About UP-TSU
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Research Article
Available Online at http://www.recentscientific.com International Journal of CODEN: IJRSFP (USA) Recent Scientific International Journal of Recent Scientific Research Research Vol. 10, Issue, 11(A), pp. 35764-35767, November, 2019 ISSN: 0976-3031 DOI: 10.24327/IJRSR Research Article SOME MEDICINAL PLANTS TO CURE JAUNDICE AND DIABETES DISEASES AMONG THE RURAL COMMUNITIES OF SHRAVASTI DISTRICT (U.P.) , INDIA Singh, N.K1 and Tripathi, R.B2 1Department of Botany, M.L.K.P.G. College Balrampur (U.P.), India 2Department of Zoology, M.L.K.P.G. College Balrampur (U.P.), India DOI: http://dx.doi.org/10.24327/ijrsr.2019.1011.4166 ARTICLE INFO ABSTRACT An ethnobotanical survey was undertaken to collect information from traditional healers on the use Article History: of medicinal plants in rural communities of district Shravasti Uttar Pradesh. The important th Received 4 August, 2019 information on the medicinal plants was obtained from the traditional medicinal people. Present th Received in revised form 25 investigation was carried out for the evaluation on the current status and survey on these medicinal September, 2019 plants. In the study we present 14 species of medicinal plants which are commonly used among the th Accepted 18 October, 2019 rural communities of Shravasti district (U.P.) to cure jaundice and diabetes diseases. This study is th Published online 28 November, 2019 important to preserve the knowledge of medicinal plants used by the rural communities of Shravasti district (U.P.), the survey of the psychopharmacological and literatures of these medicinal plants Key Words: have great pharmacological and ethnomedicinal significance. Medicinal plants, jaundice and diabetes diseases, rural communities of Shravasti. -

Modeling of Rainfall and Ground Water Fluctuation of Gonda District Uttar Pradesh, India
Int.J.Curr.Microbiol.App.Sci (2018) 7(5): 2613-2618 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 05 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.705.302 Modeling of Rainfall and Ground Water Fluctuation of Gonda District Uttar Pradesh, India Dinesh Kumar Vishwakarma1*, Rohitashw Kumar2, Kusum Pandey3, Vikash Singh4 and Kuldeep Singh Kushwaha5 1,2College of Agricultural Engineering and Technology, Sher-e-Kashmir University of Agricultural Sciences and Technology of Kashmir, Shalimar Campus Srinagar – Jammu and Kashmir, India 3Department of Soil and Water Conservation Engineering, Punjab Agricultural University, Ludhiana, Punjab 141004, India 4Department of Farm Engineering, Institute of Agricultural Sciences, Banaras Hindu University, Varanasi 221005 5Centre of Water Engineering and Management, Central University of Jharkhand – 835205, India *Corresponding author ABSTRACT Various quantitative analyses are required for complex and dynamic nature of water resources systems to manage it properly. Groundwater table fluctuations over time in shallow aquifer systems need to be evaluated for formulating or designing an K e yw or ds appropriate groundwater development scheme. This paper demonstrates a methodology Precipitation, for modeling rainfall- runoff and groundwater table fluctuations observed in a shallow unconfined aquifer Gonda District Utter Pradesh. The rainfall recharge contributed to its Ground water recharge, Ground annual increment in the ground in water reserve which in turn is reflected in the rise of water table water table during the post monsoon period. The linear regression model between water fluctuation, Karl table and annual rainfall was derived by Karl parson’s method. -

