A Breakthrough in Myopia Control for Your Child
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

7. Kansas Vision Screening Referral & Eye Care Professional Report
7. Kansas Vision Screening Referral & Eye Care Professional Report (Return completed report to school health clinic or nurse) Child’s Name: Date of Birth: Date of Referral: School: Grade: Met referral criteria (check applicable boxes): [ ] With Glasses/Contacts [ ] Without Correction [ ] Unable to Screen [ ] Based on Observation. Provide Symptoms/Concerns: [ ] Distance Visual Acuity [ ] R [ ] L Circle screening tool/distance: Sloan Chart, LEA Symbols, HOTV Symbols, Chart 5 or 10 feet [ ] Near Visual Acuity [ ] R [ ] L (or) if Near Binocular Testing [ ] Both [ ] Stereopsis (PASS 2) Instrument Screening (screener may attach instrument report): [ ] With Glasses/Contacts [ ] Without Correction Circle Instrument (WA Spot™ / Plusoptix S12C / WA SureSight 2.25) Met referral criteria: [ ] R [ ] L Eye Care Professional Findngs Date of Exam:____________ Without Correction With Current Prescription With New Prescription [ ] Normal R_______ L_______ R_______ L_______ R_______ L_______ Summary of vision problem & diagnosis: [ ] Hyperopia: Indicate eye R_______ L_______ [ ] Myopia: Indicate eye? R_______ L_______ [ ] Astigmatism: Indicate eye R_______ L_______ [ ] Amblyopia: Indicate eye R_______ L_______ [ ] Eye Alignment: Indicate eye? R_______ L_______ Esophoria / Esotropia / Exophoria / Exotropia / Other [ ] Binocularity (Stereovision, Near Point of Convergence): ______________________________ [ ] Other Ocular Conditions or Neurological/ Cortical Vision Impairment – Explain: Recommendations & Treatment: Glasses Prescribed: [ ] No [ ] Yes [ ] Constant -

Eyeglasses Product Narrative
Increasing Access to Eyeglasses in Low- and Middle-Income Countries PRODUCT NARRATIVE: EYEGLASSES aatscale2030.orgtscale2030.org MARCH 2020 ACKNOWLEDGEMENTS This report was delivered by the Clinton Health Access Initiative under the AT2030 programme in support of the ATscale Strategy. The AT2030 programme is funded by UK aid from the UK government and led by the Global Disability Innovation (GDI) Hub. The authors wish to acknowledge and thank vision sector experts, practitioners and users, and the partners from the AT2030 programme and Founding Partners of ATscale, the Global Partnership for Assistive Technology, for their contributions. The ATscale Founding Partners are: China Disabled Persons’ Federation, Clinton Health Access Initiative, GDI Hub, Government of Kenya, International Disability Alliance, Norwegian Agency for Development Cooperation, Office of the UN Secretary-General’s Envoy for Financing the Health Millennium Development Goals and for Malaria, UK Department for International Development, UNICEF, United States Agency for International Development, World Health Organization. The views and opinions expressed within this report are those of the authors and do not necessarily reflect the official policies or position of ATscale Founding Partners, partners of the AT2030 programme, or funders. Please use the following form (https://forms.gle/QVVKAbYMG73UVeFB8) to register any comments or questions about the content of this document. Please direct any questions about ATscale, the Global Partnership for Assistive Technology, to [email protected] or visit atscale2030.org. To learn more about the AT2030 Programme, please visit a https://at2030.org/. II PRODUCT NARRATIVE: EYEGLASSES TABLE OF CONTENTS Acronyms iii Executive Summary 1 Introduction 3 1. Assistive Technology and Market Shaping 3 2. -

