Differential Diagnosis of Pleural Effusions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Guidelines on the Diagnosis and Management of Pericardial
European Heart Journal (2004) Ã, 1–28 ESC Guidelines Guidelines on the Diagnosis and Management of Pericardial Diseases Full Text The Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology Task Force members, Bernhard Maisch, Chairperson* (Germany), Petar M. Seferovic (Serbia and Montenegro), Arsen D. Ristic (Serbia and Montenegro), Raimund Erbel (Germany), Reiner Rienmuller€ (Austria), Yehuda Adler (Israel), Witold Z. Tomkowski (Poland), Gaetano Thiene (Italy), Magdi H. Yacoub (UK) ESC Committee for Practice Guidelines (CPG), Silvia G. Priori (Chairperson) (Italy), Maria Angeles Alonso Garcia (Spain), Jean-Jacques Blanc (France), Andrzej Budaj (Poland), Martin Cowie (UK), Veronica Dean (France), Jaap Deckers (The Netherlands), Enrique Fernandez Burgos (Spain), John Lekakis (Greece), Bertil Lindahl (Sweden), Gianfranco Mazzotta (Italy), Joa~o Morais (Portugal), Ali Oto (Turkey), Otto A. Smiseth (Norway) Document Reviewers, Gianfranco Mazzotta, CPG Review Coordinator (Italy), Jean Acar (France), Eloisa Arbustini (Italy), Anton E. Becker (The Netherlands), Giacomo Chiaranda (Italy), Yonathan Hasin (Israel), Rolf Jenni (Switzerland), Werner Klein (Austria), Irene Lang (Austria), Thomas F. Luscher€ (Switzerland), Fausto J. Pinto (Portugal), Ralph Shabetai (USA), Maarten L. Simoons (The Netherlands), Jordi Soler Soler (Spain), David H. Spodick (USA) Table of contents Constrictive pericarditis . 9 Pericardial cysts . 13 Preamble . 2 Specific forms of pericarditis . 13 Introduction. 2 Viral pericarditis . 13 Aetiology and classification of pericardial disease. 2 Bacterial pericarditis . 14 Pericardial syndromes . ..................... 2 Tuberculous pericarditis . 14 Congenital defects of the pericardium . 2 Pericarditis in renal failure . 16 Acute pericarditis . 2 Autoreactive pericarditis and pericardial Chronic pericarditis . 6 involvement in systemic autoimmune Recurrent pericarditis . 6 diseases . 16 Pericardial effusion and cardiac tamponade . -

Hepatic Hydrothorax Without Apparent Ascites and Dyspnea - a Case Report
Case Report DOI: 10.7860/JCDR/2018/37185.12181 I nternal Medicine Hepatic Hydrothorax without Apparent S ection Ascites and Dyspnea - A Case Report JING HE1, RASHA HAYKAL2, HONGCHUAN COVILLE3, JAYA PRAKASH GADIKOTA4, CHRISTOPHER BRAY5 ABSTRACT A 78-year-old female with a past medical history of alcoholic cirrhosis was hospitalised with recurrent lower gastrointestinal bleeding due to rectal ulcers. The ulcers were successfully treated with cautery and placement of clips. However, a recurrent large right-sided pleural effusion without apparent ascites and dyspnea were found incidentally during the hospitalisation. The initial fluid analysis was exudate based on Light’s criteria with high protein. The fluid analysis was repeated five days later, after rapid reaccumulation which revealed transudates. Other causes of pleural effusion like heart failure, renal failure or primary pulmonary diseases were excluded. Hepatic hydrothorax was considered and the patient was started with the treatment of Furosemide and Spironolactone. The atypical presentation of hepatic hydrothorax may disguise the diagnosis and delay the treatment. Therefore, for a patient with recurrent, unexplained unilateral pleural effusions, even with atypical fluid characterisation and in the absence of ascites, hepatic hydrothorax should still remain on the top differential with underlying cirrhosis to ensure optimal treatment. Keywords: Cirrhosis, Light criteria, Liver, Pleural effusion CASE REPORT Haemogram Levels Normal range A 78-year-old Caucasian female, with a past medical history of alcoholic cirrhosis, admitted for recurrent rectal bleeding secondary WBC 6.9 (4.5-11.0 thousands/mm3) to rectal ulcers and was successfully treated with cautery and Neutrophils % 78 H (50.0-75.0 %) placement of clips. -

Albumin in Health and Disease: Protein Metabolism and Function*
Article #2 CE An In-Depth Look: ALBUMIN IN HEALTH AND DISEASE Albumin in Health and Disease: Protein Metabolism and Function* Juliene L. Throop, VMD Marie E. Kerl, DVM, DACVIM (Small Animal Internal Medicine), DACVECC Leah A. Cohn, DVM, PhD, DACVIM (Small Animal Internal Medicine) University of Missouri-Columbia ABSTRACT: Albumin is a highly charged, 69,000 D protein with a similar amino acid sequence among many veterinary species. Albumin is the major contributor to colloid oncotic pressure and also serves as an important carrier protein. Its ability to modulate coagulation by preventing pathologic platelet aggrega- tion and augmenting antithrombin III is important in diseases that result in moderately to severely decreased serum albumin levels. Synthesis is primar- ily influenced by oncotic pressure, but inflammation, hormone status, and nutrition impact the synthetic rate as well. Albumin degradation is a poorly understood process that does not appear to be selective for older mole- cules.The clinical consequences of hypoalbuminemia reflect the varied func- tions of the ubiquitous albumin protein molecule. he albumin molecule has several characteristics that make it a unique protein. Most veterinarians are aware of the importance of this molecule in maintain- Ting colloid oncotic pressure, but albumin has many other less commonly recog- nized functions as well. The clinical consequences of hypoalbuminemia are reflections of the many functions albumin fulfills. Understanding the functions, synthesis, and *A companion article on degradation of the albumin molecule can improve understanding of the causes, conse- causes and treatment of quences, and treatment of hypoalbuminemia. hypoalbuminemia appears on page 940. STRUCTURE Email comments/questions to Albumin has a molecular weight of approximately 69,000 D, with minor variations [email protected], among species. -

Renal Sodium Handling in Minimal Change Nephrotic Syndrome
Arch Dis Child: first published as 10.1136/adc.59.9.825 on 1 September 1984. Downloaded from Archives of Disease in Childhood, 1984, 59, 825-830 Renal sodium handling in minimal change nephrotic syndrome A-B BOHLIN AND U BERG Department of Paediatrics, Karolinska Institute, Huddinge Hospital, Stockholm, Sweden SUMMARY Renal sodium handling was studied in 23 children at three different stages of the minimal change nephrotic syndrome-the oedema forming state, proteinuric steady state, and remission. Clearances of inulin and para-aminohippuric acid and urinary sodium excretion were determined basally, after intravenous infusion of isotonic saline and hyperoncotic albumin, and after furosemide injection. Absolute and fractional basal sodium excretion were significantly lower in oedema forming patients than in proteinuric patients in steady state, and non-proteinuric patients. In contrast to proteinuric patients in steady state and non-proteinuric patients, the oedema forming patients failed to respond to isotonic saline infusion with increased sodium excretion. After diuretic blockade with furosemide, the fractional sodium excretion of the oedema forming patients increased to values no different from those of the non-proteinuric patients, whereas the fractional sodium excretion of the steady state patients increased to significantly higher values. The plasma aldosterone concentration was within normal limits in 11 of 14 proteinuric patients, and did not correlate with the basal sodium excretion. Thus, sodium copyright. retention in the minimal change nephrotic syndrome was found only in oedema forming patients, and since this is not related to the plasma aldosterone concentration it may be caused by an intrarenal mechanism, probably sited in distal parts of the nephron. -

Pneumothorax Ex Vacuo in a Patient with Malignant Pleural Effusion After Pleurx Catheter Placement
The Medicine Forum Volume 16 Article 20 2015 Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 Thomas Jefferson University, [email protected] Loheetha Ragupathi, MD Thomas Jefferson University, [email protected] Follow this and additional works at: https://jdc.jefferson.edu/tmf Part of the Medicine and Health Sciences Commons Let us know how access to this document benefits ouy Recommended Citation Bhardwaj, MS4, Meera and Ragupathi, MD, Loheetha (2015) "Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement," The Medicine Forum: Vol. 16 , Article 20. DOI: https://doi.org/10.29046/TMF.016.1.019 Available at: https://jdc.jefferson.edu/tmf/vol16/iss1/20 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in The Medicine Forum by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Bhardwaj, MS4 and Ragupathi, MD: Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 and Loheetha Ragupathi, MD INTRODUCTION Pneumothorax ex vacuo (“without vaccuum”) is a type of pneumothorax that can develop in patients with large pleural effusions. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
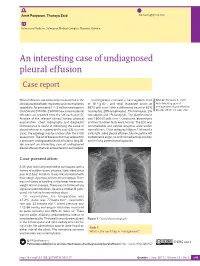
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Determinants of Glomerular Filtration in Experimental Glomerulonephritis in the Rat
Determinants of glomerular filtration in experimental glomerulonephritis in the rat. D A Maddox, … , T M Daugharty, B M Brenner J Clin Invest. 1975;55(2):305-318. https://doi.org/10.1172/JCI107934. Research Article Pressures and flows were measured in surface glomerular capillaries, efferent arterioles, and proximal tubules of 22 Wistar rats in the early autologous phase of nephrotoxic serum nephritis (NSN). Linear deposits of rabbit and rat IgG and C3 component of complement were demonstrated in glomerular capillary walls by immunofluorescence microscopy. Light microscopy revealed diffuse proliferative glomerulonephritis, and proteinuria was present. Although whole kidney and single nephron glomerular filtration rate (GFR) in NSN (0.8 plus or minus 0.04 SE2 ml/min and 2 plus or minus 2 nl/min, respectively) remained unchanged from values in 16 weight-matched NORMAL HYDROPENIC control rats (0.8 plus or minus 0.08 and 28 plus or minus 2), important alterations in glomerular dynamics were noted. Mean transcapillary hydraulic pressure difference (deltaP) averaged 41 plus or minus 1 mm Hg in NSN versus 32 plus or minus 1 in controls (P LESS THAN 0.005). Oncotic pressures at the afferent (piA) end of the glomerular capillary were similar in both groups ( 16 mm /g) but increased much less by the efferent end (piE) in NSN (to 29 plus or minus 1 mm Hg) than in controls (33 plus or minus 1, P less than 0.025). Hence, equality between deltaP and piE, denoting filtration pressure equilibrium, obtained in control but not in NSN rats. While glomerular plasma flow rate was slightly higher […] Find the latest version: https://jci.me/107934/pdf Determinants of Glomerular Filtration in Experimental Glomerulonephritis in the Rat D. -

Glomerulonephritis Management in General Practice
Renal disease • THEME Glomerulonephritis Management in general practice Nicole M Isbel MBBS, FRACP, is Consultant Nephrologist, Princess Alexandra lomerular disease remains an important cause Hospital, Brisbane, BACKGROUND Glomerulonephritis (GN) is an G and Senior Lecturer in important cause of both acute and chronic kidney of renal impairment (and is the commonest cause Medicine, University disease, however the diagnosis can be difficult of end stage kidney disease [ESKD] in Australia).1 of Queensland. nikky_ due to the variability of presenting features. Early diagnosis is essential as intervention can make [email protected] a significant impact on improving patient outcomes. OBJECTIVE This article aims to develop However, presentation can be variable – from indolent a structured approach to the investigation of patients with markers of kidney disease, and and asymptomatic to explosive with rapid loss of kidney promote the recognition of patients who need function. Pathology may be localised to the kidney or further assessment. Consideration is given to the part of a systemic illness. Therefore diagnosis involves importance of general measures required in the a systematic approach using a combination of clinical care of patients with GN. features, directed laboratory and radiological testing, DISCUSSION Glomerulonephritis is not an and in many (but not all) cases, a kidney biopsy to everyday presentation, however recognition establish the histological diagnosis. Management of and appropriate management is important to glomerulonephritis (GN) involves specific therapies prevent loss of kidney function. Disease specific directed at the underlying, often immunological cause treatment of GN may require specialist care, of the disease and more general strategies aimed at however much of the management involves delaying progression of kidney impairment. -

Glomerular Filtration I DR.CHARUSHILA RUKADIKAR Assistant Professor Physiology GFR 1
Glomerular filtration I DR.CHARUSHILA RUKADIKAR Assistant Professor Physiology GFR 1. Definition 2. Normal value 3. Variation 4. Calculation (different pressures acting on glomerular membrane) 5. Factors affecting GFR 6. Regulation of GFR 7. Measurement of GFR QUESTIONS LONG QUESTION 1. GFR 2. RENIN ANGIOTENSIN SYSTEM SHORT NOTE 1. DYNAMICS OF GFR 2. FILTRATION FRACTION 3. ANGIOTENSIN II 4. FACTORS AFFECTING GLOMERULAR FILTRATION RATE 5. REGULATION OF GFR 6. RENAL CLEARANCE TEST 7. MEASUREMENT OF GFR Collecting duct epithelium P Cells – Tall, predominant, have few organelles, Na reabsorption & vasopressin stimulated water reabsorption I cells- CT and DCT, less, having more cell organelles, Acid secretion and HCO3 transport CHARACTERISTICS OF RENAL BLOOD FLOW 600-1200 ml/min (high) AV O2 difference low (1.5 mL/dL) During exercise increases 1.5 times Low basal tone, not altered in denervated / innervated kidney VO2 in kidneys is directly proportional to RBF, Na reabsorption & GFR Not homogenous flow, cortex more & medulla less Vasa recta hairpin bend like structure, hyperosmolarity inner medulla Transplanted kidney- cortical blood flow show autoregulation & medullary blood flow don’t show autoregulation, so no TGF mechanism Neurogenic vasodilation not exist 20% of resting cardiac output, while the two kidneys make < 0.5% of total body weight. Excretory function rather than its metabolic requirement. Remarkable constancy due to autoregulation. Processes concerned with urine formation. 1. Glomerular filtration, 2. Tubular reabsorption and 3. Tubular secretion. • Filtration Fluid is squeezed out of glomerular capillary bed • Reabsorption Most nutrients, water and essential ions are returned to blood of peritubular capillaries • Secretion Moves additional undesirable molecules into tubule from blood of peritubular capillaries Glomerular filtration Glomerular filtration refers to process of ultrafiltration of plasma from glomerular capillaries into the Bowman’s capsule. -

Assessing Acute Collapse for Presentation Powerpoint and Handouts
“I’ve Fallen and [email protected] I Can’t Get Up” Assessing Acute Collapse For Presentation PowerPoint and Handouts: http://wendyblount.com Wendy Blount, DVM Kinds of Shock [email protected] Anaphylactic Shock •Obstructed airway •Acute allergic reaction •Lung Disease •Mast Cell Tumor Degranulation •Pleural air or effusion Cardiovascular Shock Neurogenic shock •Arrhythmia •Forebrain and brainstem - For Presentation PowerPoint •Left Heart Failure decreased consciousness •Right Heart Failure •Spinal cord – flaccid paralysis and Handouts: •Pericardial Disease Septic Shock http://wendyblount.com Hypovolemic Shock •Overwhelming infection •Dehydration Traumatic Shock •Hemorrhage •Due to pain •Hypoproteinemia Toxic Shock Hypoxic Shock •Due to inflammatory mediators, •Anemia endogenous and exogenous •Hemoglobin Pathology toxins Collapse Other Than Shock Assessment of Inability or Unwillingness to get up Collapse Profound Weakness Ataxia – lack of coordination •Metabolic weakness •Vestibular ataxia Quick Assessment •Hypercalcemia •Cerebellar ataxia Life Saving Treatment •Hypokalemia •Sensory ataxia •Hypoglycemia Paresis - loss of voluntary Physical Exam •Neurotoxins motor Emergency Diagnostics •Polyneuropathy •Lower Motor Neuron •Junctionopathy •CNS Lesion at level of History •Myopathy paresis Pain •Flaccid paresis In House Diagnostics •Spinal Cord/Nerve Pain •Upper Motor Neuron •Orthopedic Pain •CNS Lesion above paresis •Muscular Pain •Spastic paresis 1 Assessment of Assessment of Collapse Collapse Quick Assessment Life Saving Treatment -

Allergic Bronchopulmonary Aspergillosis: a Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2
Review Allergy Asthma Immunol Res. 2016 July;8(4):282-297. http://dx.doi.org/10.4168/aair.2016.8.4.282 pISSN 2092-7355 • eISSN 2092-7363 Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India 2Department of Respiratory Medicine, Mata Chanan Devi Hospital, New Delhi, India This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. In susceptible individuals, inhalation of Aspergillus spores can affect the respiratory tract in many ways. These spores get trapped in the viscid spu- tum of asthmatic subjects which triggers a cascade of inflammatory reactions that can result in Aspergillus-induced asthma, allergic bronchopulmo- nary aspergillosis (ABPA), and allergic Aspergillus sinusitis (AAS). An immunologically mediated disease, ABPA, occurs predominantly in patients with asthma and cystic fibrosis (CF). A set of criteria, which is still evolving, is required for diagnosis. Imaging plays a compelling role in the diagno- sis and monitoring of the disease. Demonstration of central bronchiectasis with normal tapering bronchi is still considered pathognomonic in pa- tients without CF. Elevated serum IgE levels and Aspergillus-specific IgE and/or IgG are also vital for the diagnosis. Mucoid impaction occurring in the paranasal sinuses results in AAS, which also requires a set of diagnostic criteria. Demonstration of fungal elements in sinus material is the hall- mark of AAS.