Immunization Coverage Evaluation in a Rural Block of Haryana, India Dr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Facility Wise Deployment of Contractual Staff Engaged Under NRHM Name of District: Rohtak Name of Date of Joining on Sr.No
Facility Wise Deployment of contractual Staff engaged under NRHM Name of District: Rohtak Name of Date of Joining on Sr.No. Name of contractual Designation Name of Facility Contact No. Programme contract 1 Yogender Siwach Secretarial Assistant RCH-II DH&FW Society 09 January 2006 9812508080 2 Deepak Kumar DPM RCH-II DH&FW Society 09 November 2009 9034029200 3 Manjeet Singh Accounts Assistant RCH-II CHC Sampla 09 January 2006 9416944534 4 Sarita Lab Technician RCH-II GH Rohtak 27 August 2003 9466306067 Accounts Assistant Upender RCH-II DH&FW Society 9812503192 5 (Additional) 26 August 2009 Central Store O/o Civil Sunil Computer Operator P&L RCH-II 9315454742 6 Surgeon Rohtak 28 August 2009 Central Store O/o Civil Parmvir Hooda Computer Operator RCH-II 9416472739 7 Surgeon Rohtak 24 August 2009 8 Ajay Dhingra Accounts Manager RCH-II DH&FW Society 24 January 1900 9896004141 Central Store O/o Civil Joginder Singh Pharmacist P&L RCH-II 9466794683 9 Surgeon Rohtak 24 August 2009 10 Neeru Computer Assistant RCH-II DTO Rohtak 26 February 2009 9729471886 11 Vikram Accounts Assistant RCH-II CHC Kalanaur 17 November 2008 9812281600 12 Mohammad Shahid Urdu Reader RCH-II Birth/Death Branch 17 November 2008 9467070729 13 Anil Accounts Assistant RCH-II DH&FW Society 17 November 2008 9992349003 Jyoti Information Assistant RCH-II PHC Lakhan Majra 9467222480 14 28 August 2009 Sapna rani Accounts Clerk-cum DEO RCH-II DTO Rohtak 9255168124 17 21 July 2009 Narender Information Assistant RCH-II PHC Pilana 9355621986 18 21 July 2009 Salochana Information Assistant -

Statistical Abstract Haryana 2007-08.Pdf
„UÁ⁄UÿÊáÊÊ ‚⁄U∑§Ê⁄U GOVERNMENT OF HARYANA ¬˝∑§Ê‡ÊŸ ∑˝§◊Ê¢∑§ ~vÆ PUBLICATION NO. 910 ‚Ê¢ÁÅÿ∑§Ëÿ ‚Ê⁄UÊ¢‡Ê „UÁ⁄UÿÊáÊÊ 2007-08 STATISTICAL ABSTRACT HARYANA 2007-08 ISSUED BY : DEPARTMENT OF ECONOMIC AND STATISTICAL ANALYSIS, HARYANA 2009 ÉkbPk^kTkk U„UÁ⁄UÿÊáÊÊ ∑§Ê flø◊ÊŸ ‚Ê¢ÁÅÿ∑§Ëÿ ‚Ê⁄UÊ¢‡Ê wÆÆ|-Æ} •Õ¸ ÃÕÊ ‚Ê¢ÁÅÿ∑§Ëÿ Áfl‡‹·áÊ Áfl÷ʪ ∑§Ê flÊÁ·¸∑§ ¬˝∑§Ê‡ÊŸ „ÒU Á¡‚◊¥ ⁄UÊÖÿ ∑§Ë •Õ¸√ÿflSÕÊ ∑§ ‹ª÷ª ‚÷Ë ‚Ê◊ÊÁ¡∑§ ÃÕÊ •ÊÁÕ¸∑§ ¬„U‹È•Ù¥ ¬⁄U √ÿʬ∑§ ÃÕÊ ŸflËŸÃ◊ •Ê¢∑§«∏U ÁŒÿ ªÿ „Ò¥U– ÿ„U ¬˝ÁÃÔfl·¸ ÁflœÊŸ‚÷Ê ∑§ ◊ÊŸŸËÿ ‚ŒSÿÙ¥ ∑§Ù •ãÿ ’¡≈U ŒSÃÊfl¡Ù¥ ‚Á„Uà ¬˝SÃÈà Á∑§ÿÊ ¡ÊÃÊ „ÒU– Áfl÷ʪ mÊ⁄UÊ ß‚ ¬˝∑§Ê‡ÊŸ ◊¥ ¬Á⁄UflÁøà •ÊÁÕ¸∑§ ¬Á⁄UÁSÕÁÃÿÙ¥ ∑§Ë ’…∏UÃË „ÈU߸ ◊Ê¢ª ∑§Ù ¬Í⁄UÊ ∑§⁄UŸ ∑§ Á‹∞ •Áœ∑§ ‚ •Áœ∑§ ‚ÍøŸÊ ‚Áê◊Á‹Ã ∑§⁄UŸ ∑§ ¬˝ÿÊ‚ Á∑§∞ ª∞ „Ò¥U– ◊È¤Ê •Ê‡ÊÊ „ÒU Á∑§ ß‚ ¬ÈSÃ∑§ ◊¥ ‚Áê◊Á‹Ã ‚ÍøŸÊ Ÿ ∑§fl‹ ⁄UÊÖÿ ∑§ ÁflÁ÷㟠ˇÊòÊÙ¥ ∑§Ë ¬˝ªÁà ∑§ ÁŸœÊ¸⁄UáÊ „UÃÈ ©U¬ÿÙªË Á‚h „UÙªË •Á¬ÃÈ ÷Áflcÿ ◊¥ ÁflÁ÷㟠Áfl∑§Ê‚ ÿÙ¡ŸÊ•Ù¥ ∑§ ÁŸM§¬áÊ ÃÕÊ ŸËÁà ÁŸœÊ¸⁄UáÊ „UÃÈ •ÊœÊ⁄U÷Íà •Ê¢∑§«∏UÙ¥ ∑§Ê ∑§Êÿ¸ ÷Ë ∑§⁄UªË– •Ã— ÿ„U ¬˝∑§Ê‡ÊŸ ÿÙ¡ŸÊ∑§Ê⁄UÙ¥, ¬˝‡ÊÊ‚∑§Ù¥, ÁflœÊÿ∑§Ù¥, ÁflûÊËÿ ‚¢SÕÊ•Ù¥ ÃÕÊ ÁflÁ÷㟠•ŸÈ‚¢œÊŸ ‚¢SÕÊŸÙ¥ Á¡ã„¥U ⁄UÊÖÿ ∑§Ë •Õ¸-√ÿflSÕÊ ◊¥ L§Áø „ÒU, ∑§ Á‹ÿ ‹Ê÷ŒÊÿ∑§ „U٪ʖ ÁflSÃÎà ¬˝ÿÙª „UÃÈ ß‚∑§Ù Áfl÷ʪ ∑§Ë flÒ’ ‚Ê߸≈U ¬⁄U ÁŒÿÊ ªÿÊ „ÒU ¡Ù Á∑§ www.esa.hry.gov.in ¬⁄U ŒπÊ ¡Ê ‚∑§ÃÊ „ÒU– ◊Ò¥ ÁŸŒ‡Ê∑§, •Õ¸ ÃÕÊ ‚Ê¢ÁÅÿ∑§Ëÿ Áfl‡‹·áÊ Áfl÷ʪU, „UÁ⁄UÿÊáÊÊ •ı⁄U ©UŸ∑§ S≈UÊ»§ Á¡ã„UÙ¥Ÿ ßß ’«∏U •Ê∑§Ê⁄U ∑§ ¬˝∑§Ê‡ÊŸ ◊¥ ÁflSÃÊ⁄U¬Ífl¸∑§ •Ê¢∑§«∏U ‚◊ÿ ¬⁄U ŒŸ ∑§ ¬˝ÿÊ‚ ∑§Ë ¬˝‡Ê¢‚Ê ∑§⁄UÃÊ „Í°U– ÁŒŸÊ¢∑§ øá«U˪…∏U — ’Ë⁄Uãº˝ Á‚¢„U vy ¡Ÿfl⁄UË, wÆÆ~ ÁflûÊ ∞fl¢ ÿÙ¡ŸÊ ◊¢òÊË, „UÁ⁄UÿÊáÊÊ– FOREWORD The present State Statistical Abstract of Haryana which contains the latest available data on almost all socio-economic aspects of the State economy, is an annual publication of Department of Economic & Statistical Analysis, Haryana. -
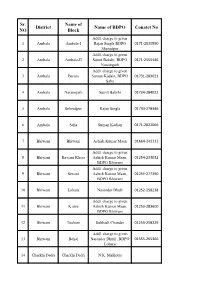
Sr. NO District Name of Block Name of BDPO Conatct No
Sr. Name of District Name of BDPO Conatct No NO Block Addl. charge to given 1 Ambala Ambala-I Rajan Singla BDPO 0171-2530550 Shazadpur Addl. charge to given 2 Ambala Ambala-II Sumit Bakshi, BDPO 0171-2555446 Naraingarh Addl. charge to given 3 Ambala Barara Suman Kadain, BDPO 01731-283021 Saha 4 Ambala Naraingarh Sumit Bakshi 01734-284022 5 Ambala Sehzadpur Rajan Singla 01734-278346 6 Ambala Saha Suman Kadian 0171-2822066 7 Bhiwani Bhiwani Ashish Kumar Maan 01664-242212 Addl. charge to given 8 Bhiwani Bawani Khera Ashish Kumar Maan, 01254-233032 BDPO Bhiwani Addl. charge to given 9 Bhiwani Siwani Ashish Kumar Maan, 01255-277390 BDPO Bhiwani 10 Bhiwani Loharu Narender Dhull 01252-258238 Addl. charge to given 11 Bhiwani K airu Ashish Kumar Maan, 01253-283600 BDPO Bhiwani 12 Bhiwani Tosham Subhash Chander 01253-258229 Addl. charge to given 13 Bhiwani Behal Narender Dhull , BDPO 01555-265366 Loharu 14 Charkhi Dadri Charkhi Dadri N.K. Malhotra Addl. charge to given 15 Charkhi Dadri Bond Narender Singh, BDPO 01252-220071 Charkhi Dadri Addl. charge to given 16 Charkhi Dadri Jhoju Ashok Kumar Chikara, 01250-220053 BDPO Badhra 17 Charkhi Dadri Badhra Jitender Kumar 01252-253295 18 Faridabad Faridabad Pardeep -I (ESM) 0129-4077237 19 Faridabad Ballabgarh Pooja Sharma 0129-2242244 Addl. charge to given 20 Faridabad Tigaon Pardeep-I, BDPO 9991188187/land line not av Faridabad Addl. charge to given 21 Faridabad Prithla Pooja Sharma, BDPO 01275-262386 Ballabgarh 22 Fatehabad Fatehabad Sombir 01667-220018 Addl. charge to given 23 Fatehabad Ratia Ravinder Kumar, BDPO 01697-250052 Bhuna 24 Fatehabad Tohana Narender Singh 01692-230064 Addl. -

