On the Genesis of Air Cells in the Conchæ Nasales
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

Macroscopic Anatomy of the Nasal Cavity and Paranasal Sinuses of the Domestic Pig (Sus Scrofa Domestica) Daniel John Hillmann Iowa State University
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 1971 Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica) Daniel John Hillmann Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Animal Structures Commons, and the Veterinary Anatomy Commons Recommended Citation Hillmann, Daniel John, "Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica)" (1971). Retrospective Theses and Dissertations. 4460. https://lib.dr.iastate.edu/rtd/4460 This Dissertation is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. 72-5208 HILLMANN, Daniel John, 1938- MACROSCOPIC ANATOMY OF THE NASAL CAVITY AND PARANASAL SINUSES OF THE DOMESTIC PIG (SUS SCROFA DOMESTICA). Iowa State University, Ph.D., 1971 Anatomy I University Microfilms, A XEROX Company, Ann Arbor. Michigan I , THIS DISSERTATION HAS BEEN MICROFILMED EXACTLY AS RECEIVED Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica) by Daniel John Hillmann A Dissertation Submitted to the Graduate Faculty in Partial Fulfillment of The Requirements for the Degree of DOCTOR OF PHILOSOPHY Major Subject: Veterinary Anatomy Approved: Signature was redacted for privacy. h Charge of -^lajoï^ Wor Signature was redacted for privacy. For/the Major Department For the Graduate College Iowa State University Ames/ Iowa 19 71 PLEASE NOTE: Some Pages have indistinct print. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery
MÜSBED 2013;3(2):102-106 DOI: 10.5455/musbed.20130410100848 Derleme / Review Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery Filiz Namdar Pekiner Department of Oral Diagnosis and Radiology, Faculty of Dentistry, Marmara University, Istanbul - Turkey Ya zış ma Ad re si / Add ress rep rint re qu ests to: Filiz Namdar Pekiner, Marmara University, Faculty of Dentistry, Department of Oral Diagnosis and Radiology, Nisantasi, Istanbul - Turkey Elekt ro nik pos ta ad re si / E-ma il add ress: [email protected] Ka bul ta ri hi / Da te of ac cep tan ce: 10 Nisan 2013 / April 10, 2013 ÖZET ABS TRACT Fonksiyonel endoskopik sinüs cerrahisinde mul- Anatomic variations of paranasal sinus tidetektör bilgisayarlı tomografide paranasal on multidetector computed tomography sinüslerin anatomik varyasyonları examinations for functional endoscopic sinus surgery Bilgisayarlı tomografi paranasal sinüslerin hastalıklarının ve fonksiyo- nel endoskopik sinüs cerrahisi ile tedavilerinin değerlendirilmesinde Computed tomography is excellent means of providing anatomical anatomik olarak sağladığı bilgi oldukça önemlidir. Paranasal sinüs- information of paranasal sinuses, assessing disease and guiding lerde izlenen anatomik varyasyonlar nadir değildir. Bu makalenin treatment with functional endoscopic sinus surgery (FESS). Common amacı paranasal sinüslerde izlenebilen bazı anatomik varyasyonları anatomical variations are not rare in the paranasal sinuses. The aim of sunmaktır. this article was presented radiological characteristics of some anatomic Anahtar sözcükler: Paranasal sinüsler, anatomik varyasyonlar, bilgi- variation in paranasal sinuses. sayarlı tomografi, fonksiyonel endoskopik sinüs cerrahisi Key words: Paranasal sinus, anatomical variation, computed tomography, functional endoscopic sinus surgery INTRODUCTION anatomy as shown on CT are of potential significance, it may predispose to certain pathologic conditions and Functional endoscopic sinus surgery (FESS) has been diseases (5). -
The Axial Skeleton Visual Worksheet
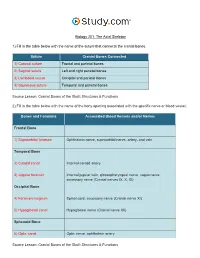
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -
![NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp](https://docslib.b-cdn.net/cover/6054/nasal-cavity-and-paranasal-sinuses-pterygopalatine-fossa-and-oral-cavity-grants-dissector-16th-ed-pp-1806054.webp)
NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp
NASAL CAVITY AND PARANASAL SINUSES, PTERYGOPALATINE FOSSA, AND ORAL CAVITY (Grant's Dissector [16th Ed.] pp. 290-294, 300-303) TODAY’S GOALS (Nasal Cavity and Paranasal Sinuses): 1. Identify the boundaries of the nasal cavity 2. Identify the 3 principal structural components of the nasal septum 3. Identify the conchae, meatuses, and openings of the paranasal sinuses and nasolacrimal duct 4. Identify the openings of the auditory tube and sphenopalatine foramen and the nerve and blood supply to the nasal cavity, palatine tonsil, and soft palate 5. Identify the pterygopalatine fossa, the location of the pterygopalatine ganglion, and understand the distribution of terminal branches of the maxillary artery and nerve to their target areas DISSECTION NOTES: General comments: The nasal cavity is divided into right and left cavities by the nasal septum. The nostril or naris is the entrance to each nasal cavity and each nasal cavity communicates posteriorly with the nasopharynx through a choana or posterior nasal aperture. The roof of the nasal cavity is narrow and is represented by the nasal bone, cribriform plate of the ethmoid, and a portion of the sphenoid. The floor is the hard palate (consisting of the palatine processes of the maxilla and the horizontal portion of the palatine bone). The medial wall is represented by the nasal septum (Dissector p. 292, Fig. 7.69) and the lateral wall consists of the maxilla, lacrimal bone, portions of the ethmoid bone, the inferior nasal concha, and the perpendicular plate of the palatine bone (Dissector p. 291, Fig. 7.67). The conchae, or turbinates, are recognized as “scroll-like” extensions from the lateral wall and increase the surface area over which air travels through the nasal cavity (Dissector p. -

Splanchnocranium
splanchnocranium - Consists of part of skull that is derived from branchial arches - The facial bones are the bones of the anterior and lower human skull Bones Ethmoid bone Inferior nasal concha Lacrimal bone Maxilla Nasal bone Palatine bone Vomer Zygomatic bone Mandible Ethmoid bone The ethmoid is a single bone, which makes a significant contribution to the middle third of the face. It is located between the lateral wall of the nose and the medial wall of the orbit and forms parts of the nasal septum, roof and lateral wall of the nose, and a considerable part of the medial wall of the orbital cavity. In addition, the ethmoid makes a small contribution to the floor of the anterior cranial fossa. The ethmoid bone can be divided into four parts, the perpendicular plate, the cribriform plate and two ethmoidal labyrinths. Important landmarks include: • Perpendicular plate • Cribriform plate • Crista galli. • Ala. • Ethmoid labyrinths • Medial (nasal) surface. • Orbital plate. • Superior nasal concha. • Middle nasal concha. • Anterior ethmoidal air cells. • Middle ethmoidal air cells. • Posterior ethmoidal air cells. Attachments The falx cerebri (slide) attaches to the posterior border of the crista galli. lamina cribrosa 1 crista galli 2 lamina perpendicularis 3 labyrinthi ethmoidales 4 cellulae ethmoidales anteriores et posteriores 5 lamina orbitalis 6 concha nasalis media 7 processus uncinatus 8 Inferior nasal concha Each inferior nasal concha consists of a curved plate of bone attached to the lateral wall of the nasal cavity. Each consists of inferior and superior borders, medial and lateral surfaces, and anterior and posterior ends. The superior border serves to attach the bone to the lateral wall of the nose, articulating with four different bones. -

Estimation of Nasal Cavity and Conchae Volumes by Stereological Method
Folia Morphol. Vol. 71, No. 2, pp. 105–108 Copyright © 2012 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Estimation of nasal cavity and conchae volumes by stereological method M. Emirzeoglu1, B. Sahin1, M. Celebi2, A. Uzun1, S. Bilgic1, H.O. Tontus3 1Anatomy Department, Medical Faculty, Ondokuz Mayis University, Samsun, Turkey 2ENT Department, Mehmet Aydin Research Hospital, Samsun, Turkey 3Medical Education Department, Medical Faculty, Ondokuz Mayis University, Samsun, Turkey [Received 16 February 2012; Accepted 23 February 2012] Background: Studies evaluating the mean volumes of nasal cavity and concha are very rare. Since there is little date on the mentioned topic, we aimed to carry out the presented study to obtain a volumetric index showing the relation between the nasal cavity and concha. Material and methods: The volumes of the nasal cavity and concha were measured in 30 males and 30 females (18–40 years old) on computed tomo- graphy images using stereological methods. Results: The mean volumes of nasal cavity, concha nasalis media, and concha nasalis inferior were 5.95 ± 0.10 cm3, 0.56 ± 0.22 cm3, and 1.45 ± 0.68 cm3; 7.01 ± 0.18 cm3, 0.67 ± 0.31 cm3 and 1.59 ± 0.98 cm3 in females and males, respectively. There were statistically significant differences in the volume of the nasal cavity and concha nasalis media (p < 0.05) between males and females, except for concha nasalis inferior (p > 0.05). Conclusions: Our results could provide volumetric indexes for the nasal cavity and concha, which could help the physician to manage surgical procedures related to the nasal cavity and concha. -

Nasal Septum Deviation and Inferior Nasal Concha Bone Hypertrophy in Class III Facial Deformity
Int. J. Morphol., 38(6):1544-1548, 2020. Nasal Septum Deviation and Inferior Nasal Concha Bone Hypertrophy in Class III Facial Deformity Desviación del Septum Nasal e Hipertrofia de la Concha Nasal Inferior en Deformidad Facial Clase III Javier Villa1; Leonardo Brito2,3; Marcelo Parra2,4; Pablo Navarro3; Márcio de Moraes6 & Sergio Olate2,4 VILLA, J.; BRITO, L.; PARRA, M.; NACARRO, P.; DE MORAES, M.; OLATE, S. Nasal septum deviation and inferior nasal concha bone hypertrophy in Class III facial deformity. Int. J. Morphol., 38(6):1544-1548, 2020. SUMMARY: The aim of this research was to analyze the morphology of the nasal septum and inferior nasal concha bone in class III facial deformities prior to orthodontic treatment in orthognathic surgery candidates. 40 subjects were included in this research. The inclusion criteria were an Angle class III, negative overjet and SNA angle less than 80º. Patients with facial asymmetry, facial trauma or who had undergone maxillofacial or ENT procedures were excluded. CBCT images were obtained for all the patients and the nasal septum deviation, morphology of inferior nasal concha bone and ostium of the maxillary sinus were analyzed and related to the complexity of the facial deformity expressed by the ANB angle and dental relations. The measurement was standardized by ICC and the data was analyzed using a chi square test and Spearman’s coefficient with a p value < 0.005 for statistical significance. Nasal septal deviation was observed in 77.5 %. The deviation angle was 13.28º (±4.68º) and the distance from the midline to the most deviated septum was 5.56 mm (±1.8 mm) with no statistical relation to the complexity of the facial deformity. -

Crista Galli (Part of Cribriform Plate of Ethmoid Bone)
Alveolar margins alveolar margins coronal suture coronal suture coronoid process crista galli (part of cribriform plate of ethmoid bone) ethmoid bone ethmoid bone ethmoid bone external acoustic meatus external occipital crest external occipital protuberance external occipital protuberance frontal bone frontal bone frontal bone frontal sinus frontal squama of frontal bone frontonasal suture glabella incisive fossa inferior nasal concha inferior nuchal line inferior orbital fissure infraorbital foramen internal acoustic meatus lacrimal bone lacrimal bone lacrimal fossa lambdoid suture lambdoid suture lambdoid suture mandible mandible mandible mandibular angle mandibular condyle mandibular foramen mandibular notch mandibular ramus mastoid process of the temporal bone mastoid process of the temporal bone maxilla maxilla maxilla mental foramen mental foramen middle nasal concha of ethmoid bone nasal bone nasal bone nasal bone nasal bone occipital bone occipital bone occipital bone occipitomastoid suture occipitomastoid suture occipitomastoid suture occipital condyle optic canal optic canal palatine bone palatine process of maxilla parietal bone parietal bone parietal bone parietal bone perpendicular plate of ethmoid bone pterygoid process of sphenoid bone sagittal suture sella turcica of sphenoid bone Sphenoid bone (greater wing) spehnoid bone (greater wing) sphenoid bone (greater wing) sphenoid bone (greater wing) sphenoid sinus sphenoid sinus squamous suture squamous suture styloid process of temporal bone superior nuchal line superior orbital fissure supraorbital foramen (notch) supraorbital margin sutural bone temporal bone temporal bone temporal bone vomer bone vomer bone zygomatic bone zygomatic bone. -

Anatomical Study of the Middle Meatus with Emphasis to the Maxillary Ostium and Their Clinical Relevance
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Anatomical Study of the Middle Meatus with Emphasis to the Maxillary Ostium and Their Clinical Relevance Anne D Souza1, Vrinda Hari Ankolekar1, Kumar M. R. Bhat2, Sushma R. K3, Antony Sylvan D Souza4 1Assistant Professor, 2Additional Professor, 3Lecturer, 4Professor and Head, Department of Anatomy, Kasturba Medical College, Manipal University, Manipal. Karnataka, India Corresponding Author: Sushma R. K Received: 03/01//2014 Revised: 27/01/2014 Accepted: 03/02/2014 ABSTRACT Introduction: The anatomical variations of the lateral wall of the nasal cavity may create technical difficulties during endoscopic sinus surgeries. Interventions involving the middle meatus are commonly performed as majority of the paranasal sinuses open into the osteomeatal complex. The present study was therefore designed to provide information on maxillary ostium in relation to the important anatomical landmarks and also about the variations possible in the morphology of the middle meatus. Materials and methods: The present observational study was carried out on 25sagittal sections of head and neck in the department of Anatomy Kasturba Medical College, Manipal. The nasal septum was removed to visualize the lateral wall. The middle meatus was then studied for the variations possible in the openings of the bulla ethmoidalis and hiatus semilunaris. The distance of the maxillary ostium from the prominent landmarks was measured. The findings were recorded and tabulated. Results: The mean and standard deviations of the parameters were measured. The variations in the middle nasal concha and the bulla ethmoidalis were also observed. Conclusion: This knowledge about the variations in the lateral wall of the nasal cavity is crucial during the endoscopic interventions and for functional endoscopic sinus surgeries.