FAQ: Cataracts
Don’t lose sight of Cataracts Information for people at risk What is cataract? 1 When the lens of your eye gets cloudy, it is called a cataract. It can cause vision loss in one or both eyes. It cannot spread from one eye to the other. What causes a cataract? 2 The lenses of the eyes are made mostly of water and protein. As we age, some of this protein may clump together and cloud the lenses of our eyes. Over time, this “cloud” may grow and cover more of the lens. This makes it harder to see. Smoking, alcohol use, diabetes, and prolonged exposure to the sun can also cause cataract. When are you most likely to have a cataract? 3 Older people mostly get cataracts. But people in their 40s and 50s may get them, especially if the eye has been injured. The risk of having a cataract increases after age 60, and by age 80, more than half of all Americans will have a cataract or will have had cataract surgery. Normal vision. What are the symptoms of a cataract? A scene as it might be viewed by a 4 When you first get a cataract, you may not notice much person with a cataract. change. Your vision may become blurry, as if looking through a foggy window. Or colors may not appear as bright as they once did. As the “cloud” over the lens of your eye grows, it may be harder for you to read. You may also see more glare from a lamp or car headlights at night. -
A Virtual Try-On System for Prescription Eyeglasses
Feature Article A Virtual Try-On System for Prescription Eyeglasses Qian Zhang and Yu Guo ■ Nanyang Technological University Pierre-Yves Laffont, Tobias Martin, and Markus Gross ■ ETH Zurich ision-correcting eyeglasses have improved We present a system for virtually trying on pre- the lives of millions of people. Eyeglasses scription eyeglasses. Our system acts as a virtual significantly affect the wearer’s appear- mirror, allowing users to try on a variety of eye- Vance, and the selection of new pairs of eyeglasses is glasses with corrective lenses based on their pre- largely based on how the glasses look when wearers scription (see Figure 2). We use an image sequence try them on. However, an often overlooked fact is of the user without eyeglasses as input, along with that corrective lenses introduce distortion caused the user’s eyeglasses prescription and a 3D model by the refraction effect. As Figure 1 illustrates, the of the desired eyeglasses frame. Our system gen- eyes of a person wearing correc- erates a 3D representation of the corrective lenses tive lenses for nearsightedness mounted into the eyeglasses frame and modifies the Corrective lenses introduce appear smaller compared with video sequence to virtually insert the eyeglasses us- distortion caused by the wearing nonprescription lenses, ing image-based rendering. This approach simulates refraction effect, which whereas the eyes of a person the distortion introduced by the prescription lenses changes the wearer’s wearing lenses for farsightedness and gives users a better idea of how they would look appearance. To give users a appear larger. when wearing the new pair of eyeglasses. -

Finding an Eye Care Professional
Finding an Eye Care Professional You may have recently had your vision screened and failed the screening, you may have noticed changes in your vision, or you may be at risk for developing glaucoma or diabetic retinopathy. Even if you are not experiencing vision problems, it is important to get regular eye exams. If you are thinking about seeing an eye care professional, but don’t know where to begin, this fact sheet can help. Referrals are often helpful in choosing an eye care professional. Ask trusted friends or contact a hospital or university with a medical school for names and references. You can also call one of the following organizations for a referral to someone in your area. The following are the definitions given by each professional organization with their contact information. Ophthalmologists Definition provided by the American Academy of Ophthalmology. For more information, contact the AAO at (415) 561-8540 or www.aao.org. A physician (doctor of medicine or doctor of osteopathy) who specializes in the refractive, medical and surgical care of the eyes and visual system and in the prevention of eye disease and injury. The ophthalmologist has completed four or more years of college premedical education, four or more years of medical school, and four or more years of residency, including at least three years of residency in ophthalmology. The ophthalmologist is a specialist who is qualified by lengthy medical education, training, and experience to diagnose, treat, and manage all eye and visual system problems and is licensed by a state regulatory board to practice medicine and surgery. -

Intraocular Lenses and Spectacle Correction
MEDICAL POLICY POLICY TITLE INTRAOCULAR LENSES, SPECTACLE CORRECTION AND IRIS PROSTHESIS POLICY NUMBER MP-6.058 Original Issue Date (Created): 6/2/2020 Most Recent Review Date (Revised): 6/9/2020 Effective Date: 2/1/2021 POLICY PRODUCT VARIATIONS DESCRIPTION/BACKGROUND RATIONALE DEFINITIONS BENEFIT VARIATIONS DISCLAIMER CODING INFORMATION REFERENCES POLICY HISTORY I. POLICY Intraocular Lens Implant (IOL) Initial IOL Implant A standard monofocal intraocular lens (IOL) implant is medically necessary when the eye’s natural lens is absent including the following: Following cataract extraction Trauma to the eye which has damaged the lens Congenital cataract Congenital aphakia Lens subluxation/displacement A standard monofocal intraocular lens (IOL) implant is medically necessary for anisometropia of 3 diopters or greater, and uncorrectable vision with the use of glasses or contact lenses. Premium intraocular lens implants including but not limited to the following are not medically necessary for any indication, including aphakia, because each is intended to reduce the need for reading glasses. Presbyopia correcting IOL (e.g., Array® Model SA40, ReZoom™, AcrySof® ReStor®, TECNIS® Multifocal IOL, Tecnis Symfony and Tecnis SymfonyToric, TRULIGN, Toric IO, Crystalens Aspheric Optic™) Astigmatism correcting IOL (e.g., AcrySof IQ Toric IOL (Alcon) and Tecnis Toric Aspheric IOL) Phakic IOL (e.g., ARTISAN®, STAAR Visian ICL™) Replacement IOLs MEDICAL POLICY POLICY TITLE INTRAOCULAR LENSES, SPECTACLE CORRECTION AND IRIS PROSTHESIS POLICY NUMBER -

