Role of Platelets in Restenosis After Percutaneous Coronary Revascularization
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplementary Table 1: Adhesion Genes Data Set
Supplementary Table 1: Adhesion genes data set PROBE Entrez Gene ID Celera Gene ID Gene_Symbol Gene_Name 160832 1 hCG201364.3 A1BG alpha-1-B glycoprotein 223658 1 hCG201364.3 A1BG alpha-1-B glycoprotein 212988 102 hCG40040.3 ADAM10 ADAM metallopeptidase domain 10 133411 4185 hCG28232.2 ADAM11 ADAM metallopeptidase domain 11 110695 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 195222 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 165344 8751 hCG20021.3 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 189065 6868 null ADAM17 ADAM metallopeptidase domain 17 (tumor necrosis factor, alpha, converting enzyme) 108119 8728 hCG15398.4 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 117763 8748 hCG20675.3 ADAM20 ADAM metallopeptidase domain 20 126448 8747 hCG1785634.2 ADAM21 ADAM metallopeptidase domain 21 208981 8747 hCG1785634.2|hCG2042897 ADAM21 ADAM metallopeptidase domain 21 180903 53616 hCG17212.4 ADAM22 ADAM metallopeptidase domain 22 177272 8745 hCG1811623.1 ADAM23 ADAM metallopeptidase domain 23 102384 10863 hCG1818505.1 ADAM28 ADAM metallopeptidase domain 28 119968 11086 hCG1786734.2 ADAM29 ADAM metallopeptidase domain 29 205542 11085 hCG1997196.1 ADAM30 ADAM metallopeptidase domain 30 148417 80332 hCG39255.4 ADAM33 ADAM metallopeptidase domain 33 140492 8756 hCG1789002.2 ADAM7 ADAM metallopeptidase domain 7 122603 101 hCG1816947.1 ADAM8 ADAM metallopeptidase domain 8 183965 8754 hCG1996391 ADAM9 ADAM metallopeptidase domain 9 (meltrin gamma) 129974 27299 hCG15447.3 ADAMDEC1 ADAM-like, -

Datasheet: MCA740PE Product Details
Datasheet: MCA740PE Description: MOUSE ANTI HUMAN CD42b:RPE Specificity: CD42b Other names: GPIB-ALPHA Format: RPE Product Type: Monoclonal Antibody Clone: AK2 Isotype: IgG1 Quantity: 100 TESTS Product Details Applications This product has been reported to work in the following applications. This information is derived from testing within our laboratories, peer-reviewed publications or personal communications from the originators. Please refer to references indicated for further information. For general protocol recommendations, please visit www.bio-rad-antibodies.com/protocols. Yes No Not Determined Suggested Dilution Flow Cytometry Neat Where this antibody has not been tested for use in a particular technique this does not necessarily exclude its use in such procedures. The suggested working dilution is given as a guide only. It is recommended that the user titrates the antibody for use in his/her own system using appropriate negative/positive controls. Target Species Human Product Form Purified IgG conjugated to R. Phycoerythrin (RPE) - lyophilized Reconstitution Reconstitute with 1 ml distilled water Max Ex/Em Fluorophore Excitation Max (nm) Emission Max (nm) RPE 488nm laser 496 578 Preparation Purified IgG prepared by affinity chromatography on Protein A from tissue culture supernatant Buffer Solution Phosphate buffered saline Preservative 0.09% Sodium Azide Stabilisers 1% Bovine Serum Albumin 5% Sucrose External Database Links UniProt: P07359 Related reagents Entrez Gene: 2811 GP1BA Related reagents Page 1 of 3 Specificity Mouse anti Human CD42b antibody, clone AK2 recognizes the human CD42b cell surface antigen, also known as platelet glycoprotein GP1B. CD42b is expressed by platelets and megakaryocytes. Clone AK2 has been reported to block the binding of von Willebrand Factor (VWF) to platelets Flow Cytometry Use 10ul of the suggested working dilution to label 100ul whole blood. -