Page Flood Situation Report Date: 7 August 2018 Developed By
Flood Situation Report Date: 7 August 2018 Developed by: PoorvanchalGraminVikasSansthan (PGVS) Worsening situation started in 9th districts of eastern Uttar Pradesh due to Flood. Several districts in the eastern region of the state including Bahraich, Srawasti, Sitapur, Basti, Siddhartnagar, Barabanki, Lakhimpur, Mahrajganj and Gonda are flooded. As per newspapers (Dainik Jagarn and Hindustan 7 August 2018) 228 villages of the above-mentioned districts have been hit by the floods of which 83 are totally submerged and the villagers have been shifted to safer places. The district wise impact of the flood: • 24 villages affected (as per DDMA – 6 August 2018) in Bahraich district (28 hamlets in Shivpur blocks, 14 hamlets Mihipurwa, 31 hamlets in Mahsi blocks and reaming hamlets situated in Kaisarganj sub division) • 13 villages affected in Gonda district • 44 villages affected in Srawasti district (Mostly affected Jamunha block) • 29 villages affected in Barabanki but 20 villages affected of the Singrauli sub division. • 19 village affected in siddharthangar district • 18 villages affected in Lakhimpur Kheri district (09 villages in Lakhimpur sub division and 09 villages Dharaura sub division- source of information DDMA Lakhimpur) • 12 villages in Sitapur district • 08 villages in Basti district but pressure continued on embankment by Ghaghra River Flood situation in upstream area, Nepal in Sharda River (Mahakali): Due to effects of this, water in Sharda River and also rain fall in upstream areas and Uttarakhand of Mahakali (Sharda) River, water level arisen in Parigaon DHM station, Nepal with nearest warning level is 4.89 on 6 August 2018. Currently the water level of the Mahakali (Sharda) River is 4.65 Miter and trend is steady in Parigaon DHM station, Nepal. -
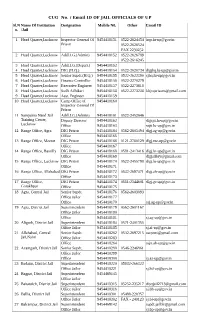
CUG No. / Email ID of JAIL OFFICIALS of up Sl.N Name of Institution Designation Mobile N0
CUG No. / Email ID OF JAIL OFFICIALS OF UP Sl.N Name Of Institution Designation Mobile N0. Other Email ID o. /Jail 1 Head Quarter,Lucknow Inspector General Of 9454418151 0522-2624454 [email protected] Prison 0522-2626524 FAX 2230252 2 Head Quarter,Lucknow Addl.I.G.(Admin) 9454418152 0522-2626789 0522-2616245 3 Head Quarter,Lucknow Addl.I.G.(Depart.) 9454418153 4 Head Quarter,Lucknow DIG (H.Q.) 9454418154 0522-2620734 [email protected] 5 Head Quarter,Lucknow Senior Supdt.(H.Q.) 9454418155 0522-2622390 [email protected] 6 Head Quarter,Lucknow Finance Controller 9454418156 0522-2270279 7 Head Quarter,Lucknow Executive Engineer 9454418157 0522-2273618 8 Head Quarter,Lucknow Sodh Adhikari 9454418158 0522-2273238 [email protected] 9 Head Quarter,Lucknow Asst. Engineer 9454418159 10 Head Quarter,Lucknow Camp Office of 9454418160 Inspector General Of Prison 11 Sampurna Nand Jail Addl.I.G.(Admin) 9454418161 0522-2452646 Training Center, Deputy Director 9454418162 [email protected] Lucknow Office 9454418163 [email protected] 12 Range Office, Agra DIG Prison 9454418164 0562-2605494 [email protected] Office 9454418165 13 Range Office, Meerut DIG Prison 9454418166 0121-2760129 [email protected] Office 9454418167 14 Range Office, Bareilly DIG Prison 9454418168 0581-2413416 [email protected] Office 9454418169 [email protected] 15 Range Office, Lucknow DIG Prison 9454418170 0522-2455798 [email protected] Office 9454418171 16 Range Office, Allahabad DIG Prison 9454418172 0532-2697471 [email protected] Office 9454418173 17 Range Office, DIG Prison 9454418174 0551-2344601 [email protected] Gorakhpur Office 9454418175 18 Agra, Central Jail Senior Supdt. -

Status of Kenaf (Hibiscus Cannabinus L) Diseases in the Districts of North Eastern Plain Zone of Uttar Pradesh R
G.J B.A.H.S., Vol.2 (1) 2013: 72-73 ISSN - 2319 – 5584 STATUS OF KENAF (HIBISCUS CANNABINUS L) DISEASES IN THE DISTRICTS OF NORTH EASTERN PLAIN ZONE OF UTTAR PRADESH R. K. Singh1*, S. R. Dubey1 & R. K. Srivastava2 1Veer Kunwar Singh University, Arrah-802301 Bihar 2N.D.U.A.T. Crop Research Station, Bahraich-271801 U.P. Abstract The incidence and survey of different diseases were worked out during 2009-10 and 2010-11 under natural disease pressure and observed that leaf mosaic (Begomovirus) was more severe followed by foot and stem rot (Phytophthora parasitica). The results indicated that over all incidence of leaf mosaic ranged from 65.66% (Bahraich) to 68.72% (Balrampur) whereas foot and stem rot ranged from 13.60% (Shravasti) to 16.36% (Gonda). Key words: Hibiscus cannabinus, diseases, foot and stem rot, leaf mosaic. Introduction Kenaf (Hibiscus cannabinus) a herbaceous annual plant similar to jute is quite popular in the western world because of its eco-friendly nature. It has high biological efficacy and ecological adaptability and can absorb CO2 and NO2 3-5 times faster than forests and its deep roots can improve the soil. The plant has an ideal blend of long and short fibers for many paper and paperboard products (Grower, 1989). It has been cultivated and used as cordage crop to produce twine, rope, gunny bags and sackcloth for six millennia (Charles, 2002) Cannabinus bark (bast) and core fibers each have desirable qualities. Bast fibers are used for specialty papers, tea bags, and grass mats (biodegradable mats impregnated with grass and/or flower seeds). -