Types of Contact Lenses and Their Characteristics1
3 ■ Types of Contact Lenses and Their Characteristics1 The basic categories of contact lenses currently acetate butyrate [CAB], PMMA-silicone, and in use are the original hard (polymethylmethacry- silicone). There are variations within each group, late [PMMA]) lenses, soft hydrogels (hydro- but their respective properties are similar enough xymethylmethacrylate [HEMA] and other mate- to consider them as essentially the same type of rials), and gas-permeable hard lenses (cellulose lenses. HARD PMMA LENSES As discussed in the previous chapter, hard rial and safe for use in the eye. It can be molded PMMA lenses were the first lenses introduced or lathed into lenses with a high degree of preci- onto the market, and corneal PMMA lenses simi- sion. Once made, PMMA lenses can be reworked lar to those currently in use have been available and modified to customize them to an individual’s since the early 1950s. Compared to later types of requirements. The result is a safe lens of excellent lenses, PMMA lenses can be difficult to adapt to, visual properties which very closely conforms to and perhaps as many as half of the people fitted patient requirements. PMMA lenses require min- do not become long-term wearers. Since PMMA imal use of cleaning, soaking, and wetting solu- is not water- or gas-permeable, wearers must rely tions. They may be tinted to reduce excessive light on the “tear pump” action of the eye to provide sensitivity, to make them easier to find when oxygen to the covered portion of the cornea. As dropped, or for appearance reasons. They are the wearer blinks, tear interchange occurs from durable, can be renewed by polishing away mi- outside the lens to beneath it, providing the nec- nor surface scratches, and often last 5 to 7 years essary oxygen. -

Lenses and Optics
PHYS 1400: Physical Science for General Education Laboratory Manual LENSES AND OPTICS INTRODUCTION If you (or your cat) wear glasses or contact lenses, you are already familiar with the science of optics. Whether you realize it or not, you understand the idea of a focal point. You are very aware when an image is out of focus (no glasses) or in focus (put your glasses back on). You even know the difference between a real and a virtual image, although you have probably never said to yourself, “I wish that the real image formed by the lens in my eye was better focused on my retina!” Or may be you have. OBJECTIVES ๏ Identify the differences between concave and convex lenses ๏ Use the lens equation to Steampunk Cat is equipped for any ocular emergency. determine the focal length of a convex lens Convex lenses are converging lenses. ๏ Construct ray diagrams to accurately show how an image is formed Concave lenses are diverging lenses. ๏ Demonstrate the difference between a near– and far–sighted eye, and show how each vision problem can be corrected ACTIVITY 1: CONVERGING AND DIVERGING LENSES ๏ Use the converging and diverging lenses to observe objects around the room. ๏ Try to use both as magnifying glasses to enlarge text. ๏ While observing a single object, move the lens toward and away from your eye. Do this for both types of lens. ๏ Try observing objects using various combinations of lenses: two converging, two diverging, one of each. QUESTIONS 1. Which type of lens can you use to magnify text? What happens to the magnified image as you draw the lens farther from the text? 2. -

Page 1 of 8 Questions and Answers from the “Year of Children's Vision
Questions and Answers from the “Year of Children’s Vision: Developing a Strong Vision Health System (Part I)” Webinar (Presented February 26, 2014) QUESTION: I don't feel comfortable not referring for vision screening at 20/33 or greater but the acuity numbers for referral were quoted as 20/40 (ages 3-5). ANSWER: The referral guidelines example in the Webinar from the American Academy of Pediatrics, the American Association for Pediatric Ophthalmology and Strabismus, the American Academy of Ophthalmology, and the American Association of Certified Orthoptists state that children ages 3 through 5 years should be rescreened or referred if they cannot identify the majority (3 of 5) of optotypes on the 20/40 line. Children ages 6 years and older should be rescreened or referred if they cannot pass the majority of optotypes on the 20/30 (20/32) line. Some states, for example, Massachusetts, do have 20/32 as a referral line for ages 3, 4, and 5. QUESTION: Is there a preference to refer to an ophthalmologist as opposed to an optometrist especially for younger children never have been screened before? ANSWER: We do not have a preference. You want to refer to a pediatric eye care professional (optometrist or ophthalmologist) with training and experience treating young children. QUESTION: Why would we get charged for direct referral? We don’t have many choices in our area who take Medicaid. ANSWER: If a child is entitled to an eye examination to identify a disability, to determine eligibility for special education services, to develop an Individualized Education Program (IEP), or as a related service under the IEP, the eye exam must occur at no cost to the family. -