TPMS Technology to Infer Biomarkers of Macular Degeneration Prognosis
bioRxiv preprint doi: https://doi.org/10.1101/625889; this version posted May 2, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. TPMS technology to infer biomarkers of macular degeneration prognosis in in silico simulated prototype-patients under the study of heart failure treatment with sacubitril and valsartan Guillem Jorba1,*, Joaquim Aguirre-Plans2,*, Valentin Junet1, Cristina Segú-Vergés1, José Luis Ruiz1, Albert Pujol1, NarCis Fernandez-Fuentes3, José Manuel Mas1, Baldo Oliva2 1AnaxomiCs BioteCh SL, BarCelona 08008, Catalonia, Spain 2StruCtural BioinformatiCs Group, ResearCh Programme on BiomediCal InformatiCs, Department of Experimental and Health ScienCe, Universitat Pompeu Fabra, BarCelona 08003, Catalonia, Spain 3Department of BiosCienCes, U ScienCe TeCh, Universitat de ViC-Universitat Central de Catalunya, ViC 08500, Catalonia, Spain *These authors Contributed equally to this work and are Considered to be Co-first authors Brief running title TPMS for in silico simulations of patients Corresponding author Baldo Oliva & José Manuel Mas Manuscript keywords: - In SiliCo CliniCal Trials - CardiovasCular Diseases - Heart Failure - Adverse effeCts - MaCular Degeneration - Comorbidity Authorship Confirmation Statement: JAP, GJ, CSV, JMM & BO analysed the data. GJ, VJ, CSV, JLR & JMM studied HF and MD with TPMS. AP, GJ, JLR & JMM desCribed the methods of TPMS. JAP, NFF & BO desCribed the methods of GUILDify. CSV & JMM analysed and desCribed the potential biomarkers for MD adverse effects by sacubitril/valsartan. JAP, NFF & BO Compared the results of TPMS with GUILDify. -

Datasheet: MCA740B Product Details
Datasheet: MCA740B Description: MOUSE ANTI HUMAN CD42b:Biotin Specificity: CD42b Other names: GPIB-ALPHA Format: Biotin Product Type: Monoclonal Antibody Clone: AK2 Isotype: IgG1 Quantity: 0.1 mg Product Details Applications This product has been reported to work in the following applications. This information is derived from testing within our laboratories, peer-reviewed publications or personal communications from the originators. Please refer to references indicated for further information. For general protocol recommendations, please visit www.bio-rad-antibodies.com/protocols. Yes No Not Determined Suggested Dilution Flow Cytometry Neat Where this antibody has not been tested for use in a particular technique this does not necessarily exclude its use in such procedures. The suggested working dilution is given as a guide only. It is recommended that the user titrates the antibody for use in his/her own system using appropriate negative/positive controls. Target Species Human Product Form Purified IgG conjugated to Biotin - liquid Preparation Purified IgG prepared by affinity chromatography on Protein A from tissue culture supernatant. Buffer Solution Phosphate buffered saline Preservative 0.09% Sodium Azide Stabilisers 1% Bovine Serum Albumin Approx. Protein IgG concentration 0.1 mg/ml Concentrations External Database Links UniProt: P07359 Related reagents Entrez Gene: 2811 GP1BA Related reagents Specificity Mouse anti Human CD42b antibody, clone AK2 recognizes the human CD42b cell surface antigen, also known as platelet glycoprotein GP1B. CD42b is expressed by platelets and Page 1 of 3 megakaryocytes. Clone AK2 has been reported to block the binding of von Willebrand Factor (VWF) to platelets Flow Cytometry Use 10ul of the suggested working dilution to label 100ul whole blood. -

