Pathophysiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Neuroophthalmology
Neuroophthalmology MAREK MICHALEC, MD PHD Clinic of Ophthalmology Faculty Hospital Brno and Masaryk University Version 12/2019 Content • Visual pathway affection • Diseases and affections of optic nerve • Optic chiasm pathology • Pathology of retrochiasmic part • Eye movement disorders • Binocular diplopia • Pupillary reaction abnormalities • Anisocoria • Combined disorders Examination - part I • Medical history • subjective (visual loss, diplopia) • When it started/ how long lasts it? • Does it change in time/ during the day? • Any progression? • What about the fellow eye? • Other signs? • Personal medical history? • Pharmacological history? • objective (pupillary dysfunction, eye movement disorders, ptosis of upper eyelid, red eye) Examination - part II • Visual acuity • Without and with correction • Monocular vision / binocular vision • Basic ophthalmological examination • Anterior segment (by slit lamp) • Posterior segment - arteficial mydriasis is essential (indirect ophthalmoscopy) • Visual field examination (static / kinetic perimetry) Examination - part III • Basic examination (GP) • Neurological examination • Intracranial conditions (including MRI) • neurological signs • Endocrinology • Thyroid associated orbitopathy / ophthalmopathy • Pituitary dysfunction Examination - part IV • Imaging techniques • Ultrasonography (eye bulb, orbit) • X-ray of skull (orbit, paranasal cavities) • Computerised Tomography of head (brain, skull bones, orbital bones) • MRI of head (brain, orbital structures) Optic nerve disorders Clinical signs • -

Ministry of Public Health of Ukraine Ukrainian Medical Stomatological Academy
Ministry of Public Health of Ukraine Ukrainian Medical Stomatological Academy Approved At the meeting of the department of neurological diseases with neurosurgery and medical genetic "__"__ ____________20___ Protocol №________ Head of department _______________ prof. Delva M.Yu. METHODICAL INSTRUCTIONS FOR THE INDEPENDENT WORK OF STUDENTS FOR PREPARATION TO PRACTICAL CLASSES AND DURING PRACTICAL CLASSES Academic subject Neurology The module № 1 General neurology Topic Syndromes of defeat oculomotor nerves. Pathology of olfactory and visual analyzers. Year of study IV Faculty Foreign Students Training (Medicine) Poltava 20___ 1.Relevance of the topic: the olfactory and visual analyzers play a role in receptor function of the nervous system. With the functions of these disorders analyzers, as well as with oculomotor disturbances faced by doctors of different specialties - neurologists, ophthalmologists, neurosurgeons, pediatricians, phthisiatricians, endocrinologists, internists. Violations of the functions of these analyzers is observed in a variety of inflammatory, demyelinating processes, tumors, trauma, endocrine disorders. The correct methodological approach to the study of functions, pathological changes of the olfactory and visual analyzers, oculomotor nerves makes it possible to deliver topical and clinical diagnosis and treatment in a timely manner. 2. Specific Objectives: To investigate the function of I, II, III, IV, VI pairs of cranial nerves, identify signs of a lesion of the nerve disorder Examine the identification functions -

Ehrlichiosis and Anaplasmosis Are Tick-Borne Diseases Caused by Obligate Anaplasmosis: Intracellular Bacteria in the Genera Ehrlichia and Anaplasma
Ehrlichiosis and Importance Ehrlichiosis and anaplasmosis are tick-borne diseases caused by obligate Anaplasmosis: intracellular bacteria in the genera Ehrlichia and Anaplasma. These organisms are widespread in nature; the reservoir hosts include numerous wild animals, as well as Zoonotic Species some domesticated species. For many years, Ehrlichia and Anaplasma species have been known to cause illness in pets and livestock. The consequences of exposure vary Canine Monocytic Ehrlichiosis, from asymptomatic infections to severe, potentially fatal illness. Some organisms Canine Hemorrhagic Fever, have also been recognized as human pathogens since the 1980s and 1990s. Tropical Canine Pancytopenia, Etiology Tracker Dog Disease, Ehrlichiosis and anaplasmosis are caused by members of the genera Ehrlichia Canine Tick Typhus, and Anaplasma, respectively. Both genera contain small, pleomorphic, Gram negative, Nairobi Bleeding Disorder, obligate intracellular organisms, and belong to the family Anaplasmataceae, order Canine Granulocytic Ehrlichiosis, Rickettsiales. They are classified as α-proteobacteria. A number of Ehrlichia and Canine Granulocytic Anaplasmosis, Anaplasma species affect animals. A limited number of these organisms have also Equine Granulocytic Ehrlichiosis, been identified in people. Equine Granulocytic Anaplasmosis, Recent changes in taxonomy can make the nomenclature of the Anaplasmataceae Tick-borne Fever, and their diseases somewhat confusing. At one time, ehrlichiosis was a group of Pasture Fever, diseases caused by organisms that mostly replicated in membrane-bound cytoplasmic Human Monocytic Ehrlichiosis, vacuoles of leukocytes, and belonged to the genus Ehrlichia, tribe Ehrlichieae and Human Granulocytic Anaplasmosis, family Rickettsiaceae. The names of the diseases were often based on the host Human Granulocytic Ehrlichiosis, species, together with type of leukocyte most often infected. -

