Disaster Medical System in Japan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Resilient Infrastructure Ppps 15 1.3 Scope and Objectives of This Study 19 1.4 Selection of Cases for the Japan Case Study 20 1.5 Structure of This Report 21
Resilient Infrastructure Public-Private Partnerships (PPPs): Contracts and Procurement Contracts Public-Private Infrastructure Partnerships (PPPs): Resilient Resilient Infrastructure Public Disclosure Authorized Public-Private Partnerships (PPPs): Contracts and Procurement Public Disclosure Authorized The Case of Japan The Case of Japan The Case Public Disclosure Authorized Public Disclosure Authorized ©2017 The World Bank International Bank for Reconstruction and Development The World Bank Group 1818 H Street NW, Washington, DC 20433 USA December 2017 DISCLAIMER This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immunities of The World Bank, all of which are specifically reserved. The report reflects information available up to November 30, 2017. RIGHTS AND PERMISSIONS The material in this work is subject to copyright. Because The World Bank encourages dissemination of its knowledge, this work may be reproduced, in whole or in part, for noncommercial purposes as long as full attribution to this work is given. Any queries on rights and licenses, including subsidiary rights, should be addressed to World Bank Publications, The World Bank Group, 1818 H Street NW, Washington, DC 20433, USA; e-mail: [email protected]. -

European Biotech and Pharma Partnering Conference, Osaka 2019
European Biotech and Pharma partnering Conference, Osaka 2019 Partnering Conference Schedule, 8 October, 2018 8:30 – 9:00 Registration 9:00 – 9:15 Welcome and Opening Remarks 9:20 – 10:20 B2B meeting – Session 1 9:20 – 11:50 B2B meeting – Session 2 12:00 – 13:20 Networking lunch 13:30 – 15:00 B2B meeting – Session 3 15:00 – 16:00 B2B meeting – Session 4 Venue Senri Hankyu Hotel Senjyu, West Building 2F *Address: Senri Hankyu Hotel, 2-1 Shinsenri Higashimachi, Toyonaka-shi, Ōsaka-fu, 560-0082, Japan *Address in Japanese: 大阪府豊中市新千里東町2丁目1番 Access to the venue Nearest station: Senri-Chuo Station How to get there? from Kansai International Airport about 80 minutes by Limousine Bus, (get off at Itami Airport) transfer to Osaka Monorail from Itami Airport, take Osaka Monorail at Osaka Airport Station to Senri-Chuo for about 12 min. (get off at Senri-Chuo Station) From Shin-Osaka Station (Shinkansen Station) about 15 min. by Subway Midosuji Line via Esaka Station to Senri-Chuo Station from Umeda Station about 20 min. by Subway Midosuji Line via Esaka Station to Senri-Chuo Station 1 Senri Chuo Station Senri Hankyu Hotel Senju Hall, West Building 2F Floor layout Poster Spaces Registration (Japanese Participants) Registration (European Participants) Partnering Platform Please accept or reject any pending requests as soon as possible, because other participants will not be able to send requests anymore if their list of pending requests gets too long. See your meeting’s status Meeting requests can only be made until October 1st, 2019. Browse participants Confirmations of preliminary schedules are planned to be sent by October 3, 2019. -

Masters Village Hyogo Duo Kobe “Duo Dome” (JR Kobe Sta
Transport Information Guide Venue Hyogo pref. Kobe City Masters Village Hyogo Duo Kobe “Duo Dome” (JR Kobe Sta. basement) 2-1 Aioicho, Chuoku, Kobe City, Hyogo http://www.duokobe.com/ ■Access to Masters Village Hyogo From Kansai International Airport Airport Kobe-Sannomiya Sannomiya Kobe Bus Airport Bus Sta. Sta. JR Kobe Line Sta. Directly 【65min.】 【3min.】 Connected JR Osaka Kobe JR Kansai-airport Line Sta. JR Kobe Line Sta. Directly 【60min.】 【26min.】 Connected ※ Transport passes can be used for JR train from Osaka to Kobe. They will be delivered to Games Check-in at Center Village located near JR Osaka Station if you have applied in advance. From Osaka International Airport ( Itami Airport) Duo Airport Kobe-Sannomiya Sannomiya Kobe Dome Bus Airport Bus Sta. Sta. JR Kobe Line Sta. Directly 【40min.】 【3min.】 Connected From Shin-Kobe Station Kobe City Sannomiya Sannomiya Kobe Subway Subway Seishin-Yamate Line Sta. Sta. JR Kobe Line Sta. Directly 【2min.】 【3min.】 Connected Kobe Airport Port Sannomiya Sannomiya Kobe Liner Port Liner Sta. Sta. JR Kobe Line Sta. Directly 【18min.】 【3min.】 Connected Osaka International Airport (Itami Airport) for Okayama Shinkansen for Kyoto Shin-Kobe Shin-Osaka Sta. Sta. for Seishin-Cyuo Subway Seishin-Yamate Line for Nishi-Akashi Kobe Sannomiya Osaka Sta. Sta. Sta. JR Kobe Line Port Liner 【Masters Village Hyogo】 Duo Kobe “Duo Dome” Kobe Airport JR Line JR Shinkansen Kansai Subway International Seishin-Yamate Line Airport PortLiner Airport Bus Transport Information Guide ■ Access map to Masters Village Hyogo ■ Transportation information to Masters Village Hyogo (Duo Dome) From JR Kobe Station, exit out of Central Gate, go down to the basement floor using the escalator at the south exit. -

Interaction of Lifecycle Properties in High Speed Rail Systems Operation
Interaction of Lifecycle Properties in High Speed Rail Systems Operation by Tatsuya Doi M.E., Aeronautics and Astronautics, University of Tokyo, 2011 B.E., Aeronautics and Astronautics, University of Tokyo, 2009 Submitted to the Institute for Data, Systems, and Society in partial fulfillment of the requirements for the degree of Master of Science in Engineering Systems at the Massachusetts Institute of Technology June 2016 © 2016 Tatsuya Doi. All rights reserved. The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic copies of this thesis document in whole or in part in any medium now known or hereafter created. Signature of Author: ____________________________________________________________________ Institute for Data, Systems, and Society May 6, 2016 Certified by: __________________________________________________________________________ Joseph M. Sussman JR East Professor of Civil and Environmental Engineering and Engineering Systems Thesis Supervisor Certified by: __________________________________________________________________________ Olivier L. de Weck Professor of Aeronautics and Astronautics and Engineering Systems Thesis Supervisor Accepted by: _________________________________________________________________________ John N. Tsitsiklis Clarence J. Lebel Professor of Electrical Engineering IDSS Graduate Officer 1 2 Interaction of Lifecycle Properties In High Speed Rail Systems Operation by Tatsuya Doi Submitted to the Institute for Data, Systems, and Society on May 6, 2016 in Partial Fulfillment of the Requirements for the Degree of Master of Science in Engineering Systems ABSTRACT High-Speed Rail (HSR) has been expanding throughout the world, providing various nations with alternative solutions for the infrastructure design of intercity passenger travel. HSR is a capital-intensive infrastructure, in which multiple subsystems are closely integrated. Also, HSR operation lasts for a long period, and its performance indicators are continuously altered by incremental updates. -
Operating Results by Business Segment — —
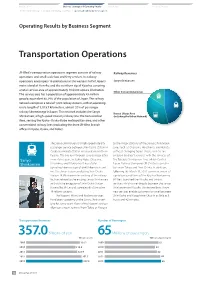
Introduction Business Strategy and Operating Results ESG Section Financial Section The President’s Message Medium-Term Management Plan Operating Results by Business Segment — — Operating Results by Business Segment Transportation Operations JR-West’s transportation operations segment consists of railway Railway Revenues operations and small-scale bus and ferry services. Its railway operations encompass 18 prefectures in the western half of Japan’s Sanyo Shinkansen main island of Honshu and the northern tip of Kyushu, covering a total service area of approximately 104,000 square kilometers. Other Conventional Lines The service area has a population of approximately 43 million people, equivalent to 34% of the population of Japan. The railway network comprises a total of 1,222 railway stations, with an operating route length of 5,015.7 kilometers, almost 20% of passenger railway kilometerage in Japan. This network includes the Sanyo Kansai Urban Area Shinkansen, a high-speed intercity railway line; the Kansai Urban (including the Urban Network) Area, serving the Kyoto–Osaka–Kobe metropolitan area; and other conventional railway lines (excluding the three JR-West branch offices in Kyoto, Osaka, and Kobe). The Sanyo Shinkansen is a high-speed intercity to the major stations of the Sanyo Shinkansen passenger service between Shin-Osaka Station in Line, such as Okayama, Hiroshima, and Hakata, Osaka and Hakata Station in Fukuoka in northern without changing trains. These services are Kyushu. The line runs through several major cities enabled by direct services with the services of Sanyo in western Japan, including Kobe, Okayama, the Tokaido Shinkansen Line, which Central Shinkansen Hiroshima, and Kitakyushu. -

LUGGAGE-FREE TRAVEL Same-Day Delivery
LUGGAGE-FREE TRAVEL Same-day Delivery ◆Airport ✈ → Hotel Delivery Delivery City Drop-off Earliest delivery From To Narita Airport 6:30ー10:00 Tokyo(Chiba) Ibaraki、Tochigi、Gunma、Saitama、Chiba、Tokyo、Kanagawa、Yamanashi Haneda airport 00:00ー10:30 Osaka Kansai International Airport 6:30ー9:30 Osaka、Kyoto、Hyogo、Nara、Shiga Chubu International Airport Terminal 1 7:00ー11:00 Aichi、Mie、Gifu Nagoya 18:00ー21:00 Chubu International Airport Terminal 2 10:00ー11:00 Aichi、Mie、Gifu Sendai Station Sendai International Airport 8:00ー9:30 Within Miyagi Sapporo New Chitose Airport 7:30ー10:00 Within Sapporo Cuty Fukuoka Fukuoka Airport 7:30ー11:30 Within Chuo Area, Fukuoka Area *Luggage that is dropped-off after the above mentioned time, but before 18:00 will be delivered by the next day. ◆Station → Hotel Delivery Delivery City・Station Drop-off Earliest delivery From To Yamato Transport Asahikawa Station Kitasaito Center (JR Within Asahikawa Area・Furano City・Within Sounkyo-Onsen Kamikawagun Asahikawa Station 8:00ー16:30 Asahikawa Station) Kamikawa Town Yamato Transport Sendai Station 2F Baggage Service Sendai Station 9:00ー10:30 Within Miyagi Counter (JR Sendai Station) Ginza Yamato Transport Ginza Konyabashi Center (Tokyo Metro 8:00ー11:00 Ibaraki、Tochigi、Gunma、Saitama、Chiba、Tokyo、Kanagawa、Yamanashi Yurakucho Staion Ginza Station, JR Yurakucho Station) Yokohama Yamato Transport Sakuragicho Station Tourist Information Sakuragcho 9:00ー10:00 Ibaraki、Tochigi、Gunma、Saitama、Chiba、Tokyo、Kanagawa、Yamanashi Center (JR Sakuragicho Station) Station Nagano Yamato Transport MIDORI -

Arrival Instructions
ARRIVAL INSTRUCTIONS In planning your trip to Japan, please read these arrival instructions carefully, for they provide important and useful information for your smooth arrival in Japan. IMPORTANT DATES FOR SPRING 2020 December 2 Deadline for submitting arrival information thru K-GENESYS January 17 University accommodations become available. January 17-18 Expected arrival period January 20 Orientation programs begin. (Attendance required.) CONTENTS PAGE 1 ・Important Dates and Contents PAGE 2 ・Pick-up Service PAGE 3 ・Orientation Accommodations ・Addresses of Accommodations ・Location of the Center for International Education PAGES 4 - 6 ・Making Your Own Arrival Arrangements KIX, ITM and JR Kyoto Station Limousine Bus Schedule PAGE 7 ・Call Your Family upon Arrival ・Return Flight PAGE 8 - 9 ・List of Hotels and Useful Websites PAGE 10 ・Check List - Have you done everything right? - NOTE: All information in this document is subject to change without prior notice. 1 PICK-UP SERVICE Pick-up service is available for all new international students at two locations: Kansai International Airport (KIX) and Osaka Itami Airport (ITM and also known as Osaka International Airport). Although you can make your own arrangements to get to Kansai Gaidai, we strongly recommend that you take advantage of our pick-up service in order to ensure your smooth arrival. It is important to note that, given the distance from the above two gateways to Kansai Gaidai, if you are not familiar with Japan’s public transportation system, you will likely encounter some difficulties on the way to Kansai Gaidai. If you use our pick-up service, you will be taken to the area of our university housing and will be guided to your assigned accommodation (to be announced in early August). -

Study on Airport Ownership and Management and the Ground Handling Market in Selected Non-European Union (EU) Countries
Study on airport DG MOVE, European ownership and Commission management and the ground handling market in selected non-EU countries Final Report Our ref: 22907301 June 2016 Client ref: MOVE/E1/SER/2015- 247-3 Study on airport DG MOVE, European ownership and Commission management and the ground handling market in selected non-EU countries Final Report Our ref: 22907301 June 2016 Client ref: MOVE/E1/SER/2015- 247-3 Prepared by: Prepared for: Steer Davies Gleave DG MOVE, European Commission 28-32 Upper Ground DM 28 - 0/110 London SE1 9PD Avenue de Bourget, 1 B-1049 Brussels (Evere) Belgium +44 20 7910 5000 www.steerdaviesgleave.com Steer Davies Gleave has prepared this material for DG MOVE, European Commission. This material may only be used within the context and scope for which Steer Davies Gleave has prepared it and may not be relied upon in part or whole by any third party or be used for any other purpose. Any person choosing to use any part of this material without the express and written permission of Steer Davies Gleave shall be deemed to confirm their agreement to indemnify Steer Davies Gleave for all loss or damage resulting therefrom. Steer Davies Gleave has prepared this material using professional practices and procedures using information available to it at the time and as such any new information could alter the validity of the results and conclusions made. The information and views set out in this report are those of the authors and do not necessarily reflect the official opinion of the European Commission. -