Supp Table 6.Pdf
Supplementary Table 6. Processes associated to the 2037 SCL candidate target genes ID Symbol Entrez Gene Name Process NM_178114 AMIGO2 adhesion molecule with Ig-like domain 2 adhesion NM_033474 ARVCF armadillo repeat gene deletes in velocardiofacial syndrome adhesion NM_027060 BTBD9 BTB (POZ) domain containing 9 adhesion NM_001039149 CD226 CD226 molecule adhesion NM_010581 CD47 CD47 molecule adhesion NM_023370 CDH23 cadherin-like 23 adhesion NM_207298 CERCAM cerebral endothelial cell adhesion molecule adhesion NM_021719 CLDN15 claudin 15 adhesion NM_009902 CLDN3 claudin 3 adhesion NM_008779 CNTN3 contactin 3 (plasmacytoma associated) adhesion NM_015734 COL5A1 collagen, type V, alpha 1 adhesion NM_007803 CTTN cortactin adhesion NM_009142 CX3CL1 chemokine (C-X3-C motif) ligand 1 adhesion NM_031174 DSCAM Down syndrome cell adhesion molecule adhesion NM_145158 EMILIN2 elastin microfibril interfacer 2 adhesion NM_001081286 FAT1 FAT tumor suppressor homolog 1 (Drosophila) adhesion NM_001080814 FAT3 FAT tumor suppressor homolog 3 (Drosophila) adhesion NM_153795 FERMT3 fermitin family homolog 3 (Drosophila) adhesion NM_010494 ICAM2 intercellular adhesion molecule 2 adhesion NM_023892 ICAM4 (includes EG:3386) intercellular adhesion molecule 4 (Landsteiner-Wiener blood group)adhesion NM_001001979 MEGF10 multiple EGF-like-domains 10 adhesion NM_172522 MEGF11 multiple EGF-like-domains 11 adhesion NM_010739 MUC13 mucin 13, cell surface associated adhesion NM_013610 NINJ1 ninjurin 1 adhesion NM_016718 NINJ2 ninjurin 2 adhesion NM_172932 NLGN3 neuroligin -

1 Novel Expression Signatures Identified by Transcriptional Analysis
ARD Online First, published on October 7, 2009 as 10.1136/ard.2009.108043 Ann Rheum Dis: first published as 10.1136/ard.2009.108043 on 7 October 2009. Downloaded from Novel expression signatures identified by transcriptional analysis of separated leukocyte subsets in SLE and vasculitis 1Paul A Lyons, 1Eoin F McKinney, 1Tim F Rayner, 1Alexander Hatton, 1Hayley B Woffendin, 1Maria Koukoulaki, 2Thomas C Freeman, 1David RW Jayne, 1Afzal N Chaudhry, and 1Kenneth GC Smith. 1Cambridge Institute for Medical Research and Department of Medicine, Addenbrooke’s Hospital, Hills Road, Cambridge, CB2 0XY, UK 2Roslin Institute, University of Edinburgh, Roslin, Midlothian, EH25 9PS, UK Correspondence should be addressed to Dr Paul Lyons or Prof Kenneth Smith, Department of Medicine, Cambridge Institute for Medical Research, Addenbrooke’s Hospital, Hills Road, Cambridge, CB2 0XY, UK. Telephone: +44 1223 762642, Fax: +44 1223 762640, E-mail: [email protected] or [email protected] Key words: Gene expression, autoimmune disease, SLE, vasculitis Word count: 2,906 The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in Annals of the Rheumatic Diseases and any other BMJPGL products to exploit all subsidiary rights, as set out in their licence (http://ard.bmj.com/ifora/licence.pdf). http://ard.bmj.com/ on September 29, 2021 by guest. Protected copyright. 1 Copyright Article author (or their employer) 2009. -

