Handover Report and Papers Federal Minister Monhsrc 2018.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Finding the Way (WILL)
A handbook for Pakistan's Women Parliamentarians and Political Leaders LEADING THE WAY By Syed Shamoon Hashmi Women's Initiative for Learning & Wi Leadership She has and shel willl ©Search For Common Ground 2014 DEDICATED TO Women parliamentarians of Pakistan — past, present and aspiring - who remain committed in their political struggle and are an inspiration for the whole nation. And to those who support their cause and wish to see Pakistan stand strong as a This guidebook has been produced by Search For Common Ground Pakistan (www.sfcg.org/pakistan), an democratic and prosperous nation. international non-profit organization working to transform the way the world deals with conflict away from adversarial approaches and towards collaborative problem solving. The publication has been made possible through generous support provided by the U.S. Bureau of Democracy, Human Rights and Labor (DRL), under the project titled “Strengthening Women’s Political Participation and Leadership for Effective Democratic Governance in Pakistan.” The content of this publication is sole responsibility of SFCG Pakistan. All content, including text, illustrations and designs are the copyrighted property of SFCG Pakistan, and may not be copied, transmitted or reproduced, in part or whole, without the prior consent of Search For Common Ground Pakistan. Women's Initiative for Learning & Wi Leadership She has and shel willl ©Search For Common Ground 2014 DEDICATED TO Women parliamentarians of Pakistan — past, present and aspiring - who remain committed in their political struggle and are an inspiration for the whole nation. And to those who support their cause and wish to see Pakistan stand strong as a This guidebook has been produced by Search For Common Ground Pakistan (www.sfcg.org/pakistan), an democratic and prosperous nation. -

National Assembly Secretariat
NATIONAL ASSEMBLY SECRETARIAT BULLETIN OF THE ASSEMBLY (52ND SESSION) Date Tuesday, the 20th February, 2018 (Private Members’ Day) Commenced at 10.35 A.M. Adjourned at 3.05 P.M. Total working hours 4 Hours 30 Minutes Presided by 1. Sardar Ayaz Sadiq, Speaker, National Assembly of Pakistan 2. Mr. Murtaza Javed Abbasi, Deputy Speaker National Assembly of Pakistan 3. Syed Naveed Qamar, Chairperson Attendance 221 1. TILAWAT AND NAAT 1. Tilawat and Naat by Dr. Qari Muhammad Yunas LEAVE APPLICATIONS The leave applications of the Members who requested for grant of leave were read out by the honourable Mr. Speaker and leave was granted. MOTION Ms. Saira Afzal Tarar, Minister for National Health Services, Regulations and Coordination moved the following motion, which was adopted by the House:- “That under rule 288 of the Rules of Procedure and Conduct of Business in the National Assembly, 2007, the requirement of rule 51 of the said Rules in respect of Private Business, to be transacted today, the 20th February, 2018 may be suspended in order to consider Government Bills.” 1 SUPPLEMENTARY ORDERS OF THE DAY LEGISLATIVE BUSINESS 49A. MS. SAIRA AFZAL TARAR, Minister for Ms. Saira Afzal Tarar, Minister for National Health National Health Services, Regulations and Services, Regulations and Coordination moved the Coordination to move that the Bill to motion which was adopted. provide for restructuring of health services academy as a degree awarding institute [The Health Services Academy (Restructuring) Bill, 2017], as reported by the Standing Committee, be taken into consideration at once. Each clause was submitted to the Assembly and stood part of the Bill. -