Government of Haryana Department of Revenue & Disaster Management
Government of Haryana Department of Revenue & Disaster Management DISTRICT DISASTER MANAGEMENT PLAN SONIPAT 2020-21 Prepared & Updated By DISTRICT DISASTER MANAGEMENT AUTHORITY, Room no. 110, Mini Secretariat, Sonipat District Disaster Management Plan, Sonipat 2020-21 2 District Disaster Management Plan, Sonipat 2020-21 3 District Disaster Management Plan, Sonipat 2020-21 4 District Disaster Management Plan, Sonipat 2020-21 Contents Page No. 1 Introduction 16 1.1 General Information 16 1.2 Topography 16 1.3 Demography 16 1.4 Climate & Rainfall 17 1.5 Land Use Pattern 17 1.6 Agriculture and Cropping Pattern 17 1.7 Industries 18 1.8 Culture 18 1.9 Transport and Connectivity 18 2 Hazard Vulnerability & Capacity Analysis 20 2.1 Hazards Analysis 20 2.2 Hazards in Sonipat 20 2.2.1 Earthquake 20 2.2.2 Chemical Accidents 20 2.2.3 Fires 21 2.2.4 Accidents 22 2.2.5 Floods 22 2.2.6 Drought 23 2.2.7 Extreme Temperature 23 2.2.8 Epidemics 23 2.2.9 Other Hazards 24 2.3 Hazards Seasonality Map 24 2.4 Vulnerability Analysis 25 2.4.1 Physical Vulnerability 25 2.4.2 Structural vulnerability 25 2.4.3 Social Vulnerability 26 2.5 Capacity Analysis 28 2.6 Risk Analysis 30 3 Institutional Mechanism 32 3.1 Institutional Mechanisms at National Level 32 3.1.1 Disaster Management Act, 2005 32 3.1.2 Central Government 32 3.1.3 Cabinet Committee on Management of Natural Calamities 33 (CCMNC) and the Cabinet Committee on Security (CCS) 3.1.4 High Level Committee (HLC) 34 3.1.5 National Crisis Management Committee (NCMC) 34 3.1.6 National Disaster Management Authority -

Uttar Haryana Bijli Vitran Nigam(UHBVN)
UTTAR HARYANA BIJLI VITRAN NIGAM NOTICE INVITING TENDER No. 53/ P&D/ 2013 Sealed Tenders from the approved and experienced contractor/ firm are invited in two parts by CGM/ PD&C, UHBVN, Panchkula in duplicate on the prescribed proforma for augmentation of existing 33 kV Sub-stations as per details given below:- Sr. NIT No. Bid Brief Scope of work/ purchase Last date of submission No. No. of Bids (Date & Time) NIT No. B- 370 Augmentation of existing 21 Nos. 33 kV Last date of sale of tender 1. 53/ P&D/ Sub-stations (1) Jaitpura, (2) Jhajjar, documents 30.12.2013 2013 (3) Jahajgarh, (4) Balu, (5) Kheri upto 17:00 Hrs Ghulam Ali, (6) Cheeka, (7) Kurar, Last date of submission of (8) Mastgarh, (9) Manjura, (10) Kailmla, bids 31.12.2013 upto 13:00 (11) Garhi Birbal, (12) Ram Nagar NDRI Hrs (Karnal), (13) Ishaq, (14) Morthali, Date of opening of bids (15) Kirmich, (16) Sr. Sec. School 31.12.2013 at 15:00 Hrs Rohtak, (17) HCC Rohtak, (18) Bhalout, (19) Lakhan Majra, (21) Model Town Rohtak, (21) Kharawar) under ‘Op’ Circles Ambala, Jhajjar, Kaithal, Karnal, Kurukshetra & Rohtak. Detailed terms & conditions are available on the website i.e. www.uhbvn.com. - Sd - General Manager/ P&D, for Chief General Manager / PD&C, UHBVN, Panchkula. C:\Documents and Settings\uhbvn\Desktop\up\NIT_1P_B- 370.doc1 UTTAR HARYANA BIJLI VITRAN NIGAM NOTICE INVITING TENDER No. 53/ P&D/ 2013 Sealed tenders in two parts (Technical, Commercial & Financial qualification Criteria (Part-I) and Price Bid (Part-II), separately sealed) are invited by the Chief General Manager/ PD&C, UHBVN, Panchkula on behalf of Uttar Haryana Bijli Vitran Nigam Limited (UHBVNL), from the approved & experienced contractors / firms on the prescribed forms for augmentation of existing 33 kV Sub-stations on turnkey basis in geographical area of UHBVN, as detailed under:- NIT No. -

Meham Assembly Haryana Factbook
Editor & Director Dr. R.K. Thukral Research Editor Dr. Shafeeq Rahman Compiled, Researched and Published by Datanet India Pvt. Ltd. D-100, 1st Floor, Okhla Industrial Area, Phase-I, New Delhi- 110020. Ph.: 91-11- 43580781, 26810964-65-66 Email : [email protected] Website : www.electionsinindia.com Online Book Store : www.datanetindia-ebooks.com Report No. : AFB/HR-60-0118 ISBN : 978-93-5293-516-1 First Edition : January, 2018 Third Updated Edition : June, 2019 Price : Rs. 11500/- US$ 310 © Datanet India Pvt. Ltd. All rights reserved. No part of this book may be reproduced, stored in a retrieval system or transmitted in any form or by any means, mechanical photocopying, photographing, scanning, recording or otherwise without the prior written permission of the publisher. Please refer to Disclaimer at page no. 144 for the use of this publication. Printed in India No. Particulars Page No. Introduction 1 Assembly Constituency at a Glance | Features of Assembly as per 1-2 Delimitation Commission of India (2008) Location and Political Maps 2 Location Map | Boundaries of Assembly Constituency in District | Boundaries 3-9 of Assembly Constituency under Parliamentary Constituency | Town & Village-wise Winner Parties- 2014-PE, 2014-AE, 2009-PE and 2009-AE Administrative Setup 3 District | Sub-district | Towns | Villages | Inhabited Villages | Uninhabited 10-13 Villages | Village Panchayat | Intermediate Panchayat Demographics 4 Population | Households | Rural/Urban Population | Towns and Villages by 14-15 Population Size | Sex Ratio -
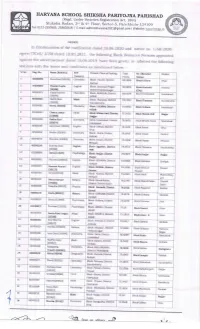
Re-Allocation Orders of Brps Appointed Vide