Anti-GP1BA Polyclonal Antibody Cat:K007056P Summary
Anti-GP1BA Polyclonal Antibody Cat:K007056P Summary: 【Product name】: Anti-GP1BA antibody 【Source】: Rabbit 【Isotype】: IgG 【Species reactivity】: Human Mouse 【Swiss Prot】: P07359 【Gene ID】: 2811 【Calculated】: MW:72kDa 【Observed】: MW:72kDa 【Purification】: Affinity purification 【Tested applications】: WB IHC 【Recommended dilution】: WB 1:500-2000. IHC 1:10-100. 【WB Positive sample】: Rat liver,Jurkat,K-562 【IHC Positive sample】: Human lymphoma 【Subcellular location】: Cytoplasm 【Immunogen】: Recombinant protein of human GP1BA 【Storage】: Shipped at 4°C. Upon delivery aliquot and store at -20°C Background: Glycoprotein Ib (GP Ib) is a platelet surface membrane glycoprotein composed of a heterodimer, an alpha chain and a beta chain, that is linked by disulfide bonds. The Gp Ib functions as a receptor for von Willebrand factor (VWF). The complete receptor complex includes noncovalent association of the alpha and beta subunits with platelet glycoprotein IX and platelet glycoprotein V. The binding of the GP Ib-IX-V complex to VWF facilitates initial platelet adhesion to vascular subendothelium after vascular injury, and also initiates signaling events within the platelet that lead to enhanced platelet activation, thrombosis, and hemostasis. This gene encodes the alpha subunit. Mutations in this gene result in Bernard-Soulier syndromes and platelet-type von Willebrand disease. The coding region of this gene is known to contain a polymophic variable number tandem repeat (VNTR) domain that is associated with susceptibility to nonarteritic anterior ischemic optic neuropathy. Sales:[email protected] For research purposes only. Tech:[email protected] Please visit www.solarbio.com for a more product information Verified picture Western blot analysis with GP1BA antibody Immunohistochemistry of paraffin-embedded diluted at 1:1000; Lane: Rat liver, Human lymphoma with GP1BA antibody Jurkat,K-562 diluted at 1:30 Sales:[email protected] For research purposes only. -

Mouse CD Marker Chart Bdbiosciences.Com/Cdmarkers
BD Mouse CD Marker Chart bdbiosciences.com/cdmarkers 23-12400-01 CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD1d CD1.1, CD1.2, Ly-38 Lipid, Glycolipid Ag + + + + + + + + CD104 Integrin b4 Laminin, Plectin + DNAX accessory molecule 1 (DNAM-1), Platelet and T cell CD226 activation antigen 1 (PTA-1), T lineage-specific activation antigen 1 CD112, CD155, LFA-1 + + + + + – + – – CD2 LFA-2, Ly-37, Ly37 CD48, CD58, CD59, CD15 + + + + + CD105 Endoglin TGF-b + + antigen (TLiSA1) Mucin 1 (MUC1, MUC-1), DF3 antigen, H23 antigen, PUM, PEM, CD227 CD54, CD169, Selectins; Grb2, β-Catenin, GSK-3β CD3g CD3g, CD3 g chain, T3g TCR complex + CD106 VCAM-1 VLA-4 + + EMA, Tumor-associated mucin, Episialin + + + + + + Melanotransferrin (MT, MTF1), p97 Melanoma antigen CD3d CD3d, CD3 d chain, T3d TCR complex + CD107a LAMP-1 Collagen, Laminin, Fibronectin + + + CD228 Iron, Plasminogen, pro-UPA (p97, MAP97), Mfi2, gp95 + + CD3e CD3e, CD3 e chain, CD3, T3e TCR complex + + CD107b LAMP-2, LGP-96, LAMP-B + + Lymphocyte antigen 9 (Ly9), -

Cd42b (GP1BA) Rabbit Polyclonal Antibody – TA350034 | Origene