February 2018 Volume 09 Issue 02 Promoting Bilateral Relations | Current Affairs | Trade & Economic Affairs | Education | Technology | Culture & Tourism ABC Certified
Monthly Magazine on National & International Political Affairs, Diplomatic Issues February 2018 Volume 09 Issue 02 Promoting Bilateral Relations | Current Affairs | Trade & Economic Affairs | Education | Technology | Culture & Tourism ABC Certified “Publishing from Pakistan, United Kingdom/EU & will be soon from UAE , Central Africa, Central Asia & Asia Pacific” Member APNS Central Media List A Largest, Widely Circulated Diplomatic Magazine | www.diplomaticfocus.org | www.diplomaticfocus-uk.com | Member Diplomatic Council /diplomaticfocusofficial /DFocusOfficial will benefit President of Indonesia H.E. Ir. H. Joko Widodo February 2018 Volume 09 Issue 02 “Publishing from Pakistan, United Kingdom/EU & will be soon from UAE ” 08 18 24 40 08 Conflicts & wars will benefit no one: President Mamnoon Hussain and President of Indonesia Ir. President of Indonesia H. Joko Widodo have agreed to work together for peace in Afghanistan and said that peace in Afghanistan is necessary for the development and progress of the region. Both countries will work together in this regard 18 Nishan-i-Imtiaz (Military) to Commander On the occasion, the President said that Pakistan and Saudi Royal Saudi Naval Forces Vice Admiral Arabia are the closest friends and the depth of their relationship Fahad Bin Abdullah Al-Ghofaily is difficult to describe in words. 24 CPEC most important initiative of our Prime Minister Shahid Khaqan said that the China Pakistan generation: PM Abbasi Economic Corridor (CPEC) is the most important initiative of our generation. “This is perhaps the most important initiative of our generation and the most visible part of the Belt and Road Initiative,” he said while addressing the inauguration ceremony of the first-ever International Gwadar Expo. -

2. MR. AKRAM MASIH GILL to Invite Attention of Minister-In-Charge Of
NATIONAL ASSEMBLY SECRETARIAT ORDERS OF THE DAY for the meeting of the National Assembly to be held on Tuesday, the 25th January, 2011 at 10.00 a.m. 1. Recitation from the Holy Quran. CALLING ATTENTION NOTICE 2. SARDAR BAHADUR AHMED KHAN SIHAR CH. ANWAR ALI CHEEMA SARDAR SHAHJEHAN YOUSAF MS. MARVI MEMON MR. AKRAM MASIH GILL to invite attention of Minister-in-Charge of the Cabinet Secretariat to a matter of urgent public importance regarding non-utilization of huge funds for rehabilitation of the flood affectees, causing grave concern amongst the public. INTRODUCTION OF BILLS 3. MR. ZAHID HAMID MR. SHAHID KHAQAN ABBASI CH. MUHAMMAD BARJEES TAHIR MR. MUHAMMAD PERVAIZ MALIK MR. MUHAMMAD HANIF ABBASI ENGR. KHURRAM DASTGIR KHAN CHAUDHRY MAHMOOD BASHIR VIRK SARDAR AYAZ SADIQ SHAIKH ROHALE ASGHAR SAHIBZADA MUHAMMAD FAZAL-E- KARIM MR. MUHAMMAD AKHTAR KHAN KANJU MS. SAIRA AFZAL TARAR MS. ANUSHA REHMAN KHAN ADVOCATE JUSTICE (RETD) IFTIKHAR AHMED CHEEMA MR. NASEER BHUTTA MR. MUHAMMAD BALIGH-UR-REHMAN CH. SAUD MAJEED BEGUM NUZHAT SADIQ DR. NELSON AZEEM MR. BILAL YASIN MR. HUMAIR HAYAT KHAN ROKHRI MR. USMAN IBRAHIM MIAN MARGHOOB AHMAD MR. MURTAZA JAVED ABBASI DR. TARIQ FAZAL CHAUDHARY MS. TAHIRA AURANGZEB to move for leave to introduce a Bill to provide for the abolition of all discretionary quotas in housing schemes in the public sector [The Abolition of Discretionary Quotas in Housing Schemes Bill, 2011]. 4. Also to introduce the Bill, if leave is granted. 5. MS. SHERRY REHMAN to move for leave to introduce a Bill to provide a law for Right to Information [The Right to Information Bill, 2011]. -

S.No. Contituency Name of Member Status 1 NA-2 Eng. Hamid Ul Haq Khalil P 2 NA-3 Mr
NATIONAL ASSEMBLY SECRETARIAT (Notice Office) 29th Session 6th sitting held on Friday, the 19th February, 2016 The following Members National Assembly of Pakistan attended the sitting S.No. Contituency Name of Member Status 1 NA-2 Eng. Hamid ul Haq Khalil P 2 NA-3 Mr. Sajid Nawaz P 3 NA-4 Mr. Gulzar Khan P 4 NA-5 Dr. Imran Khattak P 5 NA-7 Maulana Muhammad Gohar Shah P 6 NA-8 Mr. Aftab Ahmad Khan Sherpao P 7 NA-10 Mr. Ali Muhammad Khan P 8 NA-11 Mr. Mujahid Ali P 9 NA-12 Engineer Usman Khan Tarakai P 10 NA-13 Mr. Aqibullah P 11 NA-17 Dr. Muhammad Azhar Khan Jadoon P 12 NA-18 Mr. Murtaza Javed Abbasi P 13 NA-19 Mr. Babar Nawaz Khan P 14 NA-21 Capt. Retd. Muhammad Safdar P 15 NA-22 Qari Muhammad Yousaf P 16 NA-27 Col. Retd. Amirullah Marwat P 17 NA-28 Mr. Sher Akbar Khan P 18 NA-29 Mr. Murad Saeed P 19 NA-30 Mr. Salim Rehman P 20 NA-31 Mr. Ibadullah P 21 NA-32 Mr. Iftikhar ud Din P 22 NA-36 Mr. Bilal Rehman P 23 NA-37 Mr. Sajid Hussain Turi P 24 NA-39 Dr. Syed Ghazi Gulab Jamal P 25 NA-41 Mr. Ghalib Khan P 26 NA-42 Mr. Muhammad Jamal ud Din P 27 NA-43 Mr. Bismillah Khan P 28 NA-47 Mr. Qaisar Jamal P 29 NA-48 Mr. Asad Umar P 30 NA-50 Mr. Shahid Khaqan Abbasi P 31 NA-51 Raja Muhammad Javed Ikhlas P 32 NA-53 Mr. -
Premiership of Mr. Shahid Khaqan Abbasi from 01
LIST OF FEDERAL MINISTERS I MINISTERS OF STATE AND ADVISERS I SPECIAL ASSISTANTS TO THE PRIME MINISTER DURING THE PREMIERSHIPOf , MR. SHAHID KHAOAN ABBASI,From 01-08-2017 to 31-05-2018. S.NO. NAME/ PERIOD PORTFOLIO PERIOD OF PORTFOLIO 04.08.2017 to 31.05.2018 2. Commerce and Textile. 04.08.2017 to 31.05.2018 3. Hafiz Abdul Kareem 04.08.2017 to 09.03.2018 04.08.2017 to 09.03.2018 Communications. 14.03.2018 to 31.05.2018 4.03.2018 to 31. Capital Administration and 4. Dr. Tariq Fazal Chaudhry 27.04.2018 to 31.05.2018 27.04.2018 Devel ment Division. 5. Engr. Khurram Dastgir Khan Defence. 04.08.2017 to 31.05.2018 04.08.20 1.0 018 Addl: Fore n Affai 201 to 31.05.2018 6. Rana Tanveer Hussain Defence Production. 04.08.2017 to 02.05.2018 04.0 Science & Techno Mr. Usman Ibrahim 7. Defence Production. 03.05.2018 to 31.05.2018 03.05.2018 Mr. Muhammad Baligh Ur 8 Federal Education and Rehman 04.08.2017 to 31.05.2018 Professional Training. 04.08.20 9. Mr. Muhammad Ishaq Dar Finance, Revenue and .08.2017 to 21.11.2017 04.08.2017 to 11.03.2018 Economic Affairs. Without Portfolio 22.11.2017 to 11.03.2018 10. Mr. Miftah Ismail Finance, Revenue and 27.04.2018 to 31.05.2018 27.04.2018 to 31.05.2018 Economic irs. 11. Khawaja Muhammad Asif Foreign Affairs. 04.08.2017 to 26.04.2018 04.08.2017 to 26. -

Pakistan EO Report Women Contested Constituencies