ORDER In Continuation of the notification clated 25.06.2020 ancl notice no. ll6g-2020- egove/lTCell/ 2350 dated 18'05.202I, the following Block Resource persons appointed against the aclvertisement datecl 15.06.2019 have been given/ re- allottecl the following stations with the terms ancl conditions as rrientioned below :- Sr no. Reg. No, Name No] [Roll BRP Present Place of Posting Total Re- Allocated District (Subiect) Po ints Station 1 80s00090 Renu Rani [50246] Chemistry Block Pundri, District 82.3904 Block Uklana Hisar Kaithal 2 90300003 Sheetal Gupta English Block Saraswati Nagar, 80.5491 Block Ambala-l Ambala [30388] District Yamunanagar (citv) 3 80500379 Vijeta Kumari Chemistry Block AGROHA, District 80.0159 Block Fatehabad Fate ha b ad [50287] HISAR 4 80200521 Kavita Devi Math Block Thanesar, District 19.7555 Block Thanesar Ku ru kshetra [20s0sl Kurukashetra 5 80500082 Neetu [50044] Chemistry Block UKLAN& District 79.0958 Block Tohana Fateha b ad HISAR 6 80100534 Chetna Jathol Hnd Block Matan Hail, District 17.2672 Block Matan Hail Jhajjar [10488] Jhajjar 7 80500239 Rekha Rani Chemistry Block Fatehabad, District 76.9072 Block Bhattu Kalan Fate hab ad Iso274l Fatehab ad 8 80300187 Aarti Devi [30042] Engl ish Block Odhan, Dlstrict 76.s692 Block Rania Sirsa Sirsa 9 80s00265 Shalini Is0294] Chemistry Block Guhla, District 76.O107 Block Siwan Kaithal Kaith al 10 80500243 Manisha [500891 Chemistry Block Siwani, District 75.3908 Block Siwani Bhiwani Bhiwani 11 80300199 Sushma Devi English Block Jagadhri, District t 5.3571 Elock Thanesar -

Village & Townwise Primary Census Abstract, Rohtak, Part XII-A & B
CENSUS OF INDIA 1991 SERIES-8 HARYANA DISTRICT CENSUS HANDBOOK PART XII - A & B VILLAGE &TOWN DIRECTORY VILLAGE & TOWNWISE PRIMARY CENSUS ABSTRACT DISTRICT ROHTAfK v.s. CHAUDHRI DI rector of Census Operations Haryana Published by : The Government of Haryana, ]993 HARYANA DISTRICT ROHTAK Km5 0 5 10 15 10Km bLa:::EL__ :L I _ b -~ (Jl o DISTRICT ROHTAK CHANGE IN JURISDICTION 1981-91 z Km 10 0 10 Km L-.L__j o fTI r BOUNDARY, STATE! UNION TERRi10RY DIS TRICT TAHSIL AREA GAINED FROM DISTRIC1 SONIPAT AREA GAINED FROM DISTRICT HISAR \[? De/fl/ ..... AREA LOST TO DISTRICT SONIPAT AREA LOST TO NEWLY CREATED \ DISTRICT REWARI t-,· ~ .'7;URt[oN~ PART OF TAHSIL JHAJJAR OF ROHTAK FALLS IN C.D,BLO,CK DADRI-I . l...../'. ",evA DISTRICT BHIWANI \ ,CJ ~Q . , ~ I C.D.BLOCK BOUNDARY "- EXCLUDES STATUTORY ~:'"t -BOUNDARY, STATE I UNION TERRITORY TOWN (S) ',1 DISTRICT BOUNDARIES ARE UPDATED TAHSIL. UPTO I. 1.1990 C.D.BLOCK HEADQUARTERS '. DISTRICT; TAHSIL; C. D. BLOCK. NATIONAL HIGHWAY STATE HIGHWAY SH 20 C. O. BLOCKS IMPORTANT METALLED ROAD RS A MUNDlANA H SAMPLA RAILWAY LINE WITH STATION, BROAD GAUGE IiiiiI METRE GAUGE RS B GOHANA I BERI CANAL 111111""1111111 VILLAGE HAVING 5000 AND ABOVE POPULATION WITH NAME Jagsi C KATHURA J JHAJJAR URBAN AREA WITH POPULATION SIZE-CLASS I,!I,lII, IV & V" ••• ••• 0 LAKHAN MAJRA K MATENHAIL POST AND TELEGRAPH OFFICE PTO DEGREE COLLEGE AND TECHNICAL INSTITUTION .. [liiJ C'a E MAHAM L SAHLAWAS REST ClOUSE, TRAVELLERS' BUNGALOW' AND CANAL BUNGALOW RH, TB, CB F KALANAUR BAHADURGARH Other villages having PTO IRH/TBIC8 ~tc.,are shown as. -