Maternal & New Born Care Among Recently Delivered Women of Scheduled Caste Community Through the Role of Asha in Uttar Prade
World Wide Journal of Multidisciplinary Research and Development WWJMRD 2020; 6(5): 73-78 www.wwjmrd.com International Journal Peer Reviewed Journal Maternal & New born Care among Recently Delivered Refereed Journal Indexed Journal Women of Scheduled Caste Community through the Impact Factor MJIF: 4.25 E-ISSN: 2454-6615 Role of Asha in Uttar Pradesh, India Dr. Tridibesh Tripathy Homoeopathic & Public Dr. Tridibesh Tripathy, Anjali Tripathy, Dr. Umakant Prusty, Dr. Health Expert Master of Chintamani Nayak, Dr. Rakesh Dwivedi, Dr. Mohini Gautam, Public Health (Community Medicine) Course, Lucknow University, Lucknow, UP, Abstract India. When ASHAs were introduced in NRHM in 2005, their primary aim was to visit homes of newborns as the first program in UP operated through the ASHAs was the Comprehensive Child Survival Anjali Tripathy Program in 2008. Since then, tracking of all deliveries and all the newborns are an integral part of the Program Co-ordinator, Water work of ASHAs in all the primary health care programs operated by the NHM in UP (GOI, 2005, Aid, UP office, Lucknow, UP, GOUP, 2013). Evaluation studies on the performance of ASHAs was done since 2011 as by then India. ASHAs had actually worked in the field for a minimum period of 5 years. It is to be noted that National Rural Health Mission was rolled out in April 2005 but it took about one to two years for the Dr. Umakant Prusty states to hire ASHAs and put things in place right from the state to the village level (GOUP, 2013). In Research officer this article, a comprehensive feedback is elicited from the mothers of Scheduled Caste (SC) (Homoeopathy), Regional community from the last visit of ASHAs to their homes to visits during pregnancy & newborn care. -

HPCL-Retail Outlet Dealership-Oct-14-Final
1 2 3 4 5 6 7 8 9a 9b 10 11 12 83 Between Old Haiderganj Tiraha & Nakhas HINDUSTAN PETROLEUM CORPORATION LTD Chauraha On Tulsidas Marg Lucknow Regular 200 OPEN CC 20 20 25 4 Bidding 30 5 . .84 Between Babu Banarasi Das College (A Govt. of India Enterprise) Temple And Indira Nahar On Lucknow - Faizabad Road Lucknow Regular 200 OPEN CC 30 20 25 4 Bidding 30 5 . 85 Lucknow- Kanpur Road, NH-27 (old NH-25) Lucknow Regular 240 OBC CC 40 45 25 4 Bidding 30 5 . NOTICE FOR APPOINTMENT OF REGULAR / RURAL RETAIL OUTLET DEALERSHIPS 86 Indira Nagar On Road Connecting HINDUSTAN PETROLEUM CORPORATION LTD. (HPCL) proposes to appoint Retail Outlet dealers in UTTAR PRADESH at following locations: Shalimar Chauraha And Ring Road Lucknow Regular 230 OBC CC 20 20 25 4 Bidding 30 5 . 87 Between Km Stone 486 to 480 on Lucknow - LOCATIONS UNDER LUCKNOW RETAIL REGION Sitapur Road on LHS, NH24 (New NH 30) Lucknow Regular 230 OPEN CC 40 45 25 4 Bidding 30 5 . 88 Between Manoj Pandey Chauraha To Sl. Name of Revenue Type Estimated Category Type Minimum Finance to be arranged Mode of Fixed Security Hahneeman Chauraha In Gomti Nagar Lucknow Regular 220 OPEN CC 20 20 25 4 Bidding 30 5 . No location District of RO Sales of Dimension by the applicant Selection Fee / Deposit 89 Gomti Nagar Extension In Sector-4 Lucknow Regular 200 OPEN CC 26 20 25 4 Bidding 30 5 . SC * Monthly SC CC-1 Site of the site Minimum (Rs. in 90 Between Km Stone No. -

