Understanding Brachytherapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Institute for Clinical and Economic Review
INSTITUTE FOR CLINICAL AND ECONOMIC REVIEW FINAL APPRAISAL DOCUMENT BRACHYTHERAPY & PROTON BEAM THERAPY FOR TREATMENT OF CLINICALLY-LOCALIZED, LOW-RISK PROSTATE CANCER December 22, 2008 Senior Staff Daniel A. Ollendorf, MPH, ARM Chief Review Officer Julia Hayes, MD Lead Decision Scientist Pamela McMahon, PhD Sr. Decision Scientist Steven D. Pearson, MD, MSc President, ICER Associate Staff Michelle Kuba, MPH Sr. Technology Analyst Angela Tramontano, MPH Research Assistant © ICER, 2008 1 CONTENTS About ICER .................................................................................................................................. 3 Acknowledgments ...................................................................................................................... 4 Executive Summary .................................................................................................................... 5 Evidence Review Group Deliberation.................................................................................. 15 ICER Integrated Evidence Rating.......................................................................................... 21 Evidence Review Group Members........................................................................................ 24 Appraisal Overview.................................................................................................................. 28 Background ............................................................................................................................... -

Trends in Targeted Prostate Brachytherapy: from Multiparametric MRI to Nanomolecular Radiosensitizers
Nicolae et al. Cancer Nano (2016) 7:6 DOI 10.1186/s12645-016-0018-5 REVIEW Open Access Trends in targeted prostate brachytherapy: from multiparametric MRI to nanomolecular radiosensitizers Alexandru Mihai Nicolae1, Niranjan Venugopal2 and Ananth Ravi1* *Correspondence: [email protected] Abstract 1 Odette Cancer Centre, The treatment of localized prostate cancer is expected to become a significant Sunnybrook Health Sciences Centre, 2075 Bayview Ave, problem in the next decade as an increasingly aging population becomes prone to Toronto, ON M4N3M5, developing the disease. Recent research into the biological nature of prostate cancer Canada has shown that large localized doses of radiation to the cancer offer excellent long- Full list of author information is available at the end of the term disease control. Brachytherapy, a form of localized radiation therapy, has been article shown to be one of the most effective methods for delivering high radiation doses to the cancer; however, recent evidence suggests that increasing the localized radiation dose without bound may cause unacceptable increases in long-term side effects. This review focuses on methods that have been proposed, or are already in clinical use, to safely escalate the dose of radiation within the prostate. The advent of multiparametric magnetic resonance imaging (mpMRI) to better identify and localize intraprostatic tumors, and nanomolecular radiosensitizers such as gold nanoparticles (GNPs), may be used synergistically to increase doses to cancerous tissue without the -

High Dose-Rate Brachytherapy of Localized Prostate Cancer Converts
Open access Original research J Immunother Cancer: first published as 10.1136/jitc-2020-000792 on 24 June 2020. Downloaded from High dose- rate brachytherapy of localized prostate cancer converts tumors from cold to hot 1,2,3 1 1 1 Simon P Keam , Heloise Halse, Thu Nguyen, Minyu Wang , Nicolas Van Kooten Losio,1 Catherine Mitchell,4 Franco Caramia,3 David J Byrne,4 Sue Haupt,2,3 Georgina Ryland,4 Phillip K Darcy,1,2 Shahneen Sandhu,5 2,4 2,3 6 1,2 Piers Blombery, Ygal Haupt, Scott G Williams, Paul J Neeson To cite: Keam SP, Halse H, ABSTRACT organized immune infiltrates and signaling changes. Nguyen T, et al. High dose- rate Background Prostate cancer (PCa) has a profoundly Understanding and potentially harnessing these changes brachytherapy of localized immunosuppressive microenvironment and is commonly will have widespread implications for the future treatment prostate cancer converts tumors immune excluded with few infiltrative lymphocytes and of localized PCa, including rational use of combination from cold to hot. Journal for low levels of immune activation. High- dose radiation radio- immunotherapy. ImmunoTherapy of Cancer 2020;8:e000792. doi:10.1136/ has been demonstrated to stimulate the immune system jitc-2020-000792 in various human solid tumors. We hypothesized that localized radiation therapy, in the form of high dose- INTRODUCTION ► Additional material is rate brachytherapy (HDRBT), would overcome immune Standard curative- intent treatment options published online only. To view suppression in PCa. for localized prostate cancer (PCa) include please visit the journal online Methods To investigate whether HDRBT altered prostate radical prostatectomy or radiotherapy.1 (http:// dx. -

