The Occasional Greater Occipital Nerve Block
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vertebral Column and Thorax
Introduction to Human Osteology Chapter 4: Vertebral Column and Thorax Roberta Hall Kenneth Beals Holm Neumann Georg Neumann Gwyn Madden Revised in 1978, 1984, and 2008 The Vertebral Column and Thorax Sternum Manubrium – bone that is trapezoidal in shape, makes up the superior aspect of the sternum. Jugular notch – concave notches on either side of the superior aspect of the manubrium, for articulation with the clavicles. Corpus or body – flat, rectangular bone making up the major portion of the sternum. The lateral aspects contain the notches for the true ribs, called the costal notches. Xiphoid process – variably shaped bone found at the inferior aspect of the corpus. Process may fuse late in life to the corpus. Clavicle Sternal end – rounded end, articulates with manubrium. Acromial end – flat end, articulates with scapula. Conoid tuberosity – muscle attachment located on the inferior aspect of the shaft, pointing posteriorly. Ribs Scapulae Head Ventral surface Neck Dorsal surface Tubercle Spine Shaft Coracoid process Costal groove Acromion Glenoid fossa Axillary margin Medial angle Vertebral margin Manubrium. Left anterior aspect, right posterior aspect. Sternum and Xyphoid Process. Left anterior aspect, right posterior aspect. Clavicle. Left side. Top superior and bottom inferior. First Rib. Left superior and right inferior. Second Rib. Left inferior and right superior. Typical Rib. Left inferior and right superior. Eleventh Rib. Left posterior view and left superior view. Twelfth Rib. Top shows anterior view and bottom shows posterior view. Scapula. Left side. Top anterior and bottom posterior. Scapula. Top lateral and bottom superior. Clavicle Sternum Scapula Ribs Vertebrae Body - Development of the vertebrae can be used in aging of individuals. -

Comparing the Injectate Spread and Nerve
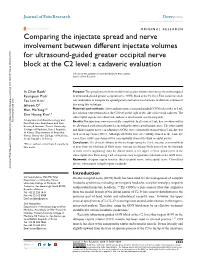
Journal name: Journal of Pain Research Article Designation: Original Research Year: 2018 Volume: 11 Journal of Pain Research Dovepress Running head verso: Baek et al Running head recto: Ultrasound-guided GON block open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S17269 Open Access Full Text Article ORIGINAL RESEARCH Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation In Chan Baek1 Purpose: The spread patterns between different injectate volumes have not yet been investigated Kyungeun Park1 in ultrasound-guided greater occipital nerve (GON) block at the C2 level. This cadaveric study Tae Lim Kim1 was undertaken to compare the spread pattern and nerve involvements of different volumes of Jehoon O2 dye using this technique. Hun-Mu Yang2,* Materials and methods: After randomization, ultrasound-guided GON blocks with 1 or 5 mL dye solution were performed at the C2 level on the right or left side of five fresh cadavers. The Shin Hyung Kim1,* suboccipital regions were dissected, and nerve involvement was investigated. 1 Department of Anesthesiology and Results: Ten injections were successfully completed. In all cases of 5 mL dye, we observed the Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University deeply stained posterior neck muscles, including the suboccipital triangle space. The suboccipital College of Medicine, Seoul, Republic and third occipital nerves, in addition to GONs, were consistently stained when 5-mL dye was 2 of Korea; Department of Anatomy, used in all injections (100%). Although all GONs were successfully stained in the 1-mL dye Yonsei University College of Medicine, Seoul, Republic of Korea cases, three of five injections (60%) concomitantly stained the third occipital nerves. -