Edema II, Clinical Significance
EDEMA II CLINICAL SIGNIFICANCE F. A. LeFEVRE, M.D., R. H. McDONALD, M.D., AND A. C. CORCORAN, M.D. It is the purpose of this paper to outline the clinical syndromes in which edema significantly appears, to discuss their differentiation, and to comment on the changes to which edema itself may give rise. The frequency with which edema occurs indicates the variety of its origins. Its physiologic bases have been reviewed in a former paper.1 Conditions in which edema commonly appears are summarized in Table 1. Although clinical edema usually involves more than one physiologic mechanism, it is not difficult to determine the predominant disturbance. Table 2 illustrates the physiologic mechanisms of clinical edema. Physiologically, edema is an excessive accumulation of interstitial fluid. Clinically, it may be latent or manifest, and, by its nature, localized or generalizing. These terms, with the exception of generalizing, have been defined, and may be accepted. By generalizing edema is meant a condi- tion in which edema is at first local in its appearance, but in which, as the process extends, edema will become general, causing anasarca. The degree of edema in any area is limited by tissue tension and the sites of its first appearance and later spread are partly determined by gravity. CARDIAC EDEMA Generalizing edema is an early manifestation of cardiac failure. It is usually considered to be evidence of inadequacy of the right ventricu- lar musculature (back pressure theory). Peripheral edema may be accompanied by pulmonary edema in cases where there is simultaneous left ventricular failure. Actually, the genesis of cardiac edema may depend more on sodium retention2,3'4 due to "forward cardiac failure" and renal constriction than on venous back pressure alone. -

Assessment Report
17 September 2020 EMA/522604/2020 Corr.1 Committee for Medicinal Products for Human Use (CHMP) Assessment report Velphoro Common name: sucroferric oxyhydroxide Procedure No. EMEA/H/C/002705/X/0020/G Note Assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us An agency of the European Union Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 © European Medicines Agency, 2021. Reproduction is authorised provided the source is acknowledged. Table of contents 1. Background information on the procedure .............................................. 6 1.1. Submission of the dossier ...................................................................................... 6 1.2. Steps taken for the assessment of the product ......................................................... 7 2. Scientific discussion ................................................................................ 8 2.1. Problem statement ............................................................................................... 8 2.1.1. Disease or condition ........................................................................................... 8 2.1.2. Epidemiology and risk factors, screening tools/prevention ...................................... 8 2.1.3. Biologic features ............................................................................................... -

Managing Hyponatremia in Patients with Syndrome of Inappropriate Antidiuretic Hormone Secretion
REVIEW Managing Hyponatremia in Patients With Syndrome of Inappropriate Antidiuretic Hormone Secretion Joseph G. Verbalis, MD Division of Endocrinology and Metabolism, Department of Medicine, Georgetown University Medical Center, Washington DC. J.G. Verbalis received an honorarium funded by an unrestricted educational grant from Otsuka America Pharmaceuticals, Inc., for time and expertise spent in the composition of this article. No editorial assistance was provided. No other conflicts exist. This review will address the management of hyponatremia caused by the syndrome of inappropriate antidiuretic hormone secretion (SIADH) in hospitalized patients. To do so requires an understanding of the pathogenesis and diagnosis of SIADH, as well as currently available treatment options. The review will be structured as responses to a series of questions, followed by a presentation of an algorithm for determining the most appropriate treatments for individual patients with SIADH based on their presenting symptoms. Journal of Hospital Medicine 2010;5:S18–S26. VC 2010 Society of Hospital Medicine. Why is SIADH Important to Hospitalists? What Causes Hyponatremia in Patients with SIADH? Disorders of body fluids, and particularly hyponatremia, are Hyponatremia can be caused by 1 of 2 potential disruptions among the most commonly encountered problems in clinical in fluid balance: dilution from retained water, or depletion medicine, affecting up to 30% of hospitalized patients. In a from electrolyte losses in excess of water. Dilutional hypo- study of 303,577 laboratory samples collected from 120,137 natremias are associated with either a normal (euvolemic) patients, the prevalence of hyponatremia (serum [Naþ] <135 or an increased (hypervolemic) extracellular fluid (ECF) vol- mmol/L) on initial presentation to a healthcare provider was ume, whereas depletional hyponatremias generally are asso- 28.2% among those treated in an acute hospital care setting, ciated with a decreased ECF volume (hypovolemic). -

Livedoid Vasculopathy Associated with Peripheral Neuropathy: a Report of Two Cases* Vasculopatia Livedoide Associada a Neuropatia Periférica: Relato De Dois Casos
CASE REPORT 227 s Livedoid vasculopathy associated with peripheral neuropathy: a report of two cases* Vasculopatia livedoide associada a neuropatia periférica: relato de dois casos Mariana Quirino Tubone1 Gabriela Fortes Escobar1 Juliano Peruzzo1 Pedro Schestatsky2 Gabriela Maldonado3 DOI: http://dx.doi.org/10.1590/abd1806-4841.20132363 Abstract: Livedoid vasculopathy (LV) is a chronic and recurrent disease consisting of livedo reticularis and sym- metric ulcerations, primarily located on the lower extremities, which heal slowly and leave an atrophic white scar ("atrophie blanche"). Neurological involvment is rare and presumed to be secondary to the ischemia from vascu- lar thrombosis of the vasa nervorum. Laboratory evaluation is needed to exclude secondary causes such as hyper- coagulable states, autoimmune disorders and neoplasms. We present two patients with a rare association of peripheral neuropathy and LV, thereby highlighting the importance of a multidisciplinary approach to reach the correct diagnosis. Keywords: Livedo reticularis; Mononeuropathies; Polyneuropathies; Skin diseases, vascular Resumo: Vasculopatia livedoide é uma doença crônica e recorrente caracterizada por livedo reticular e úlceras simétricas nos membros inferiores, que cicatrizam e deixam uma cicatriz branca atrófica ("atrophie blanche"). Envolvimento neurológico é raro e está provavelmente associado a isquemia pela trombose dos vasa nervorum. Avaliação laboratorial é indicada com o intuito de excluir causas secundárias como estados de hipercoagulabili- dade, doenças autoimunes e neoplasias. Apresentamos dois pacientes com uma rara associação de vasculopatia livedoide com neuropatia periférica, enfatizando a importância de uma abordagem multidisciplinar na busca do diagnóstico correto. Palavras-chave: Dermatopatias vasculares; Livedo reticular; Mononeuropatias; Polineuropatias INTRODUCTION Livedoid vasculopathy (LV) is a chronic and resentation of the dermo-hypodermic junction, was recurrent disease, usually restricted to the skin, and compatible with LV. -
From Confusion to Coma: a Catastrophic Deterioration
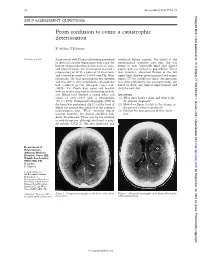
52 Postgrad Med J 2001;77:52–55 Postgrad Med J: first published as 10.1136/pmj.77.903.53a on 1 January 2001. Downloaded from SELF ASSESSMENT QUESTIONS From confusion to coma: a catastrophic deterioration K Ashkan, F Johnston Answers on p 56. A previously well 45 year old woman presented ventilated before transfer. On arrival at the to the local casualty department with a one day neurosurgical intensive care unit, she was history of generalised headache, neck stiVness, found to have bilaterally fixed and dilated and blurred vision. On examination she had a pupils, with no corneal or gag reflexes. There temperature of 38°C, a pulse of 80 beats/min, was, however, abnormal flexion of the left and a blood pressure of 130/80 mm Hg. Neu- upper limb. She was given mannitol and urgent rologically, she had spontaneous eye opening repeat CT was carried out (fig 2). An operation and was able to obey commands, although she was then performed, but postoperatively she had confused speech (Glasgow coma scale failed to show any clinical improvement and (GCS), 14). Pupils were equal and reactive died the next day. with no cranial or peripheral neurological defi- cits. Blood tests showed a raised white cell Questions count of 20.9 × 109/l with a neutrophilia (1) What does figure 1 show and what is the (19.2 × 109/l). Computed tomography (CT) of diVerential diagnosis? the brain was performed (fig 1), on the basis of (2) How does figure 2 relate to the change in which the patient was referred to the regional the patient’s clinical condition? neurosurgical unit. -