Acknowledgements The Researchers under its regional initiative Women and Politics in Asia Forum (WPAF) and its commitment for women equality and political empowerment designed the model for Observing Women Contested Constituencies. Women have been contesting General Elections not even in Pakistan but other countries of Asia; but due to unknown reasons there is very less research based documentation comparative research is available. With this background The Researchers undertook the task of Observing 65 Women Contested Constituencies in the General Elections 2008 in Pakistan and later go for the comparative research on common elements with the General Elections in other Asian Countries. In this work The Researchers was supported by its local focal organizations by providing 400 field observers and constituency coordinators. We also appreciate the efforts and dedication of our research team specially Sahibzada Saud and Rabia Khaliq for putting up unlimited hours in making this report possible. Our team of control room coordinators and trainers did an excellent job of training and coordinating throughout the project with the field teams. Lastly, this work was only possible with the financial assistance of The Asia Foundation. We hope that this first step towards the first ever documentation of women and their participation in the General Elections will help in the political empowerment of women. Aazar Ayaz Team Leader July 2008 Table of Contents Executive Summary .............................................................................................................1 -

98Th Session SENATE SECRETARIAT
98th Session SENATE SECRETARIAT ————— “QUESTIONS FOR ORAL ANSWERS AND THEIR REPLIES” to be asked at a sitting of the Senate to be held on Friday, the 8th November, 2013 DEFERRED QUESTIONS (i) Question No. 82 : Originally set down for answering on 8th March, 2013 (91st Session) (ii) Question Nos. 1, 2, 3, 8 : Originally set down for answering on 20th August, 2013 and 9. (97th Session) (iii) Question No. 91 : Originally set down for answering on 28th August, 2013 (97th Session) 82. *Col. (R) Syed Tahir Hussain Mashhadi: (Notice received on 09-01-2013 at 10:30 a.m.) Will the Minister for Overseas Pakistanis and Human Resource Development be pleased to state: (a) the initial amount of contribution made by the Government to the Workers Welfare Fund; and (b) the steps being taken by the Federal Government for further contribution in the Workers Welfare Fund alongwith its details? Pir Syed Sadaruddin Shah Rashidi: (a) An initial contribution of Rs. 100 million was made by the Federal Governemnt to Workers Welfare Fund at the time of its establishment in 1971. (b) Since WWF generates funds at its own, therefore, there are no steps under consideration of the Government for further contribution. 1. *Mr. Muhammad Talha Mehmood: (Notice received on 23-04-2013 at 11:20 a.m.) Will the Minister for Overseas Pakistanis and Human Resource Development be pleased to state: (a) the details of benefits given to the workers by the Employees’ Old Age Benefits Institution; and (b) the amount received by the Institution from the employers and also given to workers during the last five years with year-wise breakup? Pir Syed Sadaruddin Shah Rashidi: (a) Following benefits are given by EOBI to the insured workers and their survivors:— Old-age pension on attaining 60 years age for males and 55 years in case of mine workers and females. -

Office of Director Public Relations
PRESIDENT’S SECRETARIAT (PUBLIC) PRESS WING ----- ISLAMABAD AUGUST 04, 2017: President Mamnoon Hussain administered the oath of office to 27 Federal Ministers and 16 Ministers of State at an impressive and dignified ceremony held at the Aiwan-e-Sadr, Islamabad on Tuesday. Prime Minister Shahid Khaqan Abbassi was also present. Those sworn in as Federal Ministers included Mohammad Ishaq Dar, Kamran Micheal, Muhammad Pervaiz Malik, Hafiz Abdul Kareem, Engr. Khurram Dastgir Khan, Syed Javed Ali Shah, Rana Tanveer Hussain, Khawaja Muhammad Asif, Akram Khan Durrani, Ghulam Murtaza Khan Jatoi, Riaz Hussain Pirzada, Ahsan Iqbal, Lt. General (R) Salahuddin Tirmizi, Muhammad Barjees Tahir, Zahid Hamid, Mushahid Ullah Khan, Sardar Awais Ahmed Khan Leghari, Pir Syed Sadaruddin Shah Rashidi, Mir Hasil Khan Bizenjo, Khawaja Saad Rafique, Sardar Muhammad Yousaf, Lt. General (Retd) Abdul Qadir Baloch, Saira Afzal Tarar, Sikandar Hayat Khan Bosan, Sheikh Aftab Ahmed, Muhammad Baligh Ur Rehman and Molana Ameer Zaman. Dr. Tariq Fazal Chaudhary, Haji Muhammad Akram Ansari, Muhammad Junaid Anwaar Chaudhry, Abid Sher Ali, Jam Kamal Khan, Marriyum Aurangzeb, Anusha Rahman, Dr. Darshan, Muhammad Tallal Chaudhry, Barrister Mohsin Shahnawaz Ranjha, Barrister Usman Ibrahim, Abdul Rehman Khan Kanju, Ch. Jaffar Iqbal, Sardar Muhammad Arshad Khan Laghari, Pir Muhammad Amin Ul Hasnat Shah and Ghalib Khan took oath as Minsters of State. Speaker National Assembly Sardar Ayaz Sadiq, parliamentarians, senior politicians, diplomats and high level civil officials attended the oath-taking ceremony. The entire oath taking ceremony was administered in national language. ********** . -

Senate Reply
1 (248th Session) SENATE SECRETARIAT ————— “QUESTIONS FOR ORAL ANSWERS AND THEIR REPLIES” to be asked at a sitting of the Senate to be held on Wednesday, the 11th May, 2016 DEFERRED QUESTIONS (Questions Nos. 66, 80, 90, and 91 deferred on 19th April, 2016 (247th Session) *(Def). Question No. 66. Senator Mohammad Azam Khan Swati: (Notice received on 14-03-2016 at 03:00 p.m.) Will the Minister for Foreign Affairs be pleased to state: (a) the names of the countries where Pakistani official passport holders are allowed to enter without visa; and (b) the names of the countries citizens of which are allowed to enter in Pakistan without visa? Minister for Foreign Affairs: (a) The list showing the names of the countries where Pakistani official passport holders are allowed to enter without visa is attached at Annex-I. (b) Part b pertains to Ministry of Interior and accordingly the question was transferred to Ministry of Interior. 2 Annex-I Updated on March 25, 2016 *(Def). Question No. 80. Senator Col. (R) Syed Tahir Hussain Mashhadi: (Notice received on 18-03-2016 at 09:15 a.m.) Will the Minister for National Health Services, Regulations and Coordination be pleased to state: 3 (a) the details of registered and unregistered stents being used for heart patients in the country; (b) the steps being taken by the Government to control the use of unregistered stents in the country; and (c) whether there is any proposal under consideration of the Government to register imported stents, if so, the details thereof? Mrs. Saira Afzal Tarar: (a) The Federal Government under the Drugs Act, 1976 (XXXI of 1976) declared stent to be drug for the purpose of the said Act vide notification dated 5th November, 2009. -
