Concurrent Allergic Bronchopulmonary Aspergillosis and Aspergilloma: Is It a More Severe Form of the Disease?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Rapid and Precise Diagnosis of Pneumonia Coinfected By
Rapid and precise diagnosis of pneumonia coinfected by Pneumocystis jirovecii and Aspergillus fumigatus assisted by next-generation sequencing in a patient with systemic lupus erythematosus: a case report Yili Chen Sun Yat-Sen University Lu Ai Sun Yat-Sen University Yingqun Zhou First Peoples Hospital of Nanning Yating Zhao Sun Yat-Sen University Jianyu Huang Sun Yat-Sen University Wen Tang Sun Yat-Sen University Yujian Liang ( [email protected] ) Sun Yat-Sen University Case report Keywords: Pneumocystis jirovecii, Aspergillus fumigatus, Next generation sequencing, Case report Posted Date: March 19th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-154016/v2 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/12 Abstract Background: Pneumocystis jirovecii and Aspergillus fumigatus, are opportunistic pathogenic fungus that has a major impact on mortality in patients with systemic lupus erythematosus. With the potential to invade multiple organs, early and accurate diagnosis is essential to the survival of SLE patients, establishing an early diagnosis of the infection, especially coinfection by Pneumocystis jirovecii and Aspergillus fumigatus, still remains a great challenge. Case presentation: In this case, we reported that the application of next -generation sequencing in diagnosing Pneumocystis jirovecii and Aspergillus fumigatus coinfection in a Chinese girl with systemic lupus erythematosus (SLE). Voriconazole was used to treat pulmonary aspergillosis, besides sulfamethoxazole and trimethoprim (SMZ-TMP), and caspofungin acetate to treat Pneumocystis jirovecii infection for 6 days. On Day 10 of admission, her chest radiograph displayed obvious absorption of bilateral lung inammation though the circumstance of repeated fever had not improved. -

Rhinitis and Sinusitis
Glendale Animal Hospital 623-934-7243 www.familyvet.com Rhinitis and Sinusitis (Inflammation of the Nose and Sinuses) Basics OVERVIEW Rhinitis—inflammation of the lining of the nose Sinusitis—inflammation of the sinuses The nasal cavity communicates directly with the sinuses; thus inflammation of the nose (rhinitis) and inflammation of the sinuses (sinusitis) often occur together (known as “rhinosinusitis”) “Upper respiratory tract” (also known as the “upper airways”) includes the nose, nasal passages, throat (pharynx), and windpipe (trachea) “Lower respiratory tract” (also known as the “lower airways”) includes the bronchi, bronchioles, and alveoli (the terminal portion of the airways, in which oxygen and carbon dioxide are exchanged) SIGNALMENT/DESCRIPTION OF PET Species Dogs Cats Breed Predilections Short-nosed, flat-faced (known as “brachycephalic”) cats are more prone to long-term (chronic) inflammation of the nose (rhinitis), and possibly fungal rhinitis Dogs with a long head and nose (known as “dolichocephalic dogs,” such as the collie and Afghan hound) are more prone to Aspergillus (a type of fungus) infection and nasal tumors Mean Age and Range Cats—sudden (acute) viral inflammation of the nose and sinuses (rhinosinusitis) and red masses in the nasal cavity and throat (known as “nasopharyngeal polyps”) are more common in young kittens (6–12 weeks of age) Congenital (present at birth) diseases (such as cleft palate) are more common in young pets Tumors/cancer and dental disease—are more common in older pets Foreign -

Legionnaires' Disease
epi TRENDS A Monthly Bulletin on Epidemiology and Public Health Practice in Washington Legionnaires’ disease Vol. 22 No. 11 Legionellosis is a bacterial respiratory infection which can result in severe pneumonia and death. Most cases are sporadic but legionellosis is an important public health issue because outbreaks can occur in hotels, communities, healthcare facilities, and other settings. Legionellosis Legionellosis was first recognized in 1976 when an outbreak affected 11.17 more than 200 people and caused more than 30 deaths, mainly among attendees of a Legionnaires’ convention being held at a Philadelphia hotel. Legionellosis is caused by numerous different Legionella species and serogroups but most epiTRENDS P.O. Box 47812 recognized infections are due to Olympia, WA 98504-7812 L. pneumophila serogroup 1. The extent to which this is due to John Wiesman, DrPH, MPH testing bias is unclear since only Secretary of Health L. pneumophila serogroup 1 is Kathy Lofy, MD identified via commonly used State Health Officer urine antigen tests; other species Scott Lindquist, MD, MPH Legionella pneumophila multiplying and serogroups must be identified in a human lung cell State Epidemiologist, through PCR or culture, tests Communicable Disease www.cdc.gov which are less commonly ordered. Jerrod Davis, P.E. Assistant Secretary The disease involves two clinically distinct syndromes: Pontiac fever, Disease Control and Health Statistics a self-limited flu-like illness without pneumonia; and Legionnaires’ disease, a potentially fatal pneumonia with initial symptoms of fever, Sherryl Terletter Managing Editor cough, myalgias, malaise, and sometimes diarrhea progressing to symptoms of pneumonia which can be severe. Health conditions that Marcia J. -

Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1
ISSN: 2572-4193 Gelpi et al. J Otolaryngol Rhinol 2018, 4:036 DOI: 10.23937/2572-4193.1510036 Volume 4 | Issue 1 Journal of Open Access Otolaryngology and Rhinology CASE REPORT Rhinotillexomania in a Cystic Fibrosis Patient Resulting in Septal Perforation Mark Gelpi1*, Emily N Ahadizadeh1,2, Brian D’Anzaa1 and Kenneth Rodriguez1 1 Check for University Hospitals Cleveland Medical Center, USA updates 2Case Western Reserve University School of Medicine, USA *Corresponding author: Mark Gelpi, MD, University Hospitals Cleveland Medical Center, 11100 Euclid Avenue, Cleveland, OH 44106, USA, Tel: (216)-844-8433, Fax: (216)-201-4479, E-mail: [email protected] paranasal sinuses [1,4]. Nasal symptoms in CF patients Abstract occur early, manifesting between 5-14 years of age, and Cystic fibrosis (CF) is a multisystem disease that can have represent a life-long problem in this population [5]. Pa- significant sinonasal manifestations. Viscous secretions are one of several factors in CF that result in chronic sinona- tients with CF can develop thick nasal secretions con- sal pathology, such as sinusitis, polyposis, congestion, and tributing to chronic rhinosinusitis (CRS), nasal conges- obstructive crusting. Persistent discomfort and nasal man- tion, nasal polyposis, headaches, and hyposmia [6-8]. ifestations of this disease significantly affect quality of life. Sinonasal symptoms of CF are managed medically with Digital manipulation and removal of crusting by the patient in an attempt to alleviate the discomfort can have unfore- topical agents and antibiotics, however surgery can be seen damaging consequences. We present one such case warranted due to the chronic and refractory nature of and investigate other cases of septal damage secondary to the symptoms, with 20-25% of CF patients undergoing digital trauma, as well as discuss the importance of sinona- sinus surgery in their lifetime [8]. -

Pneumothorax Ex Vacuo in a Patient with Malignant Pleural Effusion After Pleurx Catheter Placement
The Medicine Forum Volume 16 Article 20 2015 Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 Thomas Jefferson University, [email protected] Loheetha Ragupathi, MD Thomas Jefferson University, [email protected] Follow this and additional works at: https://jdc.jefferson.edu/tmf Part of the Medicine and Health Sciences Commons Let us know how access to this document benefits ouy Recommended Citation Bhardwaj, MS4, Meera and Ragupathi, MD, Loheetha (2015) "Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement," The Medicine Forum: Vol. 16 , Article 20. DOI: https://doi.org/10.29046/TMF.016.1.019 Available at: https://jdc.jefferson.edu/tmf/vol16/iss1/20 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in The Medicine Forum by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Bhardwaj, MS4 and Ragupathi, MD: Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 and Loheetha Ragupathi, MD INTRODUCTION Pneumothorax ex vacuo (“without vaccuum”) is a type of pneumothorax that can develop in patients with large pleural effusions. -

FINAL RISK ASSESSMENT for Aspergillus Niger (February 1997)
ATTACHMENT I--FINAL RISK ASSESSMENT FOR Aspergillus niger (February 1997) I. INTRODUCTION Aspergillus niger is a member of the genus Aspergillus which includes a set of fungi that are generally considered asexual, although perfect forms (forms that reproduce sexually) have been found. Aspergilli are ubiquitous in nature. They are geographically widely distributed, and have been observed in a broad range of habitats because they can colonize a wide variety of substrates. A. niger is commonly found as a saprophyte growing on dead leaves, stored grain, compost piles, and other decaying vegetation. The spores are widespread, and are often associated with organic materials and soil. History of Commercial Use and Products Subject to TSCA Jurisdiction The primary uses of A. niger are for the production of enzymes and organic acids by fermentation. While the foods, for which some of the enzymes may be used in preparation, are not subject to TSCA, these enzymes may have multiple uses, many of which are not regulated except under TSCA. Fermentations to produce these enzymes may be carried out in vessels as large as 100,000 liters (Finkelstein et al., 1989). A. niger is also used to produce organic acids such as citric acid and gluconic acid. The history of safe use for A. niger comes primarily from its use in the food industry for the production of many enzymes such as a-amylase, amyloglucosidase, cellulases, lactase, invertase, pectinases, and acid proteases (Bennett, 1985a; Ward, 1989). In addition, the annual production of citric acid by fermentation is now approximately 350,000 tons, using either A. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
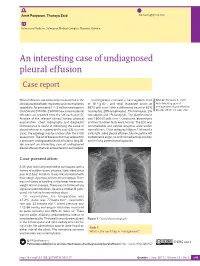
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Pneumonia: Prevention and Care at Home
FACT SHEET FOR PATIENTS AND FAMILIES Pneumonia: Prevention and Care at Home What is it? On an x-ray, pneumonia usually shows up as Pneumonia is an infection of the lungs. The infection white areas in the affected part of your lung(s). causes the small air sacs in your lungs (called alveoli) to swell and fill up with fluid or pus. This makes it harder for you to breathe, and usually causes coughing and other symptoms that sap your energy and appetite. How common and serious is it? Pneumonia is fairly common in the United States, affecting about 4 million people a year. Although for many people infection can be mild, about 1 out of every 5 people with pneumonia needs to be in the heart hospital. Pneumonia is most serious in these people: • Young children (ages 2 years and younger) • Older adults (ages 65 and older) • People with chronic illnesses such as diabetes What are the symptoms? and heart disease Pneumonia symptoms range in severity, and often • People with lung diseases such as asthma, mimic the symptoms of a bad cold or the flu: cystic fibrosis, or emphysema • Fatigue (feeling tired and weak) • People with weakened immune systems • Cough, without or without mucus • Smokers and heavy drinkers • Fever over 100ºF or 37.8ºC If you’ve been diagnosed with pneumonia, you should • Chills, sweats, or body aches take it seriously and follow your doctor’s advice. If your • Shortness of breath doctor decides you need to be in the hospital, you will receive more information on what to expect with • Chest pain or pain with breathing hospital care. -

Outcome and Prognostic Factors of Pneumocystis Jirovecii Pneumonia
Gaborit et al. Ann. Intensive Care (2019) 9:131 https://doi.org/10.1186/s13613-019-0604-x RESEARCH Open Access Outcome and prognostic factors of Pneumocystis jirovecii pneumonia in immunocompromised adults: a prospective observational study Benjamin Jean Gaborit1,6* , Benoit Tessoulin2, Rose‑Anne Lavergne3, Florent Morio3, Christine Sagan4, Emmanuel Canet5, Raphael Lecomte1, Paul Leturnier1, Colin Deschanvres1, Lydie Khatchatourian1, Nathalie Asseray1, Charlotte Garret5, Michael Vourch5, Delphine Marest5, François Raf1, David Boutoille1,6 and Jean Reignier5 Abstract Background: Pneumocystis jirovecii pneumonia (PJP) remains a severe disease associated with high rates of invasive mechanical ventilation (MV) and mortality. The objectives of this study were to assess early risk factors for severe PJP and 90‑day mortality, including the broncho‑alveolar lavage fuid cytology profles at diagnosis. Methods: We prospectively enrolled all patients meeting pre‑defned diagnostic criteria for PJP admitted at Nantes university hospital, France, from January 2012 to January 2017. Diagnostic criteria for PJP were typical clinical features with microbiological confrmation of P. jirovecii cysts by direct examination or a positive specifc quantitative real‑time polymerase chain reaction (PCR) assay. Severe PJP was defned as hypoxemic acute respiratory failure requiring high‑ fow nasal oxygen with at least 50% FiO2, non‑invasive ventilation, or MV. Results: Of 2446 respiratory samples investigated during the study period, 514 from 430 patients were positive for P. jirovecii. Of these 430 patients, 107 met criteria for PJP and were included in the study, 53 (49.5%) patients had severe PJP, including 30 who required MV. All patients were immunocompromised with haematological malignancy ranking frst (n 37, 35%), followed by solid organ transplantation (n 27, 25%), HIV‑infection (n 21, 20%), systemic diseases (n 13,= 12%), solid tumors (n 12, 11%) and primary immunodefciency= (n 6, 8%). -

Pneumocystis Pneumonia: Immunity, Vaccines, and Treatments
pathogens Review Pneumocystis Pneumonia: Immunity, Vaccines, and Treatments Aaron D. Gingerich 1,2, Karen A. Norris 1,2 and Jarrod J. Mousa 1,2,* 1 Center for Vaccines and Immunology, College of Veterinary Medicine, University of Georgia, Athens, GA 30602, USA; [email protected] (A.D.G.); [email protected] (K.A.N.) 2 Department of Infectious Diseases, College of Veterinary Medicine, University of Georgia, Athens, GA 30602, USA * Correspondence: [email protected] Abstract: For individuals who are immunocompromised, the opportunistic fungal pathogen Pneumocystis jirovecii is capable of causing life-threatening pneumonia as the causative agent of Pneumocystis pneumonia (PCP). PCP remains an acquired immunodeficiency disease (AIDS)-defining illness in the era of antiretroviral therapy. In addition, a rise in non-human immunodeficiency virus (HIV)-associated PCP has been observed due to increased usage of immunosuppressive and im- munomodulating therapies. With the persistence of HIV-related PCP cases and associated morbidity and mortality, as well as difficult to diagnose non-HIV-related PCP cases, an improvement over current treatment and prevention standards is warranted. Current therapeutic strategies have pri- marily focused on the administration of trimethoprim-sulfamethoxazole, which is effective at disease prevention. However, current treatments are inadequate for treatment of PCP and prevention of PCP-related death, as evidenced by consistently high mortality rates for those hospitalized with PCP. There are no vaccines in clinical trials for the prevention of PCP, and significant obstacles exist that have slowed development, including host range specificity, and the inability to culture Pneumocystis spp. in vitro. In this review, we overview the immune response to Pneumocystis spp., and discuss current progress on novel vaccines and therapies currently in the preclinical and clinical pipeline. -

Crohn's Disease-Associated Interstitial Lung Disease Mimicking Sarcoidosis
Case report SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES 2016; 33; 288-291 © Mattioli 1885 Crohn’s disease-associated interstitial lung disease mimicking sarcoidosis: a case report and review of the literature Choua Thao1, A Amir Lagstein2, T Tadashi Allen3, Huseyin Erhan Dincer4, Hyun Joo Kim4 1Department of Internal Medicine, University of Nevada School of Medicine Las Vegas, Las Vegas, NV; 2Department of Pathology, Univer- sity of Michigan, Ann Arbor, MI; 3Department of Radiology, University of Minnesota, Minneapolis, MN; 4 Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, University of Minnesota, Minneapolis, MN Abstract. Respiratory involvement in Crohn’s disease (CD) is a rare manifestation known to involve the large and small airways, lung parenchyma, and pleura. The clinical presentation is nonspecific, and diagnostic tests can mimic other pulmonary diseases, posing a diagnostic challenge and delay in treatment. We report a case of a 60-year-old female with a history of CD and psoriatic arthritis who presented with dyspnea, fever, and cough with abnormal radiological findings. Diagnostic testing revealed an elevated CD4:CD8 ratio in the bronchoal- veolar lavage fluid, and cryoprobe lung biopsy results showed non-necrotizing granulomatous inflammation. We describe here the second reported case of pulmonary involvement mimicking sarcoidosis in Crohn’s disease and a review of the literature on the approaches to making a diagnosis of CD-associated interstitial lung disease. (Sarcoidosis Vasc Diffuse Lung Dis 2016; 33: 288-291) Key words: interstitial lung disease, Crohns disease, sarcoidosis, cryoprobe lung biopsy Introduction Moreover, certain diagnostic tests such as bronchoal- veolar lavage (BAL) cell analysis and tissue biopsy Pulmonary involvement in Crohn’s disease (CD) results may mimic other granulomatous lung diseas- is relatively rare and can be difficult to diagnose.