Director of Public Health Annual Report 1999
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

33 Birmingham
33 Birmingham - Pheasey via Perry Barr Mondays to Fridays Operator: NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB Carrs Lane (Stop BS16) 0500 0540 0600 0617 0633 0650 0700 0710 0720 0730 0740 0750 0800 0810 0820 0830 Newtown, Six Ways Aston (near) 0510 0550 0610 0627 0644 0701 0711 0721 0731 0742 0752 0802 0812 0822 0832 0842 Aldridge Road (Stop T2) 0434 0514 0529 0554 0614 0631 0648 0706 0716 0726 0736 0747 0757 0807 0817 0827 0837 0847 Birmingham City University, Wellhead Lane 0436 0516 0531 0556 0616 0633 0650 0708 0718 0728 0738 0749 0759 0809 0819 0829 0839 0849 Warren Farm, Chingford Road (before) 0442 0522 0537 0602 0622 0639 0656 0715 0725 0735 0746 0757 0807 0817 0827 0837 0847 0857 Kingstanding, Kingstanding Police Station 0448 0528 0543 0608 0628 0645 0702 0722 0732 0742 0754 0805 0815 0825 0835 0845 0855 0905 (before) Collingwood Centre (adjacent) 0453 0533 0548 0613 0633 0650 0707 0727 0737 0747 0800 0811 0821 0831 0841 0851 0901 0911 Mondays to Fridays Operator: NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB NXB Carrs Lane (Stop BS16) 0840 0850 0900 0910 0920 0930 0940 0950 1000 1010 1020 1030 1040 1050 1100 1110 1120 1130 Newtown, Six Ways Aston (near) 0852 0902 0912 0922 0932 0942 0952 1002 1012 1022 1032 1042 1052 1102 1112 1122 1132 1142 Aldridge Road (Stop T2) 0858 0908 0918 0928 0938 0948 0958 1008 1018 1028 1038 1048 1058 1108 1118 1128 1138 1148 Birmingham City University, Wellhead Lane 0900 0910 0920 0930 0940 0950 1000 1010 1020 1030 1040 1050 1100 1110 1120 1130 1140 -

West Midlands Schools
List of West Midlands Schools This document outlines the academic and social criteria you need to meet depending on your current secondary school in order to be eligible to apply. For APP City/Employer Insights: If your school has ‘FSM’ in the Social Criteria column, then you must have been eligible for Free School Meals at any point during your secondary schooling. If your school has ‘FSM or FG’ in the Social Criteria column, then you must have been eligible for Free School Meals at any point during your secondary schooling or be among the first generation in your family to attend university. For APP Reach: Applicants need to have achieved at least 5 9-5 (A*-C) GCSES and be eligible for free school meals OR first generation to university (regardless of school attended) Exceptions for the academic and social criteria can be made on a case-by-case basis for children in care or those with extenuating circumstances. Please refer to socialmobility.org.uk/criteria-programmes for more details. If your school is not on the list below, or you believe it has been wrongly categorised, or you have any other questions please contact the Social Mobility Foundation via telephone on 0207 183 1189 between 9am – 5:30pm Monday to Friday. School or College Name Local Authority Academic Criteria Social Criteria Abbot Beyne School Staffordshire 5 7s or As at GCSE FSM or FG Alcester Academy Warwickshire 5 7s or As at GCSE FSM Alcester Grammar School Warwickshire 5 7s or As at GCSE FSM Aldersley High School Wolverhampton 5 7s or As at GCSE FSM or FG Aldridge -

WEDNESBURY (Inc
HITCHMOUGH’S BLACK COUNTRY PUBS WEDNESBURY (Inc. Kings Hill, Mesty Croft) 3rd. Edition - © 2014 Tony Hitchmough. All Rights Reserved www.longpull.co.uk INTRODUCTION Well over 40 years ago, I began to notice that the English public house was more than just a building in which people drank. The customers talked and played, held trips and meetings, the licensees had their own stories, and the buildings had experienced many changes. These thoughts spurred me on to find out more. Obviously I had to restrict my field; Black Country pubs became my theme, because that is where I lived and worked. Many of the pubs I remembered from the late 1960’s, when I was legally allowed to drink in them, had disappeared or were in the process of doing so. My plan was to collect any information I could from any sources available. Around that time the Black Country Bugle first appeared; I have never missed an issue, and have found the contents and letters invaluable. I then started to visit the archives of the Black Country boroughs. Directories were another invaluable source for licensees’ names, enabling me to build up lists. The censuses, church registers and licensing minutes for some areas, also were consulted. Newspaper articles provided many items of human interest (eg. inquests, crimes, civic matters, industrial relations), which would be of value not only to a pub historian, but to local and social historians and genealogists alike. With the advances in technology in mind, I decided the opportunity of releasing my entire archive digitally, rather than mere selections as magazine articles or as a book, was too good to miss. -

Public Health Area Profiles December 2012
Walsall Area Partnership Public Health Profile: Aldridge/Pheasey/Streetly/Walsall Wood Public Health Area Profiles December 2012 VERSION 2 Darlaston/ Bentley Area 2: Aldridge/Pheasey/ Aldridge/Pheasey/Streetly/WalsallStreetly/Walsall Wood Wood Page of 34 Walsall Area Partnership Public Health Profile: Aldridge/Pheasey/Streetly/Walsall Wood Executive Summary The Area Partnership has 5 communities within it’s bound- ary (Approx 48,000 population): Aldridge (12,700) Aldridge North (4,100) Pheasey (8,800) Streetly (13,500) & Walsall Wood (8,900) The population is on the whole older than the Walsall av- erage, with much higher %’s of both men and women aged 65 and over The area has a relatively small number of residents from BME communities—around 3-4% Compared to the majority of Walsall, residents in the Area Partnership are relatively well-off economically. Most live in small areas in the least deprived half of the country. Geographically, the area partnership shares borders with South Staffordshire and Birmingham East and North PCT’s. Residents are likely to access some primary and secondary care health services outside of Walsall Health Priorities: Generally, health outcomes are better in communities in this Area Partnership than Walsall averages. Indicators of child health are good in the area with relatively low Infant Mortality rates and lower levels of childhood obesity. Sex- ual health is also generally good in the area (low teenage pregnancies and Chlamydia infection levels). Life expectan- cy, as defined by current average age at death is a number of years higher than the rest of Walsall for both men and women. -
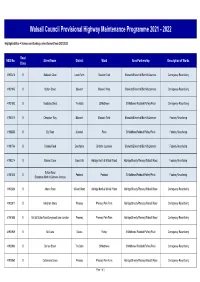
2021-2022 Works Programme.Xlsx
Walsall Council Provisional Highway Maintenance Programme 2021 - 2022 Highlighted Blue = Scheme and funding carried forward from 2021/2022 Road NSG No. Street Name District Ward Area Partnership Description of Works Class 41900414 U Bakewell Close Lower Farm Bloxwich East Bloxwich/Blakenhall/Birchills/Leamore Carriageway Resurfacing 41901945 U Station Street Bloxwich Bloxwich West Bloxwich/Blakenhall/Birchills/Leamore Carriageway Resurfacing 41901503 U Teddesley Street The Butts St Matthews St Matthews/ Paddock/Palfrey/Pleck Carriageway Resurfacing 41903016 U Chepstow Way Bloxwich Bloxwich West Bloxwich/Blakenhall/Birchills/Leamore Footway Resurfacing 41902338 U Ely Road Alumwell Pleck St Matthews/Paddock/Palfrey/Pleck Footway Resurfacing 41901746 U Faraday Road Beechdale Birchills - Leamore Bloxwich/Blakenhall/Birchills/Leamore Footway Resurfacing 41903214 U Robson Close Brownhills Aldridge North & Walsall Wood Aldridge/Streetly/Pheasey/Walsall Wood Footway Resurfacing Sutton Road 41901448 B Paddock Paddock St Matthews/Paddock/Palfrey/Pleck Footway Resurfacing (Broadway North to Greaves Avenue) 41902864 U Adams Road Walsall Wood Aldridge North & Walsall Wood Aldridge/Streetly/Pheasey/Walsall Wood Carriageway Resurfacing 41900017 U Allingham Grove Pheasey Pheasey Park Farm Aldridge/Streetly/Pheasey/Walsall Wood Carriageway Resurfacing 41901488 B B4155 Sutton Road/Longwood Lane Junction Pheasey Pheasey Park Farm Aldridge/Streetly/Pheasey/Walsall Wood Carriageway Resurfacing 41900939 U Bell Lane Delves Palfrey St Matthews/ Paddock/Palfrey/Pleck Carriageway Resurfacing 41900966 U Borneo Street The Butts St Matthews St Matthews/ Paddock/Palfrey/Pleck Carriageway Resurfacing 41900063 U Cattermole Grove Pheasey Pheasey Park Farm Aldridge/Streetly/Pheasey/Walsall Wood Carriageway Resurfacing Page 1 of 3 Walsall Council Provisional Highway Maintenance Programme 2021 - 2022 Highlighted Blue = Scheme and funding carried forward from 2021/2022 Road NSG No. -

Pheasey Park Farm January 2020 Version - FINAL Councillors
Ward Walk Profile: Pheasey Park Farm January 2020 Version - FINAL Councillors Name Party Elected on: Cllr Adrian Andrew Conservatives 4 May 2000 Cllr Mike Bird Conservatives 1 May 1980 Cllr Christopher Towe Conservatives 1 May 2003 Geography Covers 7.58 sq km (758 ha) Makes up 7.3% of the area of Walsall borough Population density of 15.0 people per hectare (lower than borough average of 27.3) Source: Ordnance Survey; ONS, Mid-2018 Population Estimates Assets Source: Ordnance Survey Population Source: ONS, Mid-2018 Population Estimates Ethnicity 25.0 20.0 15.0 % 10.0 5.0 0.0 Asian British Indian Pakistani Bangladeshi Chinese Other Ward Borough Only 13% minority ethnic residents Asian is the largest minority group at 6.5% (much less than Walsall 15.2%) Of the Asian minority group, Indian is most prolific at 4.4% (higher than 6.1% for borough) Source: ONS, 2011 Census Housing Composition Tenure . 4,539 households (with at least 1 usual resident) . Increase of 6.4% since 2001 (Proportion of borough total 4.2%) . Average household size: 2.4 residents per h/hold (Walsall average 2.5) . 3.1% of households ‘overcrowded’* (Walsall av. 6.5%) . 2.9% of households without central heating (Walsall average 2.8%) . Low proportion of socially and privately rented properties compared to borough . Above average (41.6%) mortgage owned (31.9%) Source: ONS, 2011 Census Social Segmentation - Groups The largest groups of households are classified as group F – Senior Security (41%) & group H – Aspiring Homemakers (29%) Most effective communication route Least effective communication routes Source: Experian - Mosaic Public Sector Profiler 2019; Ordnance Survey LLPG Address file 2019 Economic Summary • 82.6% of working age people in Pheasey Park Farm ward were economically active. -

Wolverhampton City Council OPEN EXECUTIVE DECISION ITEM (AMBER)
Agenda Item: 5 Wolverhampton City Council OPEN EXECUTIVE DECISION ITEM (AMBER) SPECIAL ADVISORY GROUP Date: 28 October 2011 Portfolio(s) ALL Originating Service Group(s) DELIVERY Contact Officer(s)/ SUSAN KEMBREY KEY DECISION: YES Telephone Number(s) 4300 IN FORWARD PLAN: YES Title BOUNDARY COMMISSION REVIEW OF PARLIAMENTARY CONSTITUENCIES – WEST MIDLANDS REGION CONSULTATION ON INITIAL PROPOSALS Recommendation (a) That the initial proposals of the Boundary Commission for England for the review of Parliamentary Constituencies in the West Midland region England as detailed in Sections 2 and 3 of the report be noted (b) That the Special Advisory Group recommend Cabinet to invite the three political groups to formulate their individual views on the proposals set out in the consultation paper for submission to the Boundary Commission direct. 1 1.0 PURPOSE 1.1 To advise of the consultation exercise on the initial proposals of the Boundary Commission for the review of Parliamentary Constituencies in the West Midland region and the date to respond to the consultation. 2.0 BACKGROUND 2.1 The Boundary Commission for England (BCE) is an independent and impartial non- departmental public body which is responsible for reviewing Parliamentary constituency boundaries in England. The BCE conduct a review of all the constituencies in England every five years. Their role is to make recommendations to Parliament for new constituency boundaries. The BCE is currently conducting a review of all Parliamentary constituency boundaries in England based on new rules laid down by Parliament. These rules involve a reduction in the number of constituencies in England (from 533 to 502) and stipulate that every constituency, apart from two specific exemptions, must have an electorate no smaller than 72,810 and no larger than 80,473. -