Shoulder Anatomy & Clinical Exam
MSK Ultrasound - Spine - Incheon Terminal Orthopedic Private Clinic Yong-Hyun, Yoon C,T-spine Basic Advanced • Medial branch block • C-spine transforaminal block • Facet joint block • Thoracic paravertebral block • C-spine intra-discal injection • Superficial cervical plexus block • Vagus nerve block • Greater occipital nerve block(GON) • Third occipital nerve block(TON) • Hydrodissection • Brachial plexus(1st rib level) • Suboccipital nerve • Stellate ganglion block(SGB) • C1, C2 nerve root, C2 nerve • Brachial plexus block(interscalene) • Recurrent laryngeal nerve • Serratus anterior plane • Cervical nerve root Cervical facet joint Anatomy Diagnosis Cervical facet joint injection C-arm Ultrasound Cervical medial branch Anatomy Nerve innervation • Medial branch • Same level facet joint • Inferior level facet joint • Facet joint • Dual nerve innervation Cervical medial branch C-arm Ultrasound Cervical nerve root Anatomy Diagnosis • Motor • Sensory • Dermatome, myotome, fasciatome Cervical nerve root block C-arm Ultrasound Stallete ganglion block Anatomy Injection Vagus nerve Anatomy Injection L,S-spine Basic Advanced • Medial branch block • Lumbar sympathetic block • Facet joint block • Lumbar plexus block • Superior, inferior hypogastric nerve block • Caudal block • Transverse abdominal plane(TAP) block • Sacral plexus block • Epidural block • Hydrodissection • Interlaminal • Pudendal nerve • Transforaminal injection • Genitofemoral nerve • Superior, inferior cluneal nerve • Rectus abdominal sheath • Erector spinae plane Lumbar facet -

Anatomy of the Spine
12 Anatomy of the Spine Overview The spine is made of 33 individual bones stacked one on top of the other. Ligaments and muscles connect the bones together and keep them aligned. The spinal column provides the main support for your body, allowing you to stand upright, bend, and twist. Protected deep inside the bones, the spinal cord connects your body to the brain, allowing movement of your arms and legs. Strong muscles and bones, flexible tendons and ligaments, and sensitive nerves contribute to a healthy spine. Keeping your spine healthy is vital if you want to live an active life without back pain. Spinal curves When viewed from the side, an adult spine has a natural S-shaped curve. The neck (cervical) and low back (lumbar) regions have a slight concave curve, and the thoracic and sacral regions have a gentle convex curve (Fig. 1). The curves work like a coiled spring to absorb shock, maintain balance, and allow range of motion throughout the spinal column. The muscles and correct posture maintain the natural spinal curves. Good posture involves training your body to stand, walk, sit, and lie so that the least amount of strain is placed on the spine during movement or weight-bearing activities. Excess body weight, weak muscles, and other forces can pull at the spine’s alignment: • An abnormal curve of the lumbar spine is lordosis, also called sway back. • An abnormal curve of the thoracic spine is Figure 1. (left) The spine has three natural curves that form kyphosis, also called hunchback. an S-shape; strong muscles keep our spine in alignment. -

Occipital Neuralgia: a Literature Review of Current Treatments from Traditional Medicine to CAM Treatments
Occipital Neuralgia: A Literature Review of Current Treatments from Traditional Medicine to CAM Treatments By Nikole Benavides Faculty Advisor: Dr. Patrick Montgomery Graduation: April 2011 1 Abstract Objective. This article provides an overview of the current and upcoming treatments for people who suffer from the signs and symptoms of greater occipital neuralgia. Types of treatments will be analyzed and discussed, varying from traditional Western medicine to treatments from complementary and alternative health care. Methods. A PubMed search was performed using the key words listed in this abstract. Results. Twenty-nine references were used in this literature review. The current literature reveals abundant peer reviewed research on medications used to treat this malady, but relatively little on the CAM approach. Conclusion. Occipital Neuralgia has become one of the more complicated headaches to diagnose. The symptoms often mimic those of other headaches and can occur post-trauma or due to other contributing factors. There are a variety of treatments that involve surgery or blocking of the greater occipital nerve. As people continue to seek more natural treatments, the need for alternative treatments is on the rise. Key Words. Occipital Neuralgia; Headache; Alternative Treatments; Acupuncture; Chiropractic; Nutrition 2 Introduction Occipital neuralgia is a type of headache that describes the irritation of the greater occipital nerve and the signs and symptoms associated with it. It is a difficult headache to diagnose due to the variety of signs and symptoms it presents with. It can be due to a post-traumatic event, degenerative changes, congenital anomalies, or other factors (10). The patterns of occipital neuralgia mimic those of other headaches. -