Gonda Aligarh Kanpur Nagar Banda
1 \ , : ~ ;•, ~..".,' • ,'>--, MF Gonda IV! F Aligarh IV! F Kanpur Nagar Banda "I UTTAR PRADESH MALE REPRODUCTIVE HEALTH SURVEY 1995-1996 • The EVALUATION Project Carolina Population Center University of North Carolina at Chapel Hill CB #8120 University Square Chapel Hill, North Carolina 25716-3997 USA 1997 USAID Contract Number: DPE-3060-00-1054-00 I The EVALUATION Project / PERFORM ii CONTRIBUTORS Joseph deGraft-Johnson • Amy Ong Tsui Bates Buckner Kaushalendra K. Singh Ingrid Bou-Saada Christina Fowler Claire Viadro Julia Beamish Maria Khan In collaboration with Centre for Population and Development Studies, Hyderabad Indian Institute for Health Management Research, Jaipur Marketing and Research Organization, New Delhi Operations Research Group, New Delhi CONTENTS Page Tables , vii Figures '.' xii Acknowledgments .................................................... xv Executive Summary 1 CHAPTER 1 INTRODUCTION 5 Background of survey 5 Survey design and implementation .. : 6 Selection of rural villages and households 7 Selection of urban blocks and households 8 CHAPTER 2 RESPONDENT BACKGROUND CHARACTERISTICS 14 CHAPTER 3 KNOWLEDGE OF AND ATTITUDES TOWARD FEMALE REPRODUCTIVE ISSUES 17 Knowledge of the menstrual cycle 17 Knowledge of pregnancy and childbirth complications 18 Perception of fertility problems 19 Locus of control for pregnancy 20 Wife's ability to practice contraception 21 Importance of pregnancy prevention f9r husbands wanting no more children 23 Importance of pregnancy prevention for husbands wanting more children 24 CHAPTER -

District Wise Activities That Can Be Taken up for Rejuvenation of Rivers with Focus for Support for Migrant Workers Returning Home
District wise activities that can be taken up for Rejuvenation of Rivers with focus for support for migrant workers returning home Various works and activities involved in rejuvenation of small river in Ganga basin which are tributaries of River Ganga can be taken up under MGNREGA for generation of employment for migrant workers returning home. Accordingly, a total of 68 districts located in Ganga basin have been identified and small rivers and tributaries of River Ganga/ its tributaries have been shortlisted. Rejuvenation of these small tributaries forms an important component of rejuvenating River Ganga. Various activities have also been identified which can be implemented during pre-monsoon periods in the catchment of these rivers which will also help in rejuvenating these rivers. The potential areas for works programs to provide employment opportunities to them can be through MGNREGA, CAMPA & other funds for small river rejuvenation and afforestation. The components of work for small river rejuvenation may include desilting, construction of clean dam & other structures for water harvesting & storage, afforestation in the catchment, protection work for water bodies. The list of these activities have also been identified and given in the enclosed statement. The list of activities are not exhaustive but is illustrative as applicable for concept. These activities are such that they may not involve highly skilled manpower for their implementation. Even unskilled or semi-skilled manpower can be utilized for their implementation. Out of 73 districts, 34 districts (S No 1 to 34) fall in Uttar Pradesh while 20 are in Bihar (S No 35 to 54). Similarly, 5 in Jharkhand (S No 55 to 59), 12 districts are located in Madhya Pradesh (S No 60 to 71), and 2 in Rajasthan (S No 72-73). -