Metro Extension Proposals
N G R L B G ICK L R Museum T O W ARDW W H ON RD. S A A T D O OAD WOLVE R D H HARDWICK R RHAM E W O LITTLE PTO S H L S W O N ST. T E A A T A I U LH Y O E .P F OU D H R SE A H . R N D N Walsall U R O O L IC AD A D S L R A W T L S L L KEY O Art Galery BR LINC H T ID U O L A STREETLY R . GE N R S A N R D T T N S . B S O O A Walsall I O E L T O A D B E RID E D A OA GEM . N O R AN W Y ST. CHUCKERY D W OLE WALSALL E F L P Metro proposed extension L B C A H R T S U I S . N N Great Barr RouteE C W T TOWN T K K . S C D S T ER ROA . Y E Y S E T R ‘The Grange’ OL N CENTRE D F E Alignment under review/ S . D C A E S B A K V H U P A L IN Theatre TON Blue Coat E T D U L R L A Q N S IL D . H . R O R E R I R O ON Z A subject to change Bracebridge N D A M L C O D Y S D A L C R School G T. -

Streetly January 2020 Version - FINAL Councillors
Ward Walk Profile: Streetly January 2020 Version - FINAL Councillors Name Party Elected on: Cllr Brian Douglas- Conservatives 13 November 1980 Maul Cllr Sat Johal Conservatives 2 May 2019 Cllr Suky Samra Conservatives 3 May 2018 Geography . Covers 5.83 sq km (583 ha) . Makes up 5.6% of the area of Walsall borough . Population density of 23.4 people per hectare (lower than borough average of 27.3) Source: Ordnance Survey; ONS, Mid-2018 Population Estimates Assets Source: Ordnance Survey Population Source: ONS, Mid-2018 Population Estimates Ethnicity . 14% minority ethnic residents . Asian is the largest minority group at 8.9% (on par with Walsall average of 15.2%) . Of the Asian minority group, Indian is the most prolific at 6.1% Source: ONS, 2011 Census Housing Composition Tenure . 5,710 households (with at least 1 usual resident) . Increase of 12.6% since 2001 (Proportion of borough total 5.3%) . Average household size: 2.4 residents per h/hold (similar to Walsall average of 2.5) . 2.3% of households ‘overcrowded’* (Walsall average 6.5%) . 1.4% of households without central heating (Walsall average 2.8%) . Low proportion of socially rented (1.6%) properties compared to borough (24.1%) . Above average (31.9%) mortgage owned Source: ONS, 2011 Census (41.6%) Social Segmentation - Groups The largest groups of households are classified as group B – Prestige Positions (29%) & group F – Senior Security (26%) Most effective communication route Least effective communication routes Source: Experian - Mosaic Public Sector Profiler 2019; Ordnance Survey LLPG Address file Economic Summary • 82.6% of working age people in Streetly ward were economically active. -

'10 Lichfield to Wednesbury' (Pdf, 512KB)
L CHF ELD STAFFORDSH RE West Midlands Key Route Network WALSALL LichfieldWOLVERHAMPTON to Wednesbury WEST BROMW CH DUDLEY BRMNGHAM WARW CKSH RE WORCESTERSH RE SOL HULL COVENTRY Figure 1 12 A5 A38, A38(M), A47, A435, A441, A4400, A4540, A5127, B4138, M6 L CHF ELD Birmingham West Midlands Cross City B4144, B4145, B4148, B4154 11a Birmingham Outer Circle A4030, A4040, B4145, B4146 Key Route Network A5 11 Birmingham to Stafford A34 Black Country Route A454(W), A463, A4444 3 2 1 M6 Toll BROWNH LLS Black Country to Birmingham A41 M54 A5 10a Coventry to Birmingham A45, A4114(N), B4106 A4124 A452 East of Coventry A428, A4082, A4600, B4082 STAFFORDSH RE East of Walsall A454(E), B4151, B4152 OXLEY A449 M6 A461 Kingswinford to Halesowen A459, A4101 A38 WEDNESF ELD A34 Lichfield to Wednesbury A461, A4148 A41 A460 North and South Coventry A429, A444, A4053, A4114(S), B4098, B4110, B4113 A4124 A462 A454 Northfield to Wolverhampton A4123, B4121 10 WALSALL A454 A454 Pensnett to Oldbury A461, A4034, A4100, B4179 WOLVERHAMPTON Sedgley to Birmingham A457, A4030, A4033, A4034, A4092, A4182, A4252, B4125, B4135 SUTTON T3 Solihull to Birmingham A34(S), A41, A4167, B4145 A4038 A4148 COLDF ELD PENN B LSTON 9 A449 Stourbridge to Wednesbury A461, A4036, A4037, A4098 A4123 M6 Stourbridge to A449, A460, A491 A463 8 7 WEDNESBURY M6 Toll North of Wolverhampton A4041 A452 A5127 UK Central to Brownhills A452 WEST M42 A4031 9 A4037 BROMW CH K NGSTAND NG West Bromwich Route A4031, A4041 A34 GREAT BARR M6 SEDGLEY West of Birmingham A456, A458, B4124 A459 M5 A38 A461 -

