISO, Amarillo ISO, Lubbock ISO, Abilene ISO, Teias Education Agency Tatum ISO, Klein'IS,Q.~ Brenh,am ISO, and Brownsville ISO. It's great "\ to have all of you on board"".. \ """':"'0<>.: ~ " ....,'l< George Bayoud, Jr. With the addition of these conlmunities, the Project V.O.T.E. -

John Schmitz
Excerpted from Brad Koplinski, HATS IN THE RING: CONVERSATIONS WITH PRESIDENTIAL CANDIDATES (Presidential Publishing: North Bethesda, Maryland, 2000) John Schmitz Born: August 12, 1930 in Milwaukee, Wisconsin Election in which he ran for president: 1972 Party: American Offices held: California State Senator 1965 - 1970 and 1978 - 1982 United States Congressman 1970 - 1973 Entered the race: August 2, 1972 - Washington, D.C. Stopped campaigning: November 7, 1972 - When Richard Nixon was re-elected president Strategy: Run to the right of President Richard Nixon, exposing his vulnerability on the conservative wing of the Republican Party. Make a credible showing to build the party for success in future elections. Best finish: Third place in Idaho (28,869 votes - 9.3 percent) Total votes: 1,099,482 Amount raised: $533,000 Current residence: Washington, Virginia and Washington, D.C. Current activities: Serving as President of Chapelle Charlemagne Vineyards. Interesting facts: Owns the townhouse where Wisconsin Senator Joseph McCarthy lived while serving in the United States Senate. Officially changed his registration from the Republican Party to the American Party upon receiving the latter's presidential nomination, thereby making him the first and only member of the American Party to serve in Congress. Elected to the California State Senate in 1964, John Schmitz made a name for himself by advocating conservative causes that other Republicans feared to support. He was the first member of the ultra-conservative John Birch Society to serve in the body. When asked about his membership in the group, Schmitz Jokingly replied that he "had to do something to get the middle-of-the-road vote" in conservative Orange County. -

Congressional Record United States Th of America PROCEEDINGS and DEBATES of the 105 CONGRESS, FIRST SESSION
E PL UR UM IB N U U S Congressional Record United States th of America PROCEEDINGS AND DEBATES OF THE 105 CONGRESS, FIRST SESSION Vol. 143 WASHINGTON, WEDNESDAY, FEBRUARY 5, 1997 No. 13 House of Representatives The House met at 11 a.m. and was THE JOURNAL of our colleague, the Honorable Frank called to order by the Speaker pro tem- Tejeda; The SPEAKER pro tempore. The Whereas Representative Tejeda has spent 4 pore [Mr. LAHOOD]. Chair has examined the Journal of the years in the House of Representatives; f last day's proceedings and announces Whereas Representative Tejeda served his to the House his approval thereof. country honorably in the United States Ma- DESIGNATION OF THE SPEAKER Pursuant to clause 1, rule I, the Jour- rine Corps from 1963 to 1967; and Whereas Representative Tejeda was award- PRO TEMPORE nal stands approved. ed the Purple Heart, the Silver Star, the The SPEAKER pro tempore laid be- Ms. ROS-LEHTINEN. Mr. Speaker, Commandant's Trophy, the Marine Corps As- fore the House the following commu- pursuant to clause 1, rule I, I demand a sociation Award, and the Colonel Phil nication from the Speaker: vote on agreeing to the Speaker's ap- Yeckel Award for ``the best combined record proval of the Journal. in leadership, academics, and physical fit- WASHINGTON, DC, The SPEAKER pro tempore. The ness'': Now, therefore, be it February 5, 1997. Resolved, ThatÐ I hereby designate the Honorable RAY question is on the Chair's approval of (1) when the Senate adjourns today, it ad- LAHOOD to act as Speaker pro tempore on the Journal. -