OriGene Technologies, Inc. 9620 Medical Center Drive, Ste 200 Rockville, MD 20850, US Phone: +1-888-267-4436 [email protected] EU: [email protected] CN: [email protected] Product datasheet for TA350034 CD42b (GP1BA) Rabbit Polyclonal Antibody Product data: Product Type: Primary Antibodies Applications: IHC, WB Recommended Dilution: ELISA: 2000-10000, WB: 500-2000, IHC: 100-300 Reactivity: Human, Mouse Host: Rabbit Isotype: IgG Clonality: Polyclonal Immunogen: Fusion protein of human GP1BA Formulation: pH7.4 PBS, 0.05% NaN3, 40% Glyceroln Concentration: lot specific Purification: Antigen affinity purification Conjugation: Unconjugated Storage: Store at -20°C as received. Stability: Stable for 12 months from date of receipt. Predicted Protein Size: 72 kDa Gene Name: glycoprotein Ib platelet alpha subunit Database Link: NP_000164 Entrez Gene 14723 MouseEntrez Gene 2811 Human P07359 This product is to be used for laboratory only. Not for diagnostic or therapeutic use. View online » ©2021 OriGene Technologies, Inc., 9620 Medical Center Drive, Ste 200, Rockville, MD 20850, US 1 / 3 CD42b (GP1BA) Rabbit Polyclonal Antibody – TA350034 Background: Glycoprotein Ib (GP Ib) is a platelet surface membrane glycoprotein composed of a heterodimer, an alpha chain and a beta chain, that is linked by disulfide bonds. The Gp Ib functions as a receptor for von Willebrand factor (VWF). The complete receptor complex includes noncovalent association of the alpha and beta subunits with platelet glycoprotein IX and platelet glycoprotein V. The binding of the GP Ib-IX-V complex to VWF facilitates initial platelet adhesion to vascular subendothelium after vascular injury, and also initiates signaling events within the platelet that lead to enhanced platelet activation, thrombosis, and hemostasis. -
![Anti-Cd42a Antibody [FMC-25] (PE) (ARG23073)](https://docslib.b-cdn.net/cover/8363/anti-cd42a-antibody-fmc-25-pe-arg23073-3198363.webp)
Anti-Cd42a Antibody [FMC-25] (PE) (ARG23073)
Product datasheet [email protected] ARG23073 Package: 50 tests anti-CD42a antibody [FMC-25] (PE) Store at: 4°C Summary Product Description PE-conjugated Mouse Monoclonal antibody [FMC-25] recognizes CD42a Mouse anti Human CD42a antibody, clone FMC-25 recognizes human CD42a, also known as Platelet glycoprotein IX, Glycoprotein 9 or GP-IX. CD42a is a 177 amino acid, ~20kDa type I single pass transmembrane glycoprotein containing a single leucine-rich repeat containing N-terminal domain and a single leucine-rich repeat containing C-terminal domain.CD42a is expressed by platelets and megakaryocytes and forms a covalent complex with CD42c (GP-1b-beta), CD42b (GP-1b-alpha) and CD42d (platelet glycoprotein V) to create the platelet surface receptor for von Willebrand factor. Incubation of the intact von Willebrand receptor complex with clone FMC-25 does not appear to inhibit binding of von Willebrand factor to the receptor (Yan et al. 2011). Defects in the GP1BB gene encoding human CD42a can lead to the inherited bleeding disorder Bernard-Soulier syndrome (Diz-Küçükkaya 2013), characterized by prolonged bleeding times, thrombocytopenia and the appearence of giant platelets in the circulation (Johns et al. 2014).Mouse anti human CD42a antibody, clone FMC-25 has been successfully used as a capture reagent for platelet-autoantibody complexes in the sera of patients presenting thrombocytopenia associated with anti-phospholipid