2. Saving Newborn Lives in Uttar Pradesh
CS-28 USAID Saving Newborn Lives in Uttar Pradesh through Improved Management of Birth Asphyxia: Situational Analysis Facility Readiness for Knowledge and Skill of Coverage of Emergency Obstetric Care Providers Interventions for and Newborn Care Mothers and Newborns 2014 Newborn and Maternal Health Care at Facilities in Gonda and Aligarh Districts of Uttar Pradesh T H E INCLEN T R U S T I NTERNATIONAL 1 CS-28 USAID Saving Newborn Lives in Uttar Pradesh through Improved Management of Birth Asphyxia: Situational Analysis Report Prepared by The INCLEN Trust International F1/5, Okhla Industrial Area, Phase I, New Delhi, India-110020 For Save The Children- Bal Raksha Bharat 2 Disclaimer: This report is made possible by the support of the American people through the United States Agency for International Development (USAID). The content of this document are the sole responsibility of The INCLEN Trust International and do not necessarily reflect the views of USAID or the United States Government or Save The Children. 3 ACKNOWLEDGEMENTS We are greatly indebted to the support and encouragement extended by the following partners Department of Medical Health and Family Welfare, Government of Uttar Pradesh District Health Officials, District Gonda and Aligarh. All the staff posted at selected health facilities in Aligarh and Gonda All stakeholders who agreed to share their perception and views about the maternal and new born care All the heads (Gram Pradhans/Sarpanchs/Ward Members) of selected clusters (villages/wards) for extending their help. All the mothers and their families for sparing their valuable time to answer the questions asked by the community assessment team. -

4773-A-2017.Pdf
International Journal of Current Advanced Research ISSN: O: 2319-6475, ISSN: P: 2319-6505, Impact Factor: SJIF: 5.995 Available Online at www.journalijcar.org Volume 6; Issue 11, November 2017; Page No. 7577-7580 DOI: http://dx.doi.org/10.24327/ijcar.2017.7580.1184 Research Article TRADITIONAL USES OF HERBAL POTENTIAL FOR THE TREATMENT OF RHEUMATISM IN RAEBARELI DISTRICT (UTTAR PRADESH) Singh B. K.* Department of Botany, R.H.S.P.G. College Singramau, Jaunpur-222175, U.P ARTICLE INFO ABSTRACT Article History: The present study has been carried out among rural communities inhabited in different Received 6th August, 2017 areas of the Raebareli district (Uttar Pradesh) during 2008 to 2009 suffering with Received in revised form 25th rheumatism. The aim of the study was to explore and document herbal plants including September, 2017 inherent medicinal potential to be used in human healthcare practices, especially to cure Accepted 3rd October, 2017 rheumatism a most common but serious health problem of mankind. Total 32 plant species Published online 28th November, 2017 belonging to 26 families are identified which have been employed by the rural community of the study area to get rid of from this very popular problem. Voucher specimens of cited Key words: plant species were collected and identified following standard procedures of herbarium Herbal potential; Rural community; preparation and consulting relevant reputed flora. The plants have been enumerated with Rheumatism; Primary healthcare botanical names followed by local name, family, plant parts used, mode of administration and uses. Copyright©2017 Singh B. K. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

State and District Level Stakeholder's Perspective on Home Based
National Journal of Multidisciplinary Research and Development National Journal of Multidisciplinary Research and Development ISSN: 2455-9040; Impact Factor: RJIF 5.22 Received: 05-02-2020; Accepted: 06-03-2020; Published: 10-06-2020 www.nationaljournals.com Volume 5; Issue 2; 2020; Page No 03-07 State and district level stakeholder’s perspective on home based newborn care program in Uttar Pradesh, India Tridibesh Tripathy1, Umakant Prusty2, Chintamani Nayak3, Rakesh Dwivedi4, Mohini Gautam5 1 BHMS (Utkal University, Bhubaneswar), MD (BFUHS, Faridkot), MHA (TISS, Mumbai), Ph.D. in Health Systems Studies (TISS), Mumbai, Maharashtra, India 2 Research officer (Homoeopathy), Regional Research Institute (Homoeopathy), Puri, Odisha under Central Council for Research in Homoeopathy, Ministry of AYUSH, Government of India, Odisha, India 3 Assistant Professor, National Institute of Homoeopathy, Kolkata, West Bengal, Government of India, Kolkata, West Bengal, India 4 Associate Professor, Centre for Advanced Studies in Social Work, Department of Social Work, Lucknow University, Lucknow, Uttar Pradesh, India 5Assistant Professor, Centre for Advanced Studies in Social Work, Department of Social Work, Lucknow University, Lucknow, Uttar Pradesh, India Abstract When ASHAs were introduced in NRHM in 2005, their primary aim was to visit homes of newborns as the first program in UP operated through the ASHAs was the Comprehensive Child Survival Program in 2008. Since then, tracking of all deliveries and all the newborns are an integral part of the work of ASHAs in all the primary health care programs operated by the NHM in UP (GOI, 2005, GOUP, 2013). The current article examines the role, work & approach of ASHAs through the feedback of the program managers at district & state level.