Congressional Record United States Th of America PROCEEDINGS and DEBATES of the 105 CONGRESS, FIRST SESSION
E PL UR UM IB N U U S Congressional Record United States th of America PROCEEDINGS AND DEBATES OF THE 105 CONGRESS, FIRST SESSION Vol. 143 WASHINGTON, TUESDAY, FEBRUARY 4, 1997 No. 12 House of Representatives The House met at 12:30 p.m. and was will he be remembered for his admira- ing the insidious barriers that once called to order by the Speaker pro tem- ble courage as a Vietnam veteran and a confronted African-Americans and pore [Mr. GUTKNECHT]. scholarly education at Harvard and other minorities in tuition broadcast- f Yale, but FRANK's true dedication and ing. He helped bring the change by allegiance to the people of the 28th being the best, both in sports and in DESIGNATION OF SPEAKER PRO Congressional District of Texas will re- news coverage. For that historic and TEMPORE main in the hearts and minds of his proud achievement, we are all in his The SPEAKER pro tempore laid be- constituency. debt. fore the House the following commu- In fact, whenever there was an issue I am confident that his future plans, nication from the Speaker: affecting his district or whenever we whatever they may be, will include a needed a vote from FRANK TEJEDA, he continuing contribution to his commu- WASHINGTON, DC, nity and his country. Whether these February 4, 1997. would always say two words: Wilson I hereby designate the Honorable GIL County. Whenever he saw me on the plans include award-winning broad- GUTKNECHT to act as Speaker pro tempore on House floor and we were trying to get casts like those he anchored from Afri- this day. -

Guide to the Lambert C. Mims Papers
Guide to the Lambert C. Mims Papers Descriptive Summary: Creator: Lambert C. Mims, 1930-2008 Title: Lambert C. Mims Papers Dates: 1820-2003 (bulk 1965-1989) Quantity: 160.5 linear feet Abstract: Papers agendas, audio tapes, books, campaign material, correspondence, flyers, legal material, magazines, maps, negatives, news clippings, notes, pamphlets, photographs, plaques, reports, slides, speeches, and video tapes. Covers a multitude of local subjects typically found within such political collections. Accession: 06-09-459 ; 459-2006 Biographical Note: Lambert C. Mims was born in 1930 in Uriah, Alabama. He moved to Mobile, Alabama, in 1949 and worked as a salesman before co-founding, a year later, a feed company, and, in 1965, branching out on his own. Lambert Mims was public works commissioner and rotating mayor of Mobile from 1965 to 1985. During Mims' time as mayor/commissioner, the city of Mobile experienced the latter part of the modern civil rights movement, completed the Bayway, and unveiled the George C. Wallace Tunnel. It opened Mobile Greyhound Park and saw the Southern Market/City Hall designated a national historic landmark. It reconstructed and opened Fort Condé and celebrated the nation's bicentennial. It witnessed the devastating destruction of hurricanes Camille and Frederic and saw the first oil well drilled in the bay. It witnessed the completion of the I-65 link across the Mobile-Tensaw Delta and celebrated the opening of the Tennessee-Tombigbee Waterway. When first elected, Mims was the youngest city commissioner in Mobile's history. Upon leaving office, Governor George Wallace appointed Mims as his ambassador to the Alabama Waterways Development Agency, a position he held from 1985 until March 1987, and one in which he promoted the Tennessee-Tombigbee Waterway. -
Special Election Dates
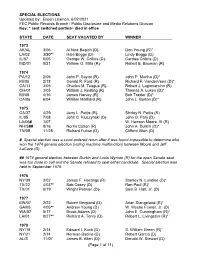
SPECIAL ELECTIONS Updated by: Eileen Leamon, 6/02/2021 FEC Public Records Branch / Public Disclosure and Media Relations Division Key: * seat switched parties/- died in office STATE DATE SEAT VACATED BY WINNER 1973 AK/AL 3/06 Al Nick Begich (D)- Don Young (R)* LA/02 3/20** Hale Boggs (D)- Lindy Boggs (D) IL/07 6/05 George W. Collins (D)- Cardiss Collins (D) MD/01 8/21 William O. Mills (R)- Robert E. Bauman (R) 1974 PA/12 2/05 John P. Saylor (R)- John P. Murtha (D)* MI/05 2/18 Gerald R. Ford (R) Richard F. VanderVeen (D)* CA/13 3/05 Charles M. Teague (R)- Robert J. Lagomarsino (R) OH/01 3/05 William J. Keating (R) Thomas A. Luken (D)* MI/08 4/16 James Harvey (R) Bob Traxler (D)* CA/06 6/04 William Mailliard (R) John L. Burton (D)* 1975 CA/37 4/29 Jerry L. Pettis (R)- Shirley N. Pettis (R) IL/05 7/08 John C. Kluczynski (D)- John G. Fary (D) LA/06# 1/07 W. Henson Moore, III (R) NH/S## 9/16 Norris Cotton (R) John A. Durkin (D)* TN/05 11/25 Richard Fulton (D) Clifford Allen (D) # Special election was a court-ordered rerun after it was found impossible to determine who won the 1974 general election (voting machine malfunction) between Moore and Jeff LaCaze (D). ## 1974 general election between Durkin and Louis Wyman (R) for the open Senate seat was too close to call and the Senate refused to seat either candidate. Special election was held in September 1975. -
TCU DAILY SKIFF Light and Variable
IRA RALEIGH, N.C. (API—The federal gianni—ll says three totricm Among the government's star witnesses are Bruton's ex-partner, Binford Records, when they were kept, often listed dead or fictitious people as mav have conspired to ^hip *W|Mwn am) ammunition from here to the Benton, and former worker John Bulla, both granted immunitv in exchange purchasers. Benton said. outlawed Irish Republican Arms for their testimons Asked where the guns were going. DeMeo replied, "someplace cool and I .meminent prosecutors also believe the owner of a gun shop in nearby Benton, who pleaded guilts in 1978 to one violation of federal firearms green," Benton recalled. Wilson, N C, conspired with two New York men to -hip 80 to 100 high- laws and received a suspended sentence, testified last week he sold 80 to "They were stockpiling them and then shipping them out of the country." powered guns to Ireland along with a million rounds ot ammunition 100 guns, many off-the-record, to DeMeo and Ferraro on Bruton's orders. Weapons that prosecutors are trying to link to the three defendants began alleged)) stolen from the Camp leieune Marine base When Kerraro first visited B and B Gun Shop in 1972. he "indicated that turning up in Ireland and Britain from 1975 to 1979 On trial in the U S. District Court gun-smuggling case are Howard he wanted to bus militarv-type weapons, and he didn't want any records After a 1975 siege of a London apartment house where IRA members had Bruton. owner of the B and B lain Shop in Wilson, Robert Ferraro of New kept of it," Benton testified. -

Joint General Ad Special Election Media Report
Media 19961105 Joint Bexar County CUMULATIVE Joint General and Special Election MEDIA FORMAT November 5, 1996 Page 1 Total Number Voting 365777 Of 744672 49.11 % Boxes Reporting 599 Of 599 100.00 % Straight Party Republican 79024 42.47 % Democratic 105103 56.49 % Libertarian 936 0.50 % Natural Law 246 0.13 % U.S. Taxpayers 741 0.39 % President and Vice President Bob Dole/Jack Kemp-R 161619 44.55 % Bill Clinton/Al Gore-D 180308 49.70 % Harry Browne/Jo Jorgensen-L 1668 0.46 % John Hagelin/Mike Tompkins-N 242 0.06 % Howard Phillips/H. W. Titus-U 445 0.12 % Ross Perot/James Campbell-I 17822 4.91 % United States Senator Phil Gramm-R 172193 47.80 % Victor M. Morales-D 183426 50.91 % Michael Bird-L 3631 1.00 % John Huff-N 982 0.27 % United States Representative, Dist. 20 James Walker-R 47616 34.40 % Henry B. Gonzalez-D 88190 63.71 % Alejandro (Alex) De Pena-L 2156 1.55 % Lyndon Felps-N 447 0.32 % United States Representative, Dist. 21 Lamar Smith-R 58924 76.89 % Gordon H. Wharton-D 16989 22.17 % Randy Rutenbeck-N 712 0.92 % United States Representative, Dist. 23 Henry Bonilla-R 41067 77.01 % Charles P. Jones-D 11339 21.26 % Linda J. Caswell-N 918 1.72 % United States Representative, Dist. 28 Mark L. Cude-R 19529 21.87 % Frank Tejeda-D 68810 77.06 % Clifford Finley-N 946 1.06 % Railroad Commissioner Carole Keeton Rylander-R 182059 52.26 % Hector Uribe-D 157846 45.31 % Rick Draheim-L 6361 1.82 % Paul Pigue-N 2046 0.58 % Chief Justice, Supreme Court Tom Phillips-R 174233 50.34 % Andrew Jackson Kupper-D 161261 46.59 % David Parker-L 10605 3.06 % Justice, Supreme Court, Place 1 John Cornyn-R 167047 48.55 % Page 1 Media 19961105 Joint Patrice Barron-D 169230 49.18 % Thomas Stults-L 7764 2.25 % Justice, Supreme Court, Place 2 James A. -

CONGRESSIONAL RECORD—HOUSE June 26, 1997
June 26, 1997 CONGRESSIONAL RECORD Ð HOUSE H4651 served 7 years as a gunner in World H. RES. 176 Our Nation could have lost control of War II, he went to work for Lorene's Resolved, That upon the adoption of this its destiny, but this Congress took ac- father, where they first met. resolution it shall be in order, any rule of tion to save Medicare, pass a balanced After they wed, they lived on a small the House to the contrary notwithstanding, budget and provide massive tax relief farm in Harrisonville, GA, and every to consider a concurrent resolution provid- for our families. These are truly his- day Grover commuted to Hapeville, ing for adjournment of the House and Senate toric accomplishments. for the Independence Day district work Independence Day is a time to cele- GA, to work for Ford Motor Co. During period. this time, Lorene worked at Callaway brate the birth of this Nation and the Mills until she decided to quit in order The SPEAKER pro tempore (Mr. perseverance of the Founding Fathers to raise their three children. In 1975, UPTON). The gentleman from Georgia who fought the heavy hand of govern- Grover and Lorene sold the farm and (Mr. LINDER) is recognized for 1 hour. ment and oppressive taxes. The budget went to work for Milliken Mills until Mr. LINDER. Mr. Speaker, for the passed by this Congress reduces the op- their retirement in the late 1980's. purpose of debate only, I yield the cus- pressive taxes on American families In addition to working hard and rais- tomary 30 minutes to the gentleman and balances the budget. -

CONGRESSIONAL RECORD — Extensions of Remarks E1209 Billions of People Around the World
June 27, 1996 CONGRESSIONAL RECORD Ð Extensions of Remarks E1209 billions of people around the world. We are af- Secretary Christopher are far reaching. They Americans need to send Congress the mes- fected by the actions of other countries that are the necessary mission for the United sage that their health is not for sale to special create ozone depleting substances, overfish States to carry forward. I rise in recognition interest groups. Mr. Speaker, I ask that the and dump low-level radioactive waste in the and with deep respect for what Secretary Texas Observer article ``It's the Environment, world's oceans, deplete our world's Christopher has set forth. It is environmental Stupid,'' be printed in the RECORD so Ameri- rainforests, and stress our Earth's ecosystem statecraft. cans know how important their response to through overpopulation. f this bill is to protect their environment and Secretary Christopher pointed out that the health. Thank you. needs of the American people are not well THE BARTON CLEAN AIR ACT [From the Texas Observer, June 14 1996] served if our foreign policy does not address AMENDMENTS IT'S THE ENVIRONMENT, STUPID these global concernsÐwe may be ``Ameri- (By Louis DuBose) cans,'' but we live on a planet that does not HON. ROSA L. DELAURO Phil Gramm got the message in January recognize geopolitical boundaries. OF CONNECTICUT when his pollster advised him that Repub- In his speech, Secretary Christopher pointed IN THE HOUSE OF REPRESENTATIVES lican voters don't trust their own party on out that environmental forces not only ``tran- environmental issues. -

FNBT NEWS First National Bank & Trust Co
FNBT NEWS First National Bank & Trust Co. Serving central and southwest Oklahoma since 1892 CONTACT: Randy Talley, SVP Marketing, 405-224-2200 July 3, 2014 FNBT Supports Juneteenth Celebration in Chickasha Chickasha’s salute to tHe abolition of slavery in America received support tHis year from First National Bank & Trust Co. The local celebration was Held on June 21. From left are FNBT Appraisal Compliance Manager Candace Jones, CHickasHa civic leader and former City Councilman James Dorn, and FNBT President Walt Voss. WHAT IS JUNETEENTH? CHICKASHA COMMUNITY JUNETEENTH CELEBRATION ON JUNE 21, 2014 Juneteenth, also known as Juneteenth Independence Day, Freedom Day, or Emancipation Day, is a holiday in the United States that commemorates the announcement of the abolition of slavery in the U.S. state of Texas in 1865, and more generally the emancipation of African-American citizens throughout the United States. Celebrated on June 19, the term is a portmanteau of June and nineteenth and is recognized as a state holiday or special day of observance in most states. During the US Civil War, President Abraham Lincoln issued the Emancipation Proclamation on September 22, 1862, with an effective date of January 1, 1863. Although it declared that slaves were to be freed in the Confederate States of America in rebellion against the federal government, Texas did not act to comply with the Emancipation Proclamation. On June 18, 1865, Union General Gordon Granger and 2,000 federal troops arrived on the island of Galveston, Texas, to take possession of the state and enforce the emancipation of its slaves. On June 19, standing on the balcony of Galveston’s Ashton Villa, Granger read the contents of "General Order No.