E-MONITORING PORTAL : Assessor Report
Emonitoring Portal For Teacher Education Institute ASSESSOR’S MONITORING SHEET General Information Name of the institution The Aaryan College of Education Address Lakhan Majra State Haryana District Rohtak City LAKHAN MAJRA Pincode 124514 Email [email protected] STD Code 01257 Telephone No. with Code 265265 Year of establishment 2008 Hilly Region No Teacher Education Programmes (s) offered in the Institution Sanctioned Year of Sr. Intake (no. Sanctioned Programme NCTE Recognition Number Recognition No. of Basic Units by NCTE Students) 1 B.Ed F.NO./NRC/NCTE/HR-1191/2015/109844-48 2008 100 2 Details of Affiliation Sr. Name of the Affiliating Year of Programme Affiliation Number No. Body Affiliation MAHARISHI DAYANAND 1 B.Ed 2nd Year CB-IX//08/14760 2008 UNIVERSITY ROHTAK CHAUDHARY RANBIR SINGH 2 B.Ed 1st Year CRSU/Colleges/2016/3260-3649 2016 UNIVERSITY JIND Status of Affiliation Temporary Temporary Affiliation, it is valid up to 2018-08-31 Type of Management Self-financing Institution Managed by Self-financing Institution Independent Institution offering only Teacher Status of the Institution Education Programme (s) Institution meant for Co-Educational Whether the institute is accessible in all weather conditions and Yes through Pucca Road Name of the Nearest Railway Station LAKHAN MAJRA Campus & Infrastructure 1) Land Area and Built-up area (For Programmes: B.Ed) Total Land Built-Up Number of Name of Area Availability Compliance/Non-Compliance area (in Compliance/Non-Compliance Programnme Programme (in of Land sqm.) (s) sqm.) Ownership 1 B.Ed 4096 Compliance 1912 Compliance basis 2) Infrastructural Facilities Infrastructure Available Size in Sq. -

29 /Ttlt98l D GC Gurgaon Commerce
1 HARYANA GOVERNMENT HIGHER EDUCATION DEPARTMENT ORDER The Governor of Haryana is pleased to confirm the following Assista nt/Associate Professors (College Cadre) from the date of.successful completion of probation period: - Sr. Name of Asistant DOB College Subiect No, Professol Ms/Mrs/Mr. 1 Kamla Devi 2413/t972 GC Satnali Economics 2 Sharmila 5ltolt977 GCw Narnaul English Political 3 Kanta tl8/1977 GCW Unhani Science 4 Vikram Singh rsl3h972 GCW Unhani Geography 5 Rajni LOlDlr9Ts GCG Rewari Maths 6 Shamsher Singh LO/2/ L977 GC Mahendergarh History 7 Ashok Kumar s/617979 GC MahenderBarh English 