Review of Baseline Conditions
Walsall Site Allocation Document (SAD) and Town Centre Action Plan (AAP) Sustainability Appraisal Report (March 2016) 4. Review of ‘Baseline’ Evidence 4.1 Background to Review Appendix E to the Revised SA Scoping Report (v2 May 2013) summarises the baseline evidence reviewed by the Council at the scoping stage, by SA Topic, and Chapters 5 and 6 of the report provides a summary of existing environmental, economic and social conditions and problems, how they are likely to develop, and the areas likely to be affected. This chapter provides an updated summary of ‘baseline’ environmental, social and economic conditions, which is based on the most up-to-date evidence available at the time the SA Framework was reviewed in July 2015. The baseline date for the evidence used in the appraisal (unless otherwise specified) is April 2015, although more up-to-date information has been used where available. 4.2 Development of Evidence Base Evidence Used in Appraisal and Plan Preparation Schedule 2 of the SEA Regulations states that the SA Report should include a description of: “The relevant aspects of the current state of the environment and the likely evolution thereof without implementation of the plan or programme;” “The environmental characteristics of areas likely to be significantly affected;” and “Any existing environmental problems which are relevant to the plan or programme, including areas of particular environmental importance,” such as ‘European Sites’ designated under the Habitats and Birds Directives.1 This Chapter addresses these requirements (see Appendix P). As the SA is an integrated assessment that includes EqIA and HIA as well as SEA, the baseline evidence must include 1 These are sites of European importance for biodiversity, including sites which are designated or proposed to be designated as Special Areas of Conservation (SAC), Special Protection Areas (SPAs) and Ramsar sites. -

View Walsall's Local Climate Impacts Profile (LCLIP)
Local Climate Impacts Profile For Walsall Council Project Manager: Carol Edmondson, Climate Change Team, Walsall Council Telephone: 01922 652864 E-mail: [email protected] Research by: Groundwork Black Country Telephone: 0121 530 5500 Email: [email protected] Contents 1 Executive Summary 1.1 Background 2 1.2 Summary of results 3 1.3 Identified costs 3 1.4 Recommendations 4 2 Background 2.1 Project Background 7 2.2 Introduction to a Local Climate Impacts Profile (LCLIP) 7 2.3 Methodology 8 2.4 Classification of extreme weather impacts 8 3 The local climate and weather 3.1 Geographical context 9 3.2 Temperature 9 3.3 Precipitation 12 3.4 Wind 13 3.5 Storms 15 3.6 Frost/snow 16 3.7 Atmospheric particulates 17 3.8 Humidity 18 3.9 Climate Change 19 4 Service Impacts 4.1 Storms 21 4.2 Rain / flooding 21 4.3 Sun / heat 24 4.4 Snow and ice 26 5. Conclusion 28 Appendix 1 30 National Indicators relating to climate Appendix 2 31 Meteorological stations, glossary and references Appendix 3 32 Media Trawl Database 2 1 Executive Summary 1.1 Background The weather has historically had a major impact upon the way human society has developed. More than ever before changing weather patterns have the potential to impact heavily upon how we live our lives. It is now an accepted scientific fact that our climate is changing, and local authorities must act proactively to adapt to the world of tomorrow. The concept of ‘future proofing’ is now essential to local and central Governance.