Vertebral Column
Vertebral Column • Backbone consists of Cervical 26 vertebrae. • Five vertebral regions – Cervical vertebrae (7) Thoracic in the neck. – Thoracic vertebrae (12) in the thorax. – Lumbar vertebrae (5) in the lower back. Lumbar – Sacrum (5, fused). – Coccyx (4, fused). Sacrum Coccyx Scoliosis Lordosis Kyphosis Atlas (C1) Posterior tubercle Vertebral foramen Tubercle for transverse ligament Superior articular facet Transverse Transverse process foramen Facet for dens Anterior tubercle • Atlas- ring of bone, superior facets for occipital condyles. – Nodding movement signifies “yes”. Axis (C2) Spinous process Lamina Vertebral foramen Transverse foramen Transverse process Superior articular facet Odontoid process (dens) •Axis- dens or odontoid process is body of atlas. – Pivotal movement signifies “no”. Typical Cervical Vertebra (C3-C7) • Smaller bodies • Larger spinal canal • Transverse processes –Shorter – Transverse foramen for vertebral artery • Spinous processes of C2 to C6 often bifid • 1st and 2nd cervical vertebrae are unique – Atlas & axis Typical Cervical Vertebra Spinous process (bifid) Lamina Vertebral foramen Inferior articular process Superior articular process Transverse foramen Pedicle Transverse process Body Thoracic Vertebrae (T1-T12) • Larger and stronger bodies • Longer transverse & spinous processes • Demifacets on body for head of rib • Facets on transverse processes (T1-T10) for tubercle of rib Thoracic Vertebra- superior view Spinous process Transverse process Facet for tubercle of rib Lamina Superior articular process -

Cervical Vertebrae 1 Cervical Vertebrae
Cervical vertebrae 1 Cervical vertebrae Cervical vertebrae or Cervilar Position of human cervical vertebrae (shown in red). It consists of 7 bones, from top to bottom, C1, C2, C3, C4, C5, C6 and C7. A human cervical vertebra Latin Vertebrae cervicales [1] Gray's p.97 [2] MeSH Cervical+vertebrae [3] TA A02.2.02.001 [4] FMA FMA:72063 In vertebrates, cervical vertebrae (singular: vertebra) are those vertebrae immediately inferior to the skull. Thoracic vertebrae in all mammalian species are defined as those vertebrae that also carry a pair of ribs, and lie caudal to the cervical vertebrae. Further caudally follow the lumbar vertebrae, which also belong to the trunk, but do not carry ribs. In reptiles, all trunk vertebrae carry ribs and are called dorsal vertebrae. In many species, though not in mammals, the cervical vertebrae bear ribs. In many other groups, such as lizards and saurischian dinosaurs, the cervical ribs are large; in birds, they are small and completely fused to the vertebrae. The transverse processes of mammals are homologous to the cervical ribs of other amniotes. Cervical vertebrae 2 In humans, cervical vertebrae are the smallest of the true vertebrae, and can be readily distinguished from those of the thoracic or lumbar regions by the presence of a foramen (hole) in each transverse process, through which passes the vertebral artery. The remainder of this article focuses upon human anatomy. Structure By convention, the cervical vertebrae are numbered, with the first one (C1) located closest to the skull and higher numbered vertebrae (C2-C7) proceeding away from the skull and down the spine. -
Comparing the Injectate Spread and Nerve
Journal name: Journal of Pain Research Article Designation: Original Research Year: 2018 Volume: 11 Journal of Pain Research Dovepress Running head verso: Baek et al Running head recto: Ultrasound-guided GON block open access to scientific and medical research DOI: http://dx.doi.org/10.2147/JPR.S17269 Open Access Full Text Article ORIGINAL RESEARCH Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation In Chan Baek1 Purpose: The spread patterns between different injectate volumes have not yet been investigated Kyungeun Park1 in ultrasound-guided greater occipital nerve (GON) block at the C2 level. This cadaveric study Tae Lim Kim1 was undertaken to compare the spread pattern and nerve involvements of different volumes of Jehoon O2 dye using this technique. Hun-Mu Yang2,* Materials and methods: After randomization, ultrasound-guided GON blocks with 1 or 5 mL dye solution were performed at the C2 level on the right or left side of five fresh cadavers. The Shin Hyung Kim1,* suboccipital regions were dissected, and nerve involvement was investigated. 1Department of Anesthesiology and For personal use only. Results: Ten injections were successfully completed. In all cases of 5 mL dye, we observed the Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University deeply stained posterior neck muscles, including the suboccipital triangle space. The suboccipital College of Medicine, Seoul, Republic and third occipital nerves, in addition to GONs, were consistently stained when 5-mL dye was 2 of Korea; Department of Anatomy, used in all injections (100%). -