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

A Review of Rectal Toxicity Following Permanent Low Dose-Rate Prostate Brachytherapy and the Potential Value of Biodegradable Rectal Spacers
Prostate Cancer and Prostatic Disease (2015) 18, 96–103 © 2015 Macmillan Publishers Limited All rights reserved 1365-7852/15 www.nature.com/pcan REVIEW A review of rectal toxicity following permanent low dose-rate prostate brachytherapy and the potential value of biodegradable rectal spacers ME Schutzer1, PF Orio2, MC Biagioli3, DA Asher4, H Lomas1 and D Moghanaki1,5 Permanent radioactive seed implantation provides highly effective treatment for prostate cancer that typically includes multidisciplinary collaboration between urologists and radiation oncologists. Low dose-rate (LDR) prostate brachytherapy offers excellent tumor control rates and has equivalent rates of rectal toxicity when compared with external beam radiotherapy. Owing to its proximity to the anterior rectal wall, a small portion of the rectum is often exposed to high doses of ionizing radiation from this procedure. Although rare, some patients develop transfusion-dependent rectal bleeding, ulcers or fistulas. These complications occasionally require permanent colostomy and thus can significantly impact a patient’s quality of life. Aside from proper technique, a promising strategy has emerged that can help avoid these complications. By injecting biodegradable materials behind Denonviller’s fascia, brachytherpists can increase the distance between the rectum and the radioactive sources to significantly decrease the rectal dose. This review summarizes the progress in this area and its applicability for use in combination with permanent LDR brachytherapy. Prostate Cancer and Prostatic Disease (2015) 18, 96–103; doi:10.1038/pcan.2015.4; published online 17 February 2015 A BRIEF HISTORY OF LOW DOSE-RATE PROSTATE demonstrated an 82% 8-year bPFS for 1444 patients treated with BRACHYTHERAPY radioactive seed implant for low-risk disease;4 (2) a series by Originally described in 1917, low dose-rate (LDR) prostate Taira et al. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
www.kjurology.org DOI:10.4111/kju.2010.51.1.70 Case Report Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis Kyung Hwa Choi, Seung Hwan Lee, Won Sug Jung1, Byung Ha Chung Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, 1National Health Insurance Corporation Ilsan Hospital, Goyang, Korea We report a rare case of robot-assisted laparoscopic radical prostatectomy (RARP) in Article History: a patient with a preexisting penile prosthesis. In this case, we completed RARP without received 27 August, 2009 14 October, 2009 removing the reservoir by using a deflation-inflation technique, and there were no com- accepted plications related to the prosthesis. The patient had a negative surgical margin. The Corresponding Author: preserved three-piece inflatable penile prosthesis continued to function properly in 1 Byung Ha Chung month. Reservoir-preserving RARP is technically feasible and safe. However, it is im- Department of Urology, Yonsei portant to be aware of device-related complications. Long-term studies on the mechan- University Health System, Gangnam Severance Hospital, 712, Eonju-ro, ical survival rate and patient satisfaction should be also performed. Dogok-dong, Gangnam-gu, Seoul Key Words: Robotics, Prostatectomy, Penile prosthesis, Prostatic neoplasms 135-720, Korea TEL: +82-2-2019-3474 FAX: +82-2-3462-8887 E-mail: [email protected] Prostate cancer has been reported to occur most frequently CASE REPORT in men over 40 years of age. In organ-confined cases, radical prostatectomy is the treatment of choice. After the in- 1. Patient troduction of the da VinciⓇ surgical system (Intuitive The patient was a 64-year-old male diagnosed with aci- Surgical, Sunnyvale, USA), robot-assisted laparoscopic nar-type prostate adenocarcinoma with a Gleason score of radical prostatectomy (RARP) has become a mainstay of 6 (3+3) by prostate biopsy. -

Review White Paper (Pdf)
Brachytherapy: high precision, targeted radiotherapy Because life is for living Table of contents Executive summary 3 Introduction 4 Radiotherapy: present and future goals 5 Overview of brachytherapy 6 • Brachytherapy: high precision, targeted radiotherapy 6 Types of brachytherapy 7 Brachytherapy dosing 7 Brachytherapy efficacy and safety outcomes; patient benefits 8 • Brachytherapy in gynecological cancer 8 • Brachytherapy in prostate cancer 9 • Brachytherapy in breast cancer 12 • Brachytherapy in other cancers 14 • Brachytherapy in palliative care 15 Brachytherapy: setting benchmarks in radiation technology 15 • Advantages: technical and cost base 15 • Ongoing advances in brachytherapy result in improved outcomes and efficiency 16 Cost effectiveness: making efficient use of healthcare resources 17 Conclusions 19 Glossary 20 References 21 2 Brachytherapy: high precision, targeted radiotherapy Executive summary Radiotherapy is a key cornerstone of cancer care: this • The ability of brachytherapy to deliver high radiation White Paper reviews the role of brachytherapy – high doses over a short time period means patients can precision, targeted radiotherapy – in cancer treatment, complete treatment in days rather than the and discusses how it offers an effective, well tolerated weeks required for EBRT. For example, high dose rate radiation treatment option, tailored to the needs and (HDR) brachytherapy treatment for prostate cancer preferences of the individual patient. can be delivered in two treatment sessions, compared to several weeks with EBRT. This has important Brachytherapy combines two fundamental aims potential implications for patient compliance with of radiotherapy: an effective tumor dose with their radiotherapy treatment, as well as minimizing sparing of the surrounding tissue. Brachytherapy is impact on patients’ lives at the forefront of innovation in radiotherapy. -
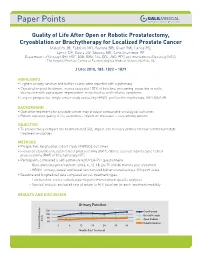
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

Permanent Source Brachytherapy for Prostate Cancer
American College of Radiology End User License Agreement ACR Appropriateness Criteria is a registered trademark of the American College of Radiology. By accessing the ACR Appropriateness Criteria®, you expressly agree and consent to the terms and conditions as described at: http://www.acr.org/~/media/ACR/Documents/AppCriteria/TermsandConditions.pdf Personal use of material is permitted for research, scientific and/or information purposes only. You may not modify or create derivative works based on American College of Radiology material. No part of any material posted on the American College of Radiology Web site may be copied, downloaded, stored in a retrieval system, or redistributed for any other purpose without the expressed written permission of American College of Radiology. Revised 2016 American College of Radiology ACR Appropriateness Criteria® PERMANENT SOURCE BRACHYTHERAPY FOR PROSTATE CANCER Expert Panel on Radiation Oncology–Prostate: Brian J. Davis, MD, PhD1; Al V. Taira, MD2; Paul L. Nguyen, MD3; Dean G. Assimos, MD4; Anthony V. D'Amico, MD, PhD5; Alexander R. Gottschalk, MD, PhD6; Gary S. Gustafson, MD7; Sameer R. Keole, MD8; Stanley L. Liauw, MD9; Shane Lloyd, MD10; Patrick W. McLaughlin, MD11; Benjamin Movsas, MD12; Bradley R Prestidge, MD, MS13; Timothy N. Showalter, MD, MPH14; Neha Vapiwala, MD.15 Summary of Literature Review Introduction/Background Improvements in permanent prostate brachytherapy (PPB) utilizing transrectal ultrasound (TRUS) guidance via a perineal template resulted in this procedure becoming a major treatment option for localized prostate cancer by the mid-1990s [1]. PPB is an outpatient procedure with short treatment time, rapid patient recovery, and demonstrated long-term efficacy. For men with low-risk disease, treatment efficacy is comparable to other primary treatment options [2-5]. -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder