Pleural Effusion: Benign and Malignant
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Pneumothorax Ex Vacuo in a Patient with Malignant Pleural Effusion After Pleurx Catheter Placement
The Medicine Forum Volume 16 Article 20 2015 Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 Thomas Jefferson University, [email protected] Loheetha Ragupathi, MD Thomas Jefferson University, [email protected] Follow this and additional works at: https://jdc.jefferson.edu/tmf Part of the Medicine and Health Sciences Commons Let us know how access to this document benefits ouy Recommended Citation Bhardwaj, MS4, Meera and Ragupathi, MD, Loheetha (2015) "Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement," The Medicine Forum: Vol. 16 , Article 20. DOI: https://doi.org/10.29046/TMF.016.1.019 Available at: https://jdc.jefferson.edu/tmf/vol16/iss1/20 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in The Medicine Forum by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Bhardwaj, MS4 and Ragupathi, MD: Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 and Loheetha Ragupathi, MD INTRODUCTION Pneumothorax ex vacuo (“without vaccuum”) is a type of pneumothorax that can develop in patients with large pleural effusions. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
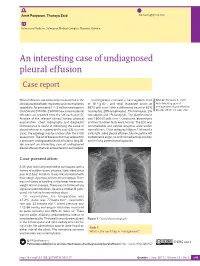
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Allergic Bronchopulmonary Aspergillosis: a Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2
Review Allergy Asthma Immunol Res. 2016 July;8(4):282-297. http://dx.doi.org/10.4168/aair.2016.8.4.282 pISSN 2092-7355 • eISSN 2092-7363 Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India 2Department of Respiratory Medicine, Mata Chanan Devi Hospital, New Delhi, India This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. In susceptible individuals, inhalation of Aspergillus spores can affect the respiratory tract in many ways. These spores get trapped in the viscid spu- tum of asthmatic subjects which triggers a cascade of inflammatory reactions that can result in Aspergillus-induced asthma, allergic bronchopulmo- nary aspergillosis (ABPA), and allergic Aspergillus sinusitis (AAS). An immunologically mediated disease, ABPA, occurs predominantly in patients with asthma and cystic fibrosis (CF). A set of criteria, which is still evolving, is required for diagnosis. Imaging plays a compelling role in the diagno- sis and monitoring of the disease. Demonstration of central bronchiectasis with normal tapering bronchi is still considered pathognomonic in pa- tients without CF. Elevated serum IgE levels and Aspergillus-specific IgE and/or IgG are also vital for the diagnosis. Mucoid impaction occurring in the paranasal sinuses results in AAS, which also requires a set of diagnostic criteria. Demonstration of fungal elements in sinus material is the hall- mark of AAS. -

The Spectrum of Computed Tomography Appearances
RESPIRATORY MEDICIXE (1997) 91, 213-219 Allergic bronchopulmonary aspergillosis: the spectrum of computed tomography appearances N. PANCHAL",R. BHAGAT",C. PANT+AND A. SHAH" “Department of Clinical Research, Vallabhbhai Pate1 Chest Institute, University of Delhi, Delhi, lndia ‘Imaging Division, Institute of Nuclear Medicine and Allied Sciences, Timaupuv, Delhi, India Although computed tomography (CT) of the thorax has been compared to plain chest radiography and bronchography for demonstration of central bronchiectasis (CB) in allergic bronchopulmonary aspergil- losis (ABPA), the CT presentation of the disease is yet to be highlighted. With this in view, the CT appearances in 23 patients with ABPA were evaluated. The scans were assessed for bronchial, parenchymal and pleural abnormalities. Central bronchiectasis was identified in all patients, involving 114 (85%) of the 134 lobes and 210 (52%) of the 406 segments studied. Other bronchial abnormalities such as dilated and totally occluded bronchi (11 patients), air-fluid levels within dilated bronchi (five patients), bronchial wall thickening (10 patients) and parallel-line shadows (seven patients) were also observed. Parenchymal abnormalities, which had a predilection for upper lobes, included consolidation in 10 (43%) patients, collapse in four (17%) patients and parenchymal scarring in 19 (83%) patients. A total of six cavities were seen in three (13%) patients, and an emphysematous bullae was detected in one (4%) patient. The pleura was involved in 10 (43%) patients. Ipsilateral pleural effusion with collapse was observed in one patient, while in nine other patients, parenchymal lesions extended up to the pleura. Concomitant allergic Aspergillus sinusitis (AAS) was also detected in three (13%) of the 23 patients. -

Case Report Cryptogenic Organising Pneumonia: Clinical, Pathological, and Prognostic Analysis of 27 Cases
Int J Clin Exp Med 2016;9(3):6911-6919 www.ijcem.com /ISSN:1940-5901/IJCEM0019752 Case Report Cryptogenic organising pneumonia: clinical, pathological, and prognostic analysis of 27 cases Yanli Li1*, Yan Li1*, Fengfeng Han1, Haiyang Yu1, Tianyun Yang1, Huimin Li2, Wenbin Guan3, Xuejun Guo1 Departments of 1Respiratory Medicine, 2Radiology, Xin Hua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, China; 3Department of Pathology, Xinhua Hospital, School of Medicine, Shanghai Jiaotong University, China. *Equal contributors and co-first authors. Received November 14, 2015; Accepted November 29, 2015; Epub March 15, 2016; Published March 30, 2016 Abstract: Background: Buds of granulation tissue within the lumen of distal pulmonary airspaces characterises organising pneumonia (OP). This study aimed to analyse the clinical and pathological features and prognosis of pa- tients with cryptogenic OP. Methods: Twenty-seven patients were retrospectively analysed. A multidisciplinary team (a clinician, radiologist, and pathologist) diagnosed all patients. Clinical features, laboratory data, chest radiology, treatment and prognosis, pulmonary function, and haematoxylin-eosin and immunohistochemical staining were assessed. Results: Symptoms (in decreasing prevalence) were cough, dyspnoea, fever, and chest tightness. The erythrocyte sedimentation rate (in most patients) and C-reactive protein level were increased. Radiologic findings (in decreasing prevalence) were consolidation, nodules, and band-like opacities. The lung function results were ‘normal’ and ‘restrictive’ in 30.8% and 38.5% of patients, respectively. Most patients responded to corticosteroids. The prognosis of the patients was excellent in 77.8% and poor in 22.2%. Organised polypoid granulation inflamma- tory tissue was in the distal bronchiole airways, respiratory bronchioles, alveolar ducts, and alveoli. -

Cryptogenic Organizing Pneumonia: Evolution of Morphological Patterns Assessed by HRCT
diagnostics Article Cryptogenic Organizing Pneumonia: Evolution of Morphological Patterns Assessed by HRCT Francesco Tiralongo 1,* , Monica Palermo 1, Giulio Distefano 1 , Ada Vancheri 2, Gianluca Sambataro 2,3 , Sebastiano Emanuele Torrisi 2, Federica Galioto 1, Agata Ferlito 1, Giulia Fazio 1, Pietro Valerio Foti 1, Letizia Antonella Mauro 1, Carlo Vancheri 2, Stefano Palmucci 1 and Antonio Basile 1 1 Radiology Unit 1, Department of Medical Surgical Sciences and Advanced Technologies “GF Ingrassia”—University Hospital “Policlinico-Vittorio Emanuele”, University of Catania, 95123 Catania, Italy; [email protected] (M.P.); [email protected] (G.D.); [email protected] (F.G.); [email protected] (A.F.); [email protected] (G.F.); [email protected] (P.V.F.); [email protected] (L.A.M.); [email protected] (S.P.); [email protected] (A.B.) 2 Regional Referral Centre for Rare Lung Diseases, A. O. U. “Policlinico-Vittorio Emanuele” Dept. of Clinical and Experimental Medicine, University of Catania, 95123 Catania, Italy; [email protected] (A.V.); [email protected] (G.S.); [email protected] (S.E.T.); [email protected] (C.V.) 3 Artroreuma S.R.L., Outpatient of Rheumatology associated with the National Health System, Corso S. Vito 53, 95030 Mascalucia (Catania), Italy * Correspondence: [email protected] Received: 14 April 2020; Accepted: 28 April 2020; Published: 29 April 2020 Abstract: To evaluate the radiological findings in patients with cryptogenic organizing pneumonia (COP) before steroid treatment and their behavior after therapy, we retrospectively evaluated a total of 22 patients with a diagnosis of COP made by bronchoalveolar lavage (BAL), biopsy or clinical/radiological features, and the patients were followed between 2014 and 2018 at the hospital; the demographic data, symptoms, radiologic findings, diagnostic methods and treatment plans of patients were collected from patients’ hospital records. -

Allergic Bronchopulmonary Aspergillosis: a Clinical Review of 24 Patients: Are We Right in Frequent Serologic Monitoring?
[Downloaded free from http://www.thoracicmedicine.org on Sunday, March 22, 2015, IP: 41.36.247.20] || Click here to download free Android application for this journal Original Article Allergic bronchopulmonary aspergillosis: A clinical review of 24 patients: Are we right in frequent serologic monitoring? Subramanian Natarajan, Poonam Subramanian1 Department of Abstract: Pulmonary Medicine, BACKGROUND: Allergic Broncho Pulmonary Aspergillosis (ABPA) is a rare disease characterized by an allergic Dhanwantary Hospital, infl ammatory response to the colonization by aspergillus or other fungi in the airways. The aim was to study the Mumbai, 1Pulmonary clinical, radiological, and serological characteristics of patients of ABPA. Medicine, The Lung MATERIALS AND METHODS: A prospective observational study of patients with breathlessness, chronic cough, Centre, Mumbai, blood eosinophilia, and infi ltrates on chest X-ray were evaluated with serologic and allergic skin fungal tests using Maharashtra, India 15 common fungal antigens. Total of 24 patients were diagnosed as ABPA. RESULTS: Total 24 patients, 15 males (62%), 9 females (38%). Age range: 14-70 years, mean 49.13, standard Address for deviation (SD) 14.12. Central bronchiectasis — sixteen patients, bronchocoele — one patient, consolidation — correspondence: fi ve patients, collapse with mucous plugging with areas of consolidation — three patients, one patient had Dr. Subramanian bronchiectasis, consolidation with hemorrhagic pleural effusion. Fifty-eight percent of patients had received Natarajan, anti-tuberculosis medications prior to diagnosis. Serum total IgE varied from 340 to 18100 IU/mL. Two patients Department of Pulmonary had IgE levels below 1,000 IU/mL. The mean decrease in Serum total IgE levels at the end of 1 month was Medicine, Dhanwantary 26.1% (range: 0.7-71.9%) and at the end of 2 months was 58.9% (range: 11.11-93.26%) (P value of 0.004). -

Original Article Role of Pleural Fluid Attenuation Values on CT for Hemothorax Diagnosis in Trauma Patients
Int J Clin Exp Med 2018;11(8):8430-8437 www.ijcem.com /ISSN:1940-5901/IJCEM0068790 Original Article Role of pleural fluid attenuation values on CT for hemothorax diagnosis in trauma patients Esin Akgul Kalkan1, Nilüfer Aylanç2 Departments of 1Forensic Medicine, 2Radiology, Faculty of Medicine, Canakkale Onsekiz Mart University, Canakkale, Turkey Received November 8, 2017; Accepted June 3, 2018; Epub August 15, 2018; Published August 30, 2018 Abstract: Background and aim: Hemothorax is a critical issue in patients with chest trauma. It should be diagnosed quickly and accurately. The study’s aim was to define the potential role of pleural fluid (PF) attenuation value deter- mined on computerized tomography (CT) for the diagnosis of traumatic hemothorax. Methods: From 01.07.2011 to 01.07.2016, patients with PF detected on CT with tube thoracostomy were reviewed. On CT sections, PF attenuation values taken from levels where pleural fluid had the most intense appearance were measured as Hounsfield Units (HU). The relationship between HU values and chest traumatic findings, macroscopic discharge diagnosis, peripher- al blood Hb and Htc levels and CT protocol were investigated. Results: Thirty-eight cases were reviewed in the study group. All PF HU values were determined to be more than 20.0 HU. PF attenuation values were more than 35 HU in 71.1% (n:27) of the cases and between 20.0 and 34.9 for 28.9% (n:11). In the subgroup with hemorrhagic fluid drained from the thoracic cavity, HU values were often higher than 35. For the sub-groups with and without coexist- ing traumatic findings, there was no statistically significant difference in terms of PF density being below or above 35 HU. -

Pulmonary Infarction Due to Pulmonary Embolism
SYMPTOMS TO DIAGNOSIS GREGORY W. RUTECKI, MD, Section Editor MELDA SONMEZ, MD LOUTFI S. ABOUSSOUAN, MD CAROL FARVER, MD Medical Student, Koc University Department of Pulmonary, Allergy, and Critical Care Department of Pathology, Cleveland Clinic; Professor of School of Medicine, Istanbul, Turkey Medicine, Cleveland Clinic; Associate Professor of Medicine, Pathology, Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western of Case Western Reserve University, Cleveland, OH Reserve University, Cleveland, OH SUDISH C. MURTHY, MD, PhD ROOP KAW, MD Department of Thoracic and Cardiovascular Departments of Hospital Medicine and Outcomes Research Surgery, Cleveland Clinic; Professor of Surgery, Anesthesiology, Cleveland Clinic; Associate Professor of Cleveland Clinic Lerner College of Medicine of Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH Case Western University, Cleveland, OH Pulmonary infarction due to pulmonary embolism 76-year-old man whose history included □ It is rarely, if ever, associated with A abdominal aortic aneurysm repair, bilat- pulmonary embolism eral femoral artery bypass for popliteal artery □ Most patients with pleural effusion due to aneurysm, hypertension, and peptic ulcer pulmonary embolism do not have disease was admitted to a community hospi- pleuritic chest pain tal with pleuritic chest pain and shortness of □ Pulmonary embolism should be excluded breath. Two days earlier, he had undergone in all cases of pleural effusion without a repair of a ventral hernia. clear cause At the time of that admission, he reported Pulmonary embolism should be excluded in no fever, chills, night sweats, cough, or his- all cases of pleural effusion that do not have tory of heart or lung disease. -

Concurrent Allergic Bronchopulmonary Aspergillosis and Aspergilloma: Is It a More Severe Form of the Disease?
Eur Respir Rev 2010; 19: 118, 261–263 DOI: 10.1183/09059180.00009010 CopyrightßERS 2010 EDITORIAL Concurrent allergic bronchopulmonary aspergillosis and aspergilloma: is it a more severe form of the disease? A. Shah he mould Aspergillus, a genus of spore forming fungi, lung diseases in which aspergilloma formation has been affects the respiratory system in more ways than one. reported include sarcoidosis [15], hydatidosis [16], pneumato- T The clinical spectrum of Aspergillus involvement of the coele caused by Pneumocystis pneumonia [17], bronchiectasis, lungs ranges from various hypersensitivity manifestations to emphysematous bullae, and sites of prior lobectomies or invasive disease which can be fatal. The inhaled spores hardly pneumonectomies. The time required for the development of affect healthy persons but in asthmatic subjects these spores fungal balls ranges from a few months to more than 10 yrs [18]. are trapped in the viscid secretions found in the airways. Repeated inhalation of Aspergillus antigens triggers allergic The clinical categories of Aspergillus-related respiratory disor- reactions in atopic individuals, which may manifest as ders, for reasons unknown, usually remain mutually exclusive. Aspergillus-induced asthma, allergic bronchopulmonary asper- In spite of similar immunopathological responses, concomitant gillosis (ABPA) and allergic Aspergillus sinusitis (AAS) [1]. occurrence of ABPA and AAS is infrequently reported [19–22]. Saprobic colonisation of airways, cavities and necrotic tissue In this issue of the European Respiratory Review,MONTANI et al. leads to the development of aspergillomas. [23] describe a 50-yr-old female with concomitant ABPA and aspergilloma. Even though chronic lung damage appears to Although ABPA is predominantly a disease of asthmatics, only provide a favourable milieu for aspergilloma formation, the a few asthmatics actually suffer from it. -

Pleural Effusion a Medford, N Maskell
702 Postgrad Med J: first published as 10.1136/pgmj.2005.035352 on 4 November 2005. Downloaded from REVIEW Pleural effusion A Medford, N Maskell ............................................................................................................................... Postgrad Med J 2005;81:702–710. doi: 10.1136/pgmj.2005.035352 Pleural disease remains a commonly encountered clinical fluid may be helpful diagnostically and should always be recorded in the medical notes. A problem for both general physicians and chest specialists. pleural:serum packed cell volume .0.5 shows a This review focuses on the investigation of undiagnosed haemothorax with ,1% being not significant.3 pleural effusions and the management of malignant and parapneumonic effusions. New developments in this area Exudate compared with transudates Classically, exudates having a protein level are also discussed at the end of the review. It aims to be .30 g/l and transudates ,30 g/l. Light’s criteria evidence based together with some practical suggestions will enable differentiation more accurately when for practising clinicians. the pleural protein is unhelpful (box 2).4 Occasionally, Light’s criteria will label an effu- ........................................................................... sion in a patient with left ventricular failure taking diuretics an exudate in which case clinical leural effusions are a common medical judgement is required. problem and a significant source of morbid- ity. There is wide variation in management P Differential cell counts despite their significant prevalence, partly because of the relative lack of randomised Differential cell counting adds little diagnostic controlled trials in this area. This review con- information. Pleural lymphocytosis is common in siders: malignant and tuberculous effusions but can also be attributable to rheumatoid disease, N The approach to the investigation of the lymphoma, sarcoidosis, and chylothorax.5 undiagnosed pleural effusion.