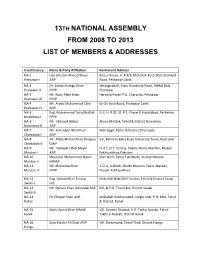
13Th National Assembly from 2008 to 2013 List of Members & Addresses
13TH NATIONAL ASSEMBLY FROM 2008 TO 2013 LIST OF MEMBERS & ADDRESSES Constituency Name & Party Affiliation Permanent Address NA-1 Haji Ghulam Ahmad Bilour Bilour House, H. # 3/2, Mohallah Raza Shah Shaheed Peshawar-I ANP Road, Peshawar Cantt. NA-2 Dr. Arbab Alamgir Khan Jehangirabad, Main University Road, Tehkal Bala, Peshawar-II PPPP Peshawar NA-3 Mr. Noor Alam Khan Haryana Payan P.O. Charpriza, Peshawar Peshawar-III PPPP NA-4 Mr. Arbab Muhammad Zahir 65-Sir Syed Road, Peshawar Cantt. Peshawar-IV ANP NA-5 Eng. Muhammad Tariq Khattak G-2, H. # 92, St. # 7, Phase-II, Hayatabad, Peshawar Nowshera-I PPPP NA-6 Mr. Masood Abbas Akora-Khattak, Tehsil & District Nowshera Nowshera-II ANP NA-7 Mr. Asfandyar Wali Khan Wali Bagh, Tehsil & District Charsadda Charsadda-I ANP NA-8 Mr. Aftab Ahmad Khan Sherpao 5-F, Rehman Baba Road University Town, Peshawar Charsadda-II QWP NA-9 Mr. Himayat Ullah Mayar H. # 1, D.C. Colony, Shamsi Road, Mardan, Khyber Mardan-I ANP Pakhtunkhwa,Pakistan NA-10 Moulana Mohammad Qasim Sher Garh, Tehsil Takhtbahi, District Mardan Mardan-II MMAP NA-11 Mr. Khanzada Khan 172-A, A-Block, Sheikh Matoon Town, Mardan, Mardan-III PPPP Khyber Pakhtunkhwa NA-12 Eng. Usman Khan Tarakai Mohallah Babi Khel Tarakai, Tehsil & District Swabi Swabi-I Ind NA-13 Mr. Pervaiz Khan Advocate ANP Vill. & P.O. Thand Koi, District Swabi Swabi-II NA-14 Pir Dilawar Shah ANP Mohallah Gulshanabad, Jungle Khel, P.O. KDA, Tehsil Kohat & District, Kohat NA-15 Mufti Ajmal Khan MMAP Vill. Ganderi Khattak, P.O. -

FINAL CR BULLETIN English
IDP IDP IDP CRISIS RESPONSE BULLETIN March 23, 2015 - Volume: 1, Issue: 10 IN THIS BULLETIN HIGHLIGHTS: English News 2-29 Agri-Economy: World Bank approves $187m for Irrigation System 02 Two-Day Training on Disaster Risk Reduction held 02 Women Turn Thar Drought into a Lesson on Sustainability 04 Natural Calamities Section 2-7 Pakistan: Proper Handling of the Dead Eases the Suffering of the 05 Safety and Security Section 8-13 Bereaved Battle for Pakistan: TDPs resettlement won’t be over until Dec 2016 08 Public Services Section 14-29 Insufficient security at Govt schools puts parents on tenterhooks 08 PM Nawaz vows to transform Karachi into ‘crime-free city’ 09 Maps 30-37 Pakistan does not want to be drawn into arms race with India: 10 President United Nation to monitor safety measures at Pakistani schools: Brown 11 Urdu News 55-38 COAS asks nation to join hands in war against terror 11 Employees dismissed to keep Pakistan's nuclear programme safe 12 Natural Calamities Section 55-53 Substandard tap changers may cause havoc to transformers 14 Suspension of mobile phone service perturbs Islooiites 14 Safety and Security section 52-46 APCNGA demands reopening of CNG stations in Punjab 15 Public Service Section 45-38 NTDCL of Pakistan signs 3 deals for 130 MW wind energy purchase 16 PAKISTAN WEATHER MAP WIND SPEED MAP OF PAKISTAN TEMPERATURE MAP OF PAKISTAN POLIO CASES IN PAKISTAN - 2015 MAPS CNG SECTOR GAS LOAD MANAGEMENT PLAN-SINDH VEGETATION ANALYSIS MAP OF PAKISTAN PUNJAB - FIRE INCIDENTS MAP SUICIDE ATTACKS IN PUNJAB (FROM OCTOBER 10,