Primal Contact Lenses Care Instructions and Waiver Page 1 PRIMAL CONTACTS
PRIMAL CONTACTS - Soft (Hydrophilic) Contact Lenses Eye Care Instructions IMPORTANT: Please read carefully and keep this information for future use. Primal Brand Contacts Lenses are available as corrective and non-corrective lens designs. The Lenses are composed of 62% Polymacon and 38% water a silicone-containing hydrogel. PRIMAL (NON-CORRECTIVE) CONTACT LENSES PARAMETERS Diameter : 14,0 mm to 14,8 mm Base Curve : 8,6 mm to 8,8 mm Power : Plano INDICATIONS (USES) AND WEARING RESTRICTIONS Primal ® Brand Fashion Lenses is indicated for non-corrective use in the colour enhancement of the iris and have no therapeutic effects for daily wear. CONTRAINDICATIONS (REASONS NOT TO USE PRIMAL BRAND CONTACT LENSES) Inflammation or infection in or around the eye or eyelids. Any eye disease, injury, or abnormality that affects the cornea, conjunctiva, or eyelids. Any previously diagnosed condition that makes contact lens wear uncomfortable. Any systemic disease that may affect the eye or be exaggerated by wearing contact lenses. Allergic reactions of ocular surfaces of the eye (adnexa) that may be induced or exaggerated by wearing contact lenses or use of contact lens solutions. Allergy to any ingredient, such as mercury or Thimerosal, in a solution which is to be used to care for your contact lenses. Severe dry eye. Any active corneal infection (bacterial, fungal, protozoal or viral). Not to be used if you are unable to follow the lens care regimen or unable to obtain assistance to do so. POTENTIAL ADVERSE SIDE EFFECTS FROM WEARING PRIMAL BRAND CONTACT LENSES Stinging, burning, itching (irritation), pain, tearing or other eye discomfort or sensation of foreign object in the eye. -
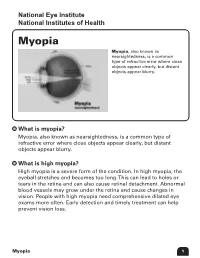
Myopia Myopia, Also Known As Nearsightedness, Is a Common Type of Refractive Error Where Close Objects Appear Clearly, but Distant Objects Appear Blurry
National Eye Institute Eye Institute National Institutes Institutes of Health of Health Myopia Myopia, also known as nearsightedness, is a common type of refractive error where close objects appear clearly, but distant objects appear blurry. What is myopia? Myopia, also known as nearsightedness, is a common type of refractive error where close objects appear clearly, but distant objects appear blurry. What is high myopia? High myopia is a severe form of the condition. In high myopia, the eyeball stretches and becomes too long. This can lead to holes or tears in the retina and can also cause retinal detachment. Abnormal blood vessels may grow under the retina and cause changes in vision. People with high myopia need comprehensive dilated eye exams more often. Early detection and timely treatment can help prevent vision loss. Myopia 1 What is refraction? Refraction is the bending of light as it passes through one object to another. Vision occurs when light rays are bent (refracted) as they pass through the cornea and the lens. The light is then focused on the retina. The retina converts the light-rays into messages that are sent through the optic nerve to the brain. The brain interprets these messages into the images we see. What are refractive errors? In refractive errors, the shape of the eye prevents light from focusing on the retina. The length of the eyeball (longer or shorter), changes in the shape of the cornea, or aging of the lens can cause refractive errors. How does myopia develop? Myopia develops in eyes that focus images in front of the retina instead of on the retina, which results in blurred vision. -
Speaker's Guide
Speaker’s Guide Living With Low Vision: What you should know Slide 1 Presenter Instructions: • Introduce yourself to the group. • Tell your audience how long the presentation will last. • Engage the audience by asking them to introduce themselves and to name one thing they would like to learn from this presentation. Talking Points: • The purpose of this presentation is to provide information about low vision, what can be done about it, and where to get more information. • After attending this presentation, you will be able to do the following: ❍❍ Identify signs that may signal vision loss. ❍❍ Define low vision and vision rehabilitation. ❍❍ Outline what you can do if you have low vision. ❍❍ List questions that are good to ask an eye care professional and/or specialist in low vision. Living With Low Vision Speaker’s Guide 1 7/14 Slide 2 Talking Point: • Many changes to vision are normal and common as you age. But losing vision or going blind is not a normal part of aging. Living With Low Vision Speaker’s Guide 7/14 Slide 3 Talking Points: • As we get older, our eyes and vision change. Some of these normal changes include: ❍❍ Losing the ability to focus, which makes it harder to perform tasks such as reading, writing, playing cards, and working on the computer. ❍❍ Noticing declining contrast and color sensitivity, making it harder to distinguish colors such as blue and black or distinguish where an object ends and its background begins. ❍❍ Needing more light to see well and more time to adjust to changing levels of light.