SŁOWNIK ANATOMICZNY (ANGIELSKO–Łacinsłownik Anatomiczny (Angielsko-Łacińsko-Polski)´ SKO–POLSKI)
ANATOMY WORDS (ENGLISH–LATIN–POLISH) SŁOWNIK ANATOMICZNY (ANGIELSKO–ŁACINSłownik anatomiczny (angielsko-łacińsko-polski)´ SKO–POLSKI) English – Je˛zyk angielski Latin – Łacina Polish – Je˛zyk polski Arteries – Te˛tnice accessory obturator artery arteria obturatoria accessoria tętnica zasłonowa dodatkowa acetabular branch ramus acetabularis gałąź panewkowa anterior basal segmental artery arteria segmentalis basalis anterior pulmonis tętnica segmentowa podstawna przednia (dextri et sinistri) płuca (prawego i lewego) anterior cecal artery arteria caecalis anterior tętnica kątnicza przednia anterior cerebral artery arteria cerebri anterior tętnica przednia mózgu anterior choroidal artery arteria choroidea anterior tętnica naczyniówkowa przednia anterior ciliary arteries arteriae ciliares anteriores tętnice rzęskowe przednie anterior circumflex humeral artery arteria circumflexa humeri anterior tętnica okalająca ramię przednia anterior communicating artery arteria communicans anterior tętnica łącząca przednia anterior conjunctival artery arteria conjunctivalis anterior tętnica spojówkowa przednia anterior ethmoidal artery arteria ethmoidalis anterior tętnica sitowa przednia anterior inferior cerebellar artery arteria anterior inferior cerebelli tętnica dolna przednia móżdżku anterior interosseous artery arteria interossea anterior tętnica międzykostna przednia anterior labial branches of deep external rami labiales anteriores arteriae pudendae gałęzie wargowe przednie tętnicy sromowej pudendal artery externae profundae zewnętrznej głębokiej -
Bones of the Trunk
BONES OF THE TRUNK Andrea Heinzlmann Veterinary University Department of Anatomy and Histology 16th September 2019 VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) • the vertebral column composed of the vertebrae • the vertebrae form a horizontal chain https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) along the vertebral column three major curvatures are recognized: 1. the DORSAL CONVEX CURVATURE – between the head and the neck 2. the DORSAL CONCAVE CURVATURE – between the neck and the chest 3. the DORSAL CONVEX CURVATURE – between the thorax and the lumbar region - in carnivores (Ca) there is an additional DORSAL CONVEXITY in the sacral region https://hu.pinterest.com/pin/159877855502035893/ VERTEBRAL COLUMN (COLUMNA VERTEBRALIS) - corresponding to the regions of the body, we distinguish: 1. CERVICAL VERTEBRAE 2. THORACIC VERTEBRAE 3. LUMBAR VERTEBRAE 4. SACRAL VERTEBRAE 5. CAUDAL (COCCYGEAL) VERTEBRAE https://www.ufaw.org.uk/dogs/french-bulldog-hemivertebrae https://rogueshock.com/know-your-horse-in-9-ways/5/ BUILD OF THE VERTEBRAE each vertebrae presents: 1. BODY (CORPUS VERTEBRAE) 2. ARCH (ARCUS VERTEBRAE) 3. PROCESSES corpus Vertebra thoracica (Th13) , Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) - the ventral portion of the vertebra ITS PARTS: 1. EXTREMITAS CRANIALIS (seu CAPUT VERTEBRAE) – convex 2. EXTREMITAS CAUDALIS (seu FOSSA VERTEBRAE) - concave Th13, Ca. THE VERTEBRAL BODY (CORPUS VERTEBRAE) 3. VENTRAL SURFACE of the body has a: - ventral crest (CRISTA VENTRALIS) 4. DORSAL SURFACE of the body carries : - the vertebral arch (ARCUS VERTEBRAE) Th13, Ca., lateral aspect Arcus vertebrae corpus Vertebra thoracica (Th13) , Ca., caudal aspect THE VERTEBRAL BODY (CORPUS VERTEBRAE) 6. VERTEBRAL ARCH (ARCUS VERTEBRAE) compraisis: a) a ventral PEDICULUS ARCUS VERTEBRAE b) a dorsal LAMINA ARCUS VERTEBRAE C7, Ca. -

Redalyc.Headaches and Pain Referred to the Teeth: Frequency And
RSBO Revista Sul-Brasileira de Odontologia ISSN: 1806-7727 [email protected] Universidade da Região de Joinville Brasil Franklin Molina, Omar; Huber Simião, Bruno Ricardo; Yukio Hassumi, Marcio; Iuata Rank, Rise Consolação; da Silva Junior, Fausto Félix; Alves de Carvalho, Adilson Headaches and pain referred to the teeth: frequency and potential neurophysiologic mechanisms RSBO Revista Sul-Brasileira de Odontologia, vol. 12, núm. 2, abril-junio, 2015, pp. 151- 159 Universidade da Região de Joinville Joinville, Brasil Available in: http://www.redalyc.org/articulo.oa?id=153041505002 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative ISSN: Electronic version: 1984-5685 RSBO. 2015 Apr-Jun;12(2):151-9 Original Research Article Headaches and pain referred to the teeth: frequency and potential neurophysiologic mechanisms Omar Franklin Molina1 Bruno Ricardo Huber Simião2 Marcio Yukio Hassumi3 Rise Consolação Iuata Rank4 Fausto Félix da Silva Junior5 Adilson Alves de Carvalho6 Corresponding author: Omar Franklin Molina Avenida Pará, 1.544 – Faculdade de Odontologia CEP 77400-000 – Gurupi – TO – Brasil E-mail: [email protected] 1 School of Dentistry (Orofacial Pain), UNIRG University Center – Gurupi – TO – Brazil. 2 School of Dentistry (Prosthodontics), UNIRG University Center – Gurupi – TO – Brazil. 3 School of Dentistry (Periodontics), UNIRG University Center – Gurupi – TO – Brazil. 4 School of Dentistry (Pedodontics), UNIRG University Center – Gurupi – TO – Brazil 5 School of Dentistry (Preventive Dentistry), UNIRG University Center – Gurupi – TO – Brazil 6 Private Practice – Goiânia – GO – Brazil. -

Anatomy of the Spine
Anatomy of the Spine Musculoskeletal block- Anatomy-lecture 4 Editing file Color guide : Objectives Only in boys slides in Blue Only in girls slides in Purple By the end of this lecture you should be able to: important in Red Doctor note in Green ✓ Distinguish and describe the cervical, thoracic, lumbar, sacral and Extra information in Grey coccygeal vertebrae. ✓ Describe the vertebral curvatures. ✓ Describe the movement which occur in each region of the vertebral column. ✓ List the structures which connect 2 adjacent vertebrae together. ✓ List and identify the ligaments of the intervertebral joints. Spine or Vertebral Column ● The vertebral column extends from the skull to the pelvis. ● It surrounds and protects the spinal cord and supports the whole body. ● It is formed from 33 irregular vertebrae. It consists of 24 single vertebrae and 2 bones: •Sacrum, (5 fused vertebrae).(Convex) •Coccyx, (4 fused vertebrae). Of the 24 single bones, •7 Cervical vertebrae (concave) •12 Thoracic vertebrae(convex) •5 Lumbar vertebrae.(concave) The single vertebrae are separated by pads of flexible fibrocartilage called the intervertebral disc. • The intervertebral discs cushion the vertebrae and absorb shocks. • The spinal curvature and discs make the body trunk flexible and prevent shock to head while walking or running. • We have 2 spinal curvatures: 1) Primary curvature (present at birth): Concave forward - Thoracic - Sacral regions 2) Secondary curvature (present after birth): Convex forward - Cervical (after the baby holds his head 6th month) - Lumbar (after walking around one year) 3 Typical Vertebra ● Any vertebra is made up of: 1) Body or Centrum: - disc-like weight bearing part that lies anteriorly 2) Vertebral Arch: - Formed from fusion of 2 pedicles and 2 laminae ● Vertebral foramen lies between the body and the vertebral foramen.