Cerebral Venous Thrombosis and Livedo Reticularis in a Case with MTHFR 677TT Homozygote
Journal of Clinical Neurology / Volume 2 / June, 2006 Case Report Cerebral Venous Thrombosis and Livedo Reticularis in a Case with MTHFR 677TT Homozygote Jee-Young Lee, M.D., Manho Kim, M.D., Ph.D. Department of Neurology, College of Medicine, Seoul National University, Seoul, Korea Hyperhomocysteinemia associated with methylene terahydrofolate reductase (MTHFR) mutation can be a risk factor for idiopathic cerebral venous thrombosis. We describe the first case of MTHFR 677TT homozygote with cerebral venous thrombosis and livedo reticularis. A 45-year-old man presented with seizures and mottled-like skin lesions, that were aggravated by cold temperature. Hemorrhagic infarct in the right frontoparietal area with superior sagittal sinus thrombosis was observed. He had hyperhomocysteinemia, low plasma folate level, and MTHFR 677TT homozygote genotype, which might be associated with livedo reticularis and increase the risk for cerebral venous thrombosis. J Clin Neurol 2(2):137-140, 2006 Key Words : Livedo reticularis, Methylene tetrahydrofolate reductase, Cerebral venous thrombosis Hyperhomocysteinemia causes vascular endothelial venous infarct due to cerebral venous thrombosis. damage that result in atherosclerosis and ischemic strokes.1 It is also associated with prothrombotic state or venous thromboembolism2 including cerebral venous CASE REPORT thrombosis.3 Among the thrombophilic factors with hyperhomocysteinemia, methylene tetrahydrofolate reduc- A 45 year-old man was brought to the emergency tase (MTHFR) mutant (C677 → T, homozygote) with room with uncontrolled seizures. Two days ago, sudden low plasma folate concentration increases the risk for paresthesia in left arm developed, which progressed to cerebral venous thrombosis.4 MTHFR 677TT is thermo- tonic posturing and leftward head version, followed by labile and sensitive to temperature alteration.5 a generalized tonic clonic seizure. -
Hypervitaminosis - an Emerging Pathological Condition
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Review Article Hypervitaminosis - An Emerging Pathological Condition J K Roop PG Department of Zoology, JC DAV College (Affiliated to Panjab University, Chandigarh), Dasuya-144205, District Hoshiarpur, Punjab, India ABSTRACT Vitamins are essential organic compounds that are required in small amounts to regulate various metabolic activities in the body. Prolonged and overconsumption of pharmaceutical forms of both water-soluble and fat-soluble vitamins may lead to toxicity and/or hypervitaminosis. Hypervitaminosis is an acute emerging pathological condition of the body due to excess accumulation of any of the vitamins. In case of acute poisoning with vitamin supplements/drugs, emergency assistance is required to detoxify the effects and restore the organization, structure and function of body’s tissues and organs. Sometimes death may occur due to intoxication to liver, kidney and heart. So, to manage any type of hypervitaminosis, proper diagnosis is essential to initiate eliminating the cause of its occurrence and accelerate the elimination of the supplement from the body. The present review discusses the symptoms of hypervitaminosis that seems to be a matter of concern today and management strategies to overcome toxicity or hypervitaminosis. Keywords: Hypervitaminosis, Toxicity, Vitamins, Vitamin pathology, Fat-soluble vitamin, Water- soluble vitamin. INTRODUCTION body, particularly in the liver. Vitamin B Vitamins are potent organic Complex and vitamin C are water- soluble. compounds present in small concentrations They are dissolved easily in food during in various fruits and vegetables. They cooking and a portion of these vitamins may regulate physiological functions and help in be destroyed by heating. -

Question of the Day Archives: Monday, December 5, 2016 Question: Calcium Oxalate Is a Widespread Toxin Found in Many Species of Plants
Question Of the Day Archives: Monday, December 5, 2016 Question: Calcium oxalate is a widespread toxin found in many species of plants. What is the needle shaped crystal containing calcium oxalate called and what is the compilation of these structures known as? Answer: The needle shaped plant-based crystals containing calcium oxalate are known as raphides. A compilation of raphides forms the structure known as an idioblast. (Lim CS et al. Atlas of select poisonous plants and mushrooms. 2016 Disease-a-Month 62(3):37-66) Friday, December 2, 2016 Question: Which oral chelating agent has been reported to cause transient increases in plasma ALT activity in some patients as well as rare instances of mucocutaneous skin reactions? Answer: Orally administered dimercaptosuccinic acid (DMSA) has been reported to cause transient increases in ALT activity as well as rare instances of mucocutaneous skin reactions. (Bradberry S et al. Use of oral dimercaptosuccinic acid (succimer) in adult patients with inorganic lead poisoning. 2009 Q J Med 102:721-732) Thursday, December 1, 2016 Question: What is Clioquinol and why was it withdrawn from the market during the 1970s? Answer: According to the cited reference, “Between the 1950s and 1970s Clioquinol was used to treat and prevent intestinal parasitic disease [intestinal amebiasis].” “In the early 1970s Clioquinol was withdrawn from the market as an oral agent due to an association with sub-acute myelo-optic neuropathy (SMON) in Japanese patients. SMON is a syndrome that involves sensory and motor disturbances in the lower limbs as well as visual changes that are due to symmetrical demyelination of the lateral and posterior funiculi of the spinal cord, optic nerve, and peripheral nerves. -

Assessing Acute Collapse for Presentation Powerpoint and Handouts
“I’ve Fallen and [email protected] I Can’t Get Up” Assessing Acute Collapse For Presentation PowerPoint and Handouts: http://wendyblount.com Wendy Blount, DVM Kinds of Shock [email protected] Anaphylactic Shock •Obstructed airway •Acute allergic reaction •Lung Disease •Mast Cell Tumor Degranulation •Pleural air or effusion Cardiovascular Shock Neurogenic shock •Arrhythmia •Forebrain and brainstem - For Presentation PowerPoint •Left Heart Failure decreased consciousness •Right Heart Failure •Spinal cord – flaccid paralysis and Handouts: •Pericardial Disease Septic Shock http://wendyblount.com Hypovolemic Shock •Overwhelming infection •Dehydration Traumatic Shock •Hemorrhage •Due to pain •Hypoproteinemia Toxic Shock Hypoxic Shock •Due to inflammatory mediators, •Anemia endogenous and exogenous •Hemoglobin Pathology toxins Collapse Other Than Shock Assessment of Inability or Unwillingness to get up Collapse Profound Weakness Ataxia – lack of coordination •Metabolic weakness •Vestibular ataxia Quick Assessment •Hypercalcemia •Cerebellar ataxia Life Saving Treatment •Hypokalemia •Sensory ataxia •Hypoglycemia Paresis - loss of voluntary Physical Exam •Neurotoxins motor Emergency Diagnostics •Polyneuropathy •Lower Motor Neuron •Junctionopathy •CNS Lesion at level of History •Myopathy paresis Pain •Flaccid paresis In House Diagnostics •Spinal Cord/Nerve Pain •Upper Motor Neuron •Orthopedic Pain •CNS Lesion above paresis •Muscular Pain •Spastic paresis 1 Assessment of Assessment of Collapse Collapse Quick Assessment Life Saving Treatment