8 Somveer 6191t977 GC Ateli Hindi 9 Sunita Mehra 79/sh973 GC Saha English 10 Sunil Kumar 7/917979 GCG Rewari Maths GCG Palwal 11 Manjit Kaur tzl3/1987 English (Kurukshetra) 72 Payal Rani 29 /ttlt98L D GC Gurgaon Commerce 13 Anita 3rlLzlt980 GC Dujana English Defence L4 Dinesh Kumar t4l2lt983 GC Karnal Studies 15 Jarnail Singh tol2he73 GC Satnali English 16 Raiwanti 2s/8lt98O GCW Murthal Commerce 77 Savita Nain 30l3lt978 GC Panipat English 18 Sanjay Kumar 3lsh978 GC kaithal English 19 Jyoti chahal 7/4/L984 GCW Gohana Commerce 20 Manju Yadav 721L(7983 GC Ateli Commerce 2t Sheela Devi 20/3/1982 GC Narwana History Physical 22 Satyajeet 7s/8he80 GC Ateli Education 23 Ramesh Kumar r/3/7979 GC Matak Majri Hindi 24 Bharati Yadav t9l8i198s GC Kanwali Physics 25 Sangita Yadav 70/2/1984 GC Kanwali Maths 26 Mukesh Yadav t4/9/7978 GC Satnali Maths 2 Sr. Name of Asslstant DOB College Subiect No Professor Ms/Mrc/Mr. -

Elected Members of Panchayat Samiti
Elected Members of Panchayat Samiti Name of the Designation Sr. No. State District Block Mobile No. / Landline No. -

Sarva Haryana Gramin Bank Head Office: Rohtak
SARVA HARYANA GRAMIN BANK HEAD OFFICE: ROHTAK Details of Branches (Districtwise) Sr.No District Branch Date of Opening Telephone No. 1 Jhajjar BADLI 09.08.1983 01276-240665 2 Jhajjar BAHADURGARH 16.03.1983 01276-230903 3 Jhajjar BARHANA 29.03.2011 01251-215622 4 Jhajjar BERI 06.05.1983 01251-220910 5 Jhajjar BHADANI 31.10.2013 94665-56688 6 Jhajjar BIROHAR 10.06.1986 01251-278204 7 Jhajjar CHHUCHHAKWAS 10.06.1983 01251-232163 8 Jhajjar DUBAL DHAN 28.03.1981 01251-228308 9 Jhajjar JAHAJGARH 05.05.1981 01251-234136 10 Jhajjar JAHANGIRPUR 23.03.2013 01251-264064 11 Jhajjar JHAJJAR 10.03.1983 01251-252146 12 Jhajjar KABLANA 09.08.1983 01251-239433 13 Jhajjar KANONDA 08.07.1983 01276-247326 14 Jhajjar KHANPUR KHURD 22.09.2011 82958-66988 15 Jhajjar KHERI JASSAUR 10.12.2011 01276-280140 16 Jhajjar LADAIN 22.02.2011 97299-97699 17 Jhajjar MANDANA 09.08.1983 01251-224076 18 Jhajjar MANDHOTHI 10.12.2011 01276-276166 19 Jhajjar MATAN HAIL 20.08.1987 01251-230190 20 Jhajjar NUNA MAJRA 10.08.1983 01276-250100 21 Jhajjar PARNALA 05.05.1983 01276-239486 22 Jhajjar SILANI 09.08.1983 01251-262188 23 Panipat BAPOLI 07.12.2006 0180-2586333 24 Panipat BARANA 02.07.2013 0180-2582001 25 Panipat ISRANA 07.07.2010 0180-2598200 26 Panipat PANIPAT 31.03.2008 0180-2641144 27 Panipat SAMALKHA 04.08.2010 0180-2574800 28 Panipat SANOLI KHURD 10.11.2006 0180-2567333 29 Panipat SEENK 15.02.2013 94661-97001 30 Rewari BHAKLI 10.11.1980 01259-275609 31 Rewari GUDIYANI 10.08.1983 01259-274141 32 Rewari JHARODA 10.08.1983 01259-273163 33 Rewari KAROLI 10.08.1983 01259-272227