syndrome (Godeau et al. 1997). Tested Reactivity Hu Tested Application FACS Host Mouse Clonality Monoclonal Clone FMC-25 Isotype IgG1 Target Name CD42a Antigen Species Human Immunogen Peripheral blood mononuclear cells. Conjugation PE Alternate Names Glycoprotein 9; CD antigen CD42a; CD42a; GPIX; GP-IX; Platelet glycoprotein IX Application Instructions Application table Application Dilution FACS Assay-dependent Application Note FACS: Use 10 µl of the suggested working dilution to label 10^6 cells in 100 µl. -

A Transition at Nucleotide 2110 in the Human Platelet Glycoprotein (Gp) Ix Gene Resulting in Ala139(Acc)~ Thr(Gcc) Substitution
Jpn J Human Genet 42, 369-371, 1997 Mutation Report G~A TRANSITION AT NUCLEOTIDE 2110 IN THE HUMAN PLATELET GLYCOPROTEIN (GP) IX GENE RESULTING IN ALA139(ACC)~ THR(GCC) SUBSTITUTION Tomohiro HAYASHI, I'* Keijiroh SUZUKI,1 Jiroh AKIBA, I Akito YAHAGI,x Katsushi TAJIMA, l Shinji SATOH,z and Hideo SASAKI1 1 Third Department of Internal Medicine and 2 Division of Blood Transfusion, Yamagata University School of Medicine, 2-2-2 lida-Nishi, Yamagata 990-23, Japan Key Words platelet glycoprotein IX, platelet membrane receptor, polymorphism, BstEII The glycoprotein (GP) IX is a platelet membrane-associated protein and forms an I : I non-covalent complex with GP Ib, a heterodimeric transmembrane protein consisting of a disulfide linked 140 kD a chain and 22 kD ,8 chain (Roth, 1991). This GPIb/IX complex serves as a receptor for plasma von Willebrand factor (vWF) to mediate platetet adhesion to the damaged vascular wall (Lopez, 1994). The GPIbot'chain provides the vWF binding site, but the individual contribution of GPIX to adherence is unclear. GPIX is a relatively small (Mr 20,000) surface protein, and employed in the efficient membrane expression of a functional GPIb/IX complex (Lopez et al., 1992). The gene of GPIX has been cloned and mapped to chromosome 3 (Hickey et al., 1990; Hickey and Roth, 1993). Genetic analyses of the patients with Bernard-Soulier syndrome (BSS), a hereditary qualitative platelet disorder characterized by a quantitative and/or qualitative abnormality of the GPIb/IX complex, revealed that the abnormality of the GPIX gene was able to cause BSS (Wright et al, 1993; Clemetson et al., 1994). -
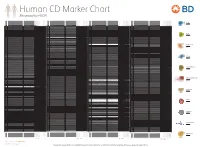
Reviewed by HLDA1
Human CD Marker Chart Reviewed by HLDA1 T Cell Key Markers CD3 CD4 CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD Alternative Name Ligands & Associated Molecules T Cell B Cell Dendritic Cell NK Cell Stem Cell/Precursor Macrophage/Monocyte Granulocyte Platelet Erythrocyte Endothelial Cell Epithelial Cell CD8 CD1a R4, T6, Leu6, HTA1 b-2-Microglobulin, CD74 + + + – + – – – CD74 DHLAG, HLADG, Ia-g, li, invariant chain HLA-DR, CD44 + + + + + + CD158g KIR2DS5 + + CD248 TEM1, Endosialin, CD164L1, MGC119478, MGC119479 Collagen I/IV Fibronectin + ST6GAL1, MGC48859, SIAT1, ST6GALL, ST6N, ST6 b-Galactosamide a-2,6-sialyl- CD1b R1, T6m Leu6 b-2-Microglobulin + + + – + – – – CD75 CD22 CD158h KIR2DS1, p50.1 HLA-C + + CD249 APA, gp160, EAP, ENPEP + + tranferase, Sialo-masked lactosamine, Carbohydrate of a2,6 sialyltransferase + – – + – – + – – CD1c M241, R7, T6, Leu6, BDCA1 b-2-Microglobulin + + + – + – – – CD75S a2,6 Sialylated lactosamine CD22 (proposed) + + – – + + – + + + CD158i KIR2DS4, p50.3 HLA-C + – + CD252 TNFSF4,