ANATOMY of the ORBIT.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Eyelid Conjunctival Tumors
EYELID &CONJUNCTIVAL TUMORS PHOTOGRAPHIC ATLAS Dr. Olivier Galatoire Dr. Christine Levy-Gabriel Dr. Mathieu Zmuda EYELID & CONJUNCTIVAL TUMORS 4 EYELID & CONJUNCTIVAL TUMORS Dear readers, All rights of translation, adaptation, or reproduction by any means are reserved in all countries. The reproduction or representation, in whole or in part and by any means, of any of the pages published in the present book without the prior written consent of the publisher, is prohibited and illegal and would constitute an infringement. Only reproductions strictly reserved for the private use of the copier and not intended for collective use, and short analyses and quotations justified by the illustrative or scientific nature of the work in which they are incorporated, are authorized (Law of March 11, 1957 art. 40 and 41 and Criminal Code art. 425). EYELID & CONJUNCTIVAL TUMORS EYELID & CONJUNCTIVAL TUMORS 5 6 EYELID & CONJUNCTIVAL TUMORS Foreword Dr. Serge Morax I am honored to introduce this Photographic Atlas of palpebral and conjunctival tumors,which is the culmination of the close collaboration between Drs. Olivier Galatoire and Mathieu Zmuda of the A. de Rothschild Ophthalmological Foundation and Dr. Christine Levy-Gabriel of the Curie Institute. The subject is now of unquestionable importance and evidently of great interest to Ophthalmologists, whether they are orbital- palpebral specialists or not. Indeed, errors or delays in the diagnosis of tumor pathologies are relatively common and the consequences can be serious in the case of malignant tumors, especially carcinomas. Swift diagnosis and anatomopathological confirmation will lead to a treatment, discussed in multidisciplinary team meetings, ranging from surgery to radiotherapy. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
The Orbit Is Composed Anteri
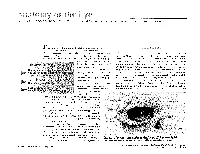
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Original Article Anatomic Study of the Lacrimal Fossa and Lacrimal Pathway
Original Article Anatomic study of the lacrimal fossa and lacrimal pathway for bypass surgery with autogenous tissue grafting Hai Tao, Zhi‑zhong Ma1, Hai‑Yang Wu, Peng Wang, Cui Han Purpose: To study the microsurgical anatomy of the lacrimal drainage system and to provide anatomical Access this article online evidence for transnasal endoscopic lacrimal drainage system bypass surgery by autogenous tissue grafting. Website: Materials and Methods: A total of 20 Chinese adult cadaveric heads in 10% formaldehyde, comprising www.ijo.in 40 lacrimal ducts were used. The middle third section of the specimens were examined for the following DOI: features: the thickness of the lacrimal fossa at the anterior lacrimal crest, vertical middle line, and posterior 10.4103/0301-4738.121137 lacrimal crest; the cross section of the upper opening, middle part, and lower opening of the nasolacrimal PMID: canal; the horizontal, 30° oblique, and 45° oblique distances from the lacrimal caruncle to the nasal cavity; ***** the distance from the lacrimal caruncle to the upper opening of the nasolacrimal duct; and the included Quick Response Code: angle between the lacrimal caruncle–nasolacrimal duct upper opening junction and Aeby’s plane. Results: The middle third of the anterior lacrimal crest was significantly thicker than the vertical middle line and the posterior lacrimal crest (P > 0.05). The horizontal distance, 30° oblique distance, and 45° oblique distance from the lacrimal caruncle to the nasal cavity exhibited no significant differences (P > 0.05). The included angle between the lacrimal caruncle and the lateral wall middle point of the superior opening line of the nasolacrimal duct and Aeby’s plane was average (49.9° ± 1.8°). -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

Cosmetic Lateral Canthoplasty: Lateral Topic Canthoplasty to Lengthen the Lateral Canthal Angle and Correct the Outer Tail of the Eye
Cosmetic Lateral Canthoplasty: Lateral Topic Canthoplasty to Lengthen the Lateral Canthal Angle and Correct the Outer Tail of the Eye Soo Wook Chae1, Byung Min Yun2 1BY Plastic Surgery Clinic, Seoul; 2Department of Plastic and Reconstructive Surgery, Jeju National University, Jeju, Korea There are many women who want larger and brighter eyes that will give a favorable impression. Correspondence: Soo Wook Chae Surgical methods that make the eye larger and brighter include double eyelidplasty, epican- BY Plastic Surgery Clinic, Wookyung Bldg. 5th Fl., 466 Apgujeong-ro, thoplasty, as well as lateral canthoplasty. Double eyelidplasty produces changes in the vertical Gangnam-gu, Seoul 06015, Korea dimension of the eyes, whereas epicanthoplasty and lateral canthoplasty create changes in Tel: +82-2-541-5522 the horizontal dimension of the eyes. Epicanthoplasty, a surgical procedure which enlarges Fax: +82-2-545-8743 the eye horizontally, is performed at the inner corner of the eye, whereas lateral canthoplasty E-mail: [email protected] enlarges the outer edge of the eye. In particular, if the slant of the palpebral fissure is raised and the horizontal dimension of the palpebral fissure is short, adjusting the slant of the pal- pebral fissure through lateral canthoplasty can achieve an enlargement of eye width and smoother features. Depending on the patient’s condition, even better results can be achieved if this procedure is performed in conjunction with other procedures, such as double eyelid- plasty, epicanthoplasty, eye roll formation surgery, fat graft, and facial bone contouring sur- gery. In this paper, the authors will introduce in detail their surgical method for a cosmetic lateral canthoplasty that lengthens the lateral canthal angle and corrects the outer tail of the eyes, in order to ease the unfavorable impression. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. -

PALPEBRAL APERTURE with SPECIAL REFERENCE to the SURGICAL CORRECTION of PSEUDOPTOSIS by Rudolf Aebli, M.D.*
THE RELATIONSHIP OF PSEUDOPTOSIS TO MUSCLE TROPIAS AND THE PALPEBRAL APERTURE WITH SPECIAL REFERENCE TO THE SURGICAL CORRECTION OF PSEUDOPTOSIS BY Rudolf Aebli, M.D.* BERKE'S (1) DISSERTATION on blepharoptosis in 1945 and Spaeth's (2) on the same subject in 1946 were both so complete and so admirable in all respects that there would be no justification at this time for a duplication of their contributions. On the other hand, with the exception of Kirby's (3) paper, in 1940, on ptosis associated with loss of elevation of the eyeball, relatively little has been written on the subject of pseudoptosis caused by vertical muscle tropias. Almost nothing, furthermore, has been written on the relationship of the palpebral aperture to these anomalies. This contribution has a threefold purpose: (1) to explain this relationship; (2) to outline the correct diagnostic procedure in ptosis of the eyelid which results from anomalies of this kind; and (3) to set forth the best methods of treatment for them. ANATOMIC CONSIDERATIONS Before it is possible to discuss intelligently the clinical aspects of muscle tropias and the relationship of the palpebral aperture to them, certain important (albeit elementary) anatomic considera- tions must be briefly summarized. When the eyelids are in their normal relationship to the eye- ball, the margin of the upper lid lies midway between the limbus and the pupillary margin of the iris, while the margin of the lower lid is at the limbus. When the eyes are opened normally, the lids are separated from each other by an elliptical space, the palpebral From the Department of Ophthalmology, New York University Post Graduate Medical School, and the University and Lenox Hill Hospitals, New York City. -

Morphometry of Bony Orbit Related to Gender in Dry Adult Skulls of South Indian Population
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Morphometry of Bony Orbit Related to Gender in Dry Adult Skulls of South Indian Population S. Senthil Kumar1, E. Gnanagurudasan2 1Professor, 2Ph.D Scholar, Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra University, Porur, Chennai, Tamil Nadu. Corresponding Author: E. Gnanagurudasan Received: 16/07/2015 Revised: 11/08/2015 Accepted: 12/08/2015 ABSTRACT Introduction: Orbit lodges important structures for vision and allows passage of fine neurovascular structures in it. The knowledge of orbital morphometry helps to protect those structures during various surgical procedures. Aim: To determine the morphometry of bony orbit in dry South Indian skulls related to gender and to compare the results with previous authors. Material and Methods: The material of the present study consists of 100 orbits from 50 skulls (right & left) which are identifiable of their sex. Foetal skulls and skulls with damages in the area of measurement were excluded. All the parameters were examined by a single observer using a vernier calliper, divider and millimetre scale. In each wall of the orbit, a bony landmark is chosen from where the distance of other bony structures is measured. Result: The result of the present study showed significance with respect to gender and side. Conclusion: The data of the present study will be helpful for various surgical approaches around the orbit. Keywords: orbit, South Indian skulls, morphometry. INTRODUCTION pyramidal cavity formed by seven bones The bony orbits are skeletal cavities namely maxilla, palatine, frontal, zygomatic, located on either side of the root of the nose. -

CT of Perineural Tumor Extension: Pterygopalatine Fossa
731 CT of Perineural Tumor Extension: Pterygopalatine Fossa Hugh D. Curtin1.2 Tumors of the oral cavity and paranasal sinuses can spread along nerves to areas Richard Williams 1 apparently removed from the primary tumor. In tumors of the palate, sinuses, and face, Jonas Johnson3 this "perineural" spread usually involves the maxillary division of the trigeminal nerve. The pterygopalatine fossa is a pathway of the maxillary nerve and becomes a key landmark in the detection of neural metastasis by computed tomogaphy (CT). Oblitera tion of the fat in the fossa suggests pathology. Case material illustrating neural extension is presented and the CT findings are described. Perineural extension is possibly the most insidious form of tumor spread of head and neck malignancy. After invading a nerve, tumor follows the sheath to reach the deeper connections of the nerve, escaping the area of a planned resection. Thus, detection of this form of extension is important in treatment planning and estimation of prognosis. The pterygopalatine fossa (PPF) is a key crossroad in extension along cranial nerve V. The second branch of the trigeminal nerve passes from the gasserian ganglion through the foramen rotundum into the PPF. Here the nerve branches send communications to the palate, sinus, nasal cavity, and face. Tumor can follow any of these routes proximally into the PPF and eventually to the gasserian ganglion in the middle cranial fossa. The PPF contains enough fat to be an ideal subject for computed tomographic (CT) evaluation. Obliteration of this fat is an important indicator of pathology, including perineural tumor spread. Other signs of perineural extension include enlargement of foramina, increased enhancement in the region of Meckel cave (gasserian ganglion), and atrophy of the muscles innervated by the trigeminal nerve. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria.