Pamo Year 3 Work Plan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Zambia 30 September 2017
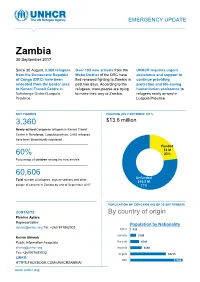
EMERGENCY UPDATE Zambia 30 September 2017 Since 30 August, 3,360 refugees Over 100 new arrivals from the UNHCR requires urgent from the Democratic Republic Moba District of the DRC have assistance and support to of Congo (DRC) have been fled renewed fighting to Zambia in continue providing relocated from the border area past two days. According to the protection and life-saving to Kenani Transit Centre in refugees, more people are trying humanitarian assistance to Nchelenge District/Luapula to make their way to Zambia. refugees newly arrived in Province. Luapula Province. KEY FIGURES FUNDING (AS 2 OCTOBER 2017) 3,360 $13.6 million requested for Zambia operation Newly-arrived Congolese refugees in Kenani Transit Centre in Nchelenge, Luapula province. 2,063 refugees have been biometrically registered Funded $3 M 60% 23% Percentage of children among the new arrivals Unfunded XX% 60,606 [Figure] M Unfunded Total number of refugees, asylum-seekers and other $10.5 M people of concern in Zambia by end of September 2017 77% POPULATION OF CONCERN (AS OF 30 SEPTEMBER) CONTACTS By country of origin Pierrine Aylara Representative Population by Nationality [email protected] Tel: +260 977862002 Other 415 Somalia 3199 Kelvin Shimoh Public Information Associate Burundi 4749 [email protected] Rwanda 6130 Tel: +260979585832 Angola 18715 LINKS: DRC 27398 HTTPS:FACEBOOK.COM/UNHCRZAMBIA/ www.unhcr.org 1 EMERGENCY UPDATE > Zambia / 30 September 2017 Emergency Response Luapula province, northern Zambia Since 30 August, over 3,000 asylum-seekers from the Democratic Republic of Congo (DRC) have crossed into northern Zambia. New arrivals are reportedly fleeing insecurity and clashes between Congolese security forces FARDC and a local militia groups in towns of Pweto, Manono, Mitwaba (Haut Katanga Province) as well as in Moba and Kalemie (Tanganyika Province). -
Fostering Accountability and Transparency (FACT) in Zambia Quarterly Report
Fostering Accountability and Transparency (FACT) in Zambia Quarterly Report January 1 to March 30, 2019 Youth Symposium Participants Outside FQM Trident Foundation Limited Offices after receiving training from one of FACT partners Submission Date: April 30, 2019 Submitted by: Chilufya Kasutu Agreement Number: Chief of Party AID-611-14-L-00001 Counterpart International, Zambia Email: [email protected] Submitted to: Edward DeMarco, USAID Zambia AOR This document was produced for review by the United States Agency for International Development, Zambia (USAID/Zambia). It was prepared by Counterpart International. ACRONYMS AND ABBREVIATIONS AOR Agreement Officer’s Representative ART Anti-Retroviral Treatment CCAs Community Conservation Areas CCPs Community Conservation Plans CFGs Community Forest Groups CEFTA Citizens Engagement in Fostering Transparency and Accountability COMACO Community Markets for Conservation CRB Community Resource Boards CSPR Civil Society for Poverty Reduction CSO Civil Society Organization DAC District Advocacy Committee DAMI District Alternative Mining Indaba DDCC District Development Coordinating Committee DEBS District Education Board Secretary DHO District Health Office DIM District Integrated Meetings EITI Extractive Industries Transparency Initiative ESSP Education and Skills Sector Plan FACT Fostering Accountability and Transparency FZS Frankfurt Zoological Society GPE Global Partnership for Education GRZ Government of the Republic of Zambia HCC Health Centre Committee HIV Human Immunodeficiency Virus LAG -

The Impact of Cassava Growing in Luapula Valley, a Historical
THE IMPACT OF CASSAVA GROWING IN LUAPULA VALLEY, A HISTORICAL STUDY, 1900-1980 BY CHAMA KALUBA JICKSON A dissertation submitted to the University of Zambia in partial fulfilment of the requirements of the Degree of Master of Arts in History. THE UNIVERSITY OF ZAMBIA LUSAKA © 2016 DECLARATION I, Chama Kaluba Jickson, do hereby declare that this dissertation represents my own work; it has not been previously submitted for any degree at this or any other university; and does not incorporate any published work or material from another dissertation without citation. Signed: ............................................................. Date: ................................................................ i COPYRIGHT All rights reserved. No part of this dissertation may be reproduced or stored in any form or by any means without prior permission in writing from the author or the University of Zambia. ii APPROVAL This dissertation of CHAMA KALUBA JICKSON is approved as fulfilling the partial requirements for the award of the degree of Master of Arts in History by the University of Zambia. Signed: Date: ......................................................... ................................................ .......................................................... ................................................. .......................................................... ................................................. .......................................................... ................................................. iii ABSTRACT This -
DRAFT REPORT 2018 DA .Pdf
NATIONAL ASSEMBLY OF ZAMBIA REPORT OF THE COMMITTEE ON GOVERNMENT ASSURANCES FOR THE SECOND SESSION OF THE TWELFTH NATIONAL ASSEMBLY APPOINTED ON THURSDAY, 21ST SEPTEMBER, 2017 Printed by the National Assembly of Zambia i Table of Content 1.1 Functions of the Committee ........................................................................................... 1 1.2 Procedure adopted by the Committee .......................................................................... 1 1.3 Meetings of the Committee ............................................................................................ 2 PART I - CONSIDERATION OF SUBMISSIONS ON NEW ASSURANCES ............... 2 MINISTRY OF HIGHER EDUCATION ................................................................................ 2 11/17 Construction of FTJ Chiluba University .................................................................... 2 MINISTRY OF GENERAL EDUCATION ............................................................................. 3 39/17 Mateyo Kakumbi Primary School in Chitambo/Local Tour .................................. 3 21 /17 Mufumbwe Day Secondary School Laboratory ...................................................... 5 26/17 Pondo Basic School ....................................................................................................... 5 28/17 Deployment of Teachers to Nangoma Constituency ............................................... 6 19/16 Class Room Block at Lumimba Day Secondary School........................................... 6 17/17 Electrification -

National Health Insurance Management Authority
NATIONAL HEALTH INSURANCE MANAGEMENT AUTHORITY LIST OF ACCREDITED HEALTH CARE PROVIDERS AS OF SEPTEMBER 2021 Type of Facility Physical Address (Govt, Private, S/N Provider Name Service Type Province District Faith Based) 1 Liteta District Hospital Hospital Central Chisamba Government 2 Chitambo District Hospital Hospital Central Chitambo Government 3 Itezhi-tezhi District Hospital Hospital Central Itezhi tezhi Government 4 Kabwe Central Hospital Hospital Central Kabwe Government 5 Kabwe Women, Newborn & Children's HospHospital Central Kabwe Government 6 Kapiri Mposhi District Hospital Hospital Central Kapiri Mposhi Government 7 Mkushi District Hospital Hospital Central Mkushi Government 8 Mumbwa District Hospital Hospital Central Mumbwa Government 9 Nangoma Mission Hospital Hospital Central Mumbwa Faith Based 10 Serenje District Hospital Hospital Central Serenje Government 11 Kakoso 1st Level Hospital Hospital Copperbelt Chililabombwe Government 12 Nchanga North General Hospital Hospital Copperbelt Chingola Government 13 Kalulushi General Hospital Hospital Copperbelt Kalulushi Government 14 Kitwe Teaching Hospital Hospital Copperbelt Kitwe. Government 15 Roan Antelope General Hospital Hospital Copperbelt Luanshya Government 16 Thomson District Hospital Hospital Copperbelt Luanshya Government 17 Lufwanyama District Hospital Hospital Copperbelt Lufwanyama Government 18 Masaiti District Hospital Hospital Copperbelt Masaiti Government 19 Mpongwe Mission Hospital Hospital Copperbelt Mpongwe Faith Based 20 St. Theresa Mission Hospital Hospital -

Zambia 23 February 2018
INTER-AGENCY OPERATIONAL UPDATE Zambia 23 February 2018 Since September 2017, A combined total of 600 Five boreholes have 14,941 refugees have been children have been been drilled in registered at Kenani registered by Plan and Mantapala Refugee Transit Centre in Luapula Save the Children in Settlement by World Province. various categories of Vision International classes at the CFCs. KEY FIGURES 906 The Ministry of Health, with support from UN agencies and other partners, provides integrated health services at at Refugees have been relocated from Kenani to Kenani and Mantapala. © UNHCR/Bruce Mulenga.. Mantapala in five transfers 150 refugee families have built and moved in to their homes in Mantapala 76,000 Projected number of Congolese by 31 December 2018 ESTIMATEDFUNDING (ASTOTAL OF FEBRUINTER-ARYAGENCY 2018) FUNDING REQUIRED FOR THE CONGOLESE RESPONSE USDUSD 79,2 77,766,70066,700 M Total Inter-agency funding requested for the Congolese situation in Zambia Funded 6.559M Each head of the family at Kenani is given a plot to erect a shelter for the family. Above, a mother and her children Unfunded outside their home stead. UNHCR/Kelvin Shimoh 72.7M 1 INTER-AGENCY OPERATIONAL UPDATE > Zambia / 23 February 2018 Update on Achievements 76, 000 Projected number of Congolese by December 2018 Operational Context The protracted political stalemate in the Democratic Republic of Congo (DRC), characterized by delays to hold presidential elections has spiraled into pockets of instability across parts of the country, notably the eastern region, where clashes between militia groups and government forces have continued unabated. Though a continuous stream of Congolese refugees have found international protection in Zambia for decades, the recent political instability has resulted in a humanitarian crisis that has led to an increased number of persons fleeing to neighboring countries, including Zambia. -

Profiles of Active Civil Society Organisations in North-Western, Copperbelt and Southern Provinces of Zambia
Profiles of Active Civil Society Organisations in North-Western, Copperbelt and Southern Provinces of Zambia On behalf of Implemented by Published by: Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH Registered offices Bonn and Eschborn, Germany Address Civil Society Participation Programme (CSPP) Mpile Office Park, 3rd floor 74 Independence Avenue Lusaka, Zambia P +260 211 250 894 E [email protected] I www.giz.de/en Programme: Civil society participation in governance reform and poverty reduction Author: Isaac Ngoma, GFA Consulting Group GmbH Editor: Markus Zwenke, GFA Consulting Group GmbH, Eulenkrugstraße 82, 22359 Hamburg, Germany Design/layout: GFA Consulting Group GmbH and IE Zhdanovich Photo credits/sources: GFA Consulting Group GmbH On behalf of German Federal Ministry for Economic Cooperation and Development (BMZ) As of June, 2021 TABLE OF CONTENT ACTIVE CIVIL SOCIETY ORGANISATIONS IN NORTH-WESTERN PROVINCE � � � � � �7 Dream Achievers Academy �������������������������������������������������������������������������������������������������������������������������� 8 Anti-voter Apathy Project ���������������������������������������������������������������������������������������������������������������������������� 9 Mentra Youth Zambia . 10 The Africa Youth Initiative Network �������������������������������������������������������������������������������������������������������� 11 Radio Kabangabanga ���������������������������������������������������������������������������������������������������������������������������������� -

Zambia's Investment
ZAMBIA’S INVESTMENT PROJECTS ZAMBIA DEVELOPMENT AGENCY Promoting Zambia’s Economic Growth and Development Sponsored by Stanbic Bank ZAMBIA AT A GLANCE he peaceful and democratic country of Zambia has for many years enjoyed both social and political stability as well as a healthy macroeconomic environment, with Teconomic growth averaging 6 percent per annum since 2003. Backed by rich natural resources such as copper and cobalt, the minerals sector has for many years been at the forefront of Zambia’s expanding economy. Another prominent sector of the Zambian economy is agriculture, thanks to the country’s good soil and large tracts of fertile arable land. There is also an abundant hydropower resource to be found in the numerous lakes, dams and rivers. Efforts to further diversify the economy mean that increased attention is being given to the manufacturing sector for increased value addition to mineral and agro products and the tourism sector on the backdrop of abundant wildlife, numerous waterfalls and scenic beauty having great potential for further development. Strategically Located - Land Linked Kenya South Africa AGRICULTURE SECTOR ZAMBIA DEVELOPMENT AGENCY 3 AGRICULTURE SECTOR INVESTMENT OPPORTUNITIES No. Project Title Project Summary Estimated Contracting Project Investment Authority Requirements/ (US$) and/ or Financing Promoter Mode 1. Farm Block The Government of the Republic of Zambia To be Ministry of Private Sector Development identified Agriculture as the Engine to determined Agriculture funding/ Programme Economic development as well as the Main by the investment stay of the Economy. In 2002 GRZ embarked type of on development and commercialization agribusiness of agriculture land as the Farm Block Development Programme (FBDP). -

The Political Ecology of a Small-Scale Fishery, Mweru-Luapula, Zambia
Managing inequality: the political ecology of a small-scale fishery, Mweru-Luapula, Zambia Bram Verelst1 University of Ghent, Belgium 1. Introduction Many scholars assume that most small-scale inland fishery communities represent the poorest sections of rural societies (Béné 2003). This claim is often argued through what Béné calls the "old paradigm" on poverty in inland fisheries: poverty is associated with natural factors including the ecological effects of high catch rates and exploitation levels. The view of inland fishing communities as the "poorest of the poorest" does not imply directly that fishing automatically lead to poverty, but it is linked to the nature of many inland fishing areas as a common-pool resources (CPRs) (Gordon 2005). According to this paradigm, a common and open-access property resource is incapable of sustaining increasing exploitation levels caused by horizontal effects (e.g. population pressure) and vertical intensification (e.g. technological improvement) (Brox 1990 in Jul-Larsen et al. 2003; Kapasa, Malasha and Wilson 2005). The gradual exhaustion of fisheries due to "Malthusian" overfishing was identified by H. Scott Gordon (1954) and called the "tragedy of the commons" by Hardin (1968). This influential model explains that whenever individuals use a resource in common – without any form of regulation or restriction – this will inevitably lead to its environmental degradation. This link is exemplified by the prisoner's dilemma game where individual actors, by rationally following their self-interest, will eventually deplete a shared resource, which is ultimately against the interest of each actor involved (Haller and Merten 2008; Ostrom 1990). Summarized, the model argues that the open-access nature of a fisheries resource will unavoidably lead to its overexploitation (Kraan 2011). -

Quarterly Progress Report (January – March, 2017)
Quarterly Progress Report (January – March, 2017) Approval Date: September 30, 2015 QPR Number: [002] Contract/Agreement Number: [AID-611-C-15-00002] Activity Start Date and End Date: [October 1, 2015 to September 30, 2020] Total Award Amount: [$24,389,716.00] Submitted by: [PATH Zambia Office, Stand 11059, Brentwood Lane, Lusaka] [Tel: +260211378950] DISCLAIMER: The author’s views expressed in this report do not necessarily reflect the views of the United States Agency for International Development (USAID), United States President’s Malaria Initiative (PMI) or the United States Government List of Abbreviations ANC Antenatal care BRITE Broad Reach Institute for Training & Education CBO Community-based organizations CD Continuous distribution CHA Community Health Assistant CHAZ Churches Health Association of Zambia CHW Community Health Worker COP Chief of Party CSO Civil Society Organization DHD District Health Director DHO District Health Office DHIS2 District Health Information System 2 DHS Demographic Health Survey DIM District Integrated Meeting EPI Expanded Program on Immunization GRZ Government of the Republic of Zambia GUC Grants under contract HMIS Health Management Information System iCCM Integrated community case management IEC Information, education, and communication IPTp Intermittent preventive treatment in pregnancy IRS Indoor residual spraying ITN Insecticide-treated net JHUCCP Johns Hopkins University Center for Communication Programs LLIN Long Lasting Insecticide Treated Net MACEPA Malaria Control and Elimination Partnership -

2000 Census of Population and Housing
2000 Census of Population and Housing Published by Central Statistical Office, P. O. Box 31908, Lusaka, Luapula. Tel: 260-01-251377/253468 Fax: 260-01-253468 E-mail: [email protected] Website: www.zamstats.gov.zm September, 2004 COPYRIGHT RESERVED Extracts may be published if Sources are duly acknowledged. Table of Content and Executive Summary i Table of Content and Executive Summary ii Preface The 2000 Census of Population and Housing was undertaken from 16th October to 15th November, 2000. This was the fourth census since Independence in 1964. The other three were carried out in 1969, 1980 and 1990. The 2000 Census operations were undertaken with the use of Grade 11 pupils as enumerators, Primary School Teachers as supervisors, Professionals from within Central Statistical Office and other government departments being as Trainers and Management Staff. Professionals and Technical Staff of the Central Statistical Office were assigned more technical and professional tasks. This report presents detailed analysis of issues on evaluation of coverage and content errors; population, size, growth and composition; ethnicity and languages; economic and education characteristics; fertility; mortality and disability. The success of the Census accrues to the dedicated support and involvement of a large number of institutions and individuals. My sincere thanks go to Co-operating partners namely the British Government, the Japanese Government, the United States Agency for International Development (USAID), United Nations Population Fund (UNFPA), the Norwegian Government, the Dutch Government, the Finnish Government, the Danish Government, the German Government, University of Michigan, the United Nations High Commission for Refugees (UNHCR) and the Canadian Government for providing financial, material and technical assistance which enabled the Central Statistical Office carry out the Census. -

Implementation Status & Results
The World Bank Report No: ISR7790 Implementation Status & Results Zambia Road Rehabilitation and Maintenance Project (P071985) Operation Name: Road Rehabilitation and Maintenance Project (P071985) Project Stage: Implementation Seq.No: 20 Status: ARCHIVED Archive Date: 27-Mar-2013 Country: Zambia Approval FY: 2004 Public Disclosure Authorized Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Adaptable Program Loan Implementing Agency(ies): National Road Fund Agency Key Dates Board Approval Date 09-Mar-2004 Original Closing Date 30-Jun-2007 Planned Mid Term Review Date Last Archived ISR Date 07-Jun-2012 Public Disclosure Copy Effectiveness Date 15-Jun-2004 Revised Closing Date 30-Jun-2014 Actual Mid Term Review Date 14-Jul-2006 Project Development Objectives Project Development Objective (from Project Appraisal Document) The revised project development objectives are to: (i) develop the institutional capacity for sustainable management of public roadinfrastructure and road safety, (ii) preserve road assets in targeted transport corridors, and (iii) rehabilitate and construct targeted transport infrastructure. Has the Project Development Objective been changed since Board Approval of the Project? ● Yes No Public Disclosure Authorized Component(s) Component Name Component Cost 1. CIVIL WORKS 74.30 2. ENGINEERING AND TECHNICAL SERVICES 7.00 3. INSTITUTIONAL DEVELOPMENT AND CAPACITY BUILDING 5.40 4. ACCESSIBILITY AND MOBILITY IMPROVEMENT 3.30 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Moderately Satisfactory Satisfactory Public Disclosure Authorized Overall Implementation Progress (IP) Moderately Satisfactory Moderately Unsatisfactory Overall Risk Rating Implementation Status Overview 1. Almost all of the activities planned under the original $50 million credit have been completed and nearly 95% of it disbursed.