Best of Japan Your Way 15 Days / 14 Nights Best of Japan Your Way
Best of Japan Your Way 15 Days / 14 Nights Best of Japan Your Way Tour Overview On the Best of Japan Your Way tour, you will be escorted from city to city just like on our escorted tours. But once you arrive at the destination, you are free to explore on your own just like on our self-guided packages. Or you can join one of our daily optional guided tours. A little bit of structure with a lot of flexibility may be the perfect combination for you. Destinations Tokyo, Hakone, Takayama, Koya-san, Osaka, Himeji, Miyajima Island, Hiroshima, Kyoto, Fushimi, Nara Tour Factors Cultural Immersion Pace Physical Activity Tour Details You’ll enjoy a colorful mix of large cities like Tokyo and Osaka, quaint and traditional Takayama, the ambiance and solitude of Miyajima Island, the historically significant Kamakura (the capital of Japan in the 13th century), the religious center of Koya-san, ancient Kyoto, the testament to peace of Hiroshima, the natural beauty of Hakone, the thermally-heated mineral water baths at an onsen and much, much more. You’ll stay overnight at a mountaintop Buddhist temple where Buddhist monks will serve you meals of shojin ryori (the traditional Buddhist vegetarian cuisine), and you can attend prayer services at the temple early the next morning. You will have the opportunity to climb to the top of a samurai castle, stroll through farmer’s markets, see where the geisha live and work, take in the view on beautiful and quiet Miyajima Island, soak in the thermally-heated mineral waters at an onsen, admire sacred Mt. -

For the Safety of Hokkaido, Hiroshima, Fukuoka, Kagoshima and Okinawa (Office for Novel Coronavirus Disease Control, Cabinet Secretariat)
For the safety of Hokkaido, Hiroshima, Fukuoka, Kagoshima and Okinawa (Office for Novel Coronavirus Disease Control, Cabinet Secretariat) Objective Entity To ensure the safety of residents of Hokkaido, Hiroshima, Fukuoka, Japanese Government (conducted by a testing vendor) Kagoshima and Okinawa, as well as those who have to travel. To contribute to early detection of infection sources and limit infections. Test Fees Free (no out-of-pocket expenses for those who wish to be tested) Test target Period: Boarding by August 31 Test procedure (Details to be posted on corona.go.jp, etc.) Targets: Passengers traveling from Haneda, Narita, Chubu, Itami, Kansai ①Testing at airport booths (Quantitative antigen test. Results are available and Fukuoka airports to airports in Hokkaido and Okinawa Prefectures, in around 30 minutes on the day of boarding. Reservation required) Hiroshima Airport, Fukuoka Airport and Kagoshima Airport, who wish to ②Testing at stores (Saliva PCR test. Please book well in advance so that be tested. you will be notified of the results before your flight date.) *In case of early morning flights, you may be asked to take the test the evening before, and in case of late evening flights, you may be asked to take the test by the evening of the same day. ③Test kit delivery (Saliva PCR test. Please apply well in advance so that you can receive the results before your flight date.) *If you are tested positive, you will not be allowed to board. ① Testing at airport booths ② Testing at stores ③ Test kit delivery Store of Govt. contracted Govt. contracted testing vendor testing vendor In In Test kit advance advance Result notification Airport booth of delivery Result notification Test at store Govt. -

Recommended Flight Routes to the Conference Venue
Recommended Flight Routes to the Conference Venue Seoul, Shanghai Two flights / week Paris, London, Frankfurt, L.A., San Francisco, Seoul, ICRERA 2012 Nagasaki Bangkok, Beijing, Nagasaki Conference Venue Hong Kong, Kuala Tokyo Airport Lumpur, Hong Kong, Int’l Singapore, etc. Narita Airport Int’l (Haneda) Most of Int’l Cities 1hour Airport 2 hours 65‐85 min Seoul, Busan, Shanghai, Beijing, 10 min Taipei, Bangkok, Takaramachi Stop JR Takaramachi Stop Hanoi, Manila, Fukuoka Nagasaki Dalian, Singapore, Airport Hong Kong, Ho Chi 140 min Station Minh, Jeju, etc. 5min (1) Flying directly to Nagasaki Airport Direct but infrequent flights to Nagasaki Airport are available only from Seoul (Incheon) and Shanghai (Pudong), but not everyday. Please make sure the flight schedule if you can find convenient ones. (2) Connecting at Tokyo International Airport (Haneda) If you are thinking of taking a connecting flight to Nagasaki, flying via Tokyo International Airport (Haneda) is most recommended. You can directly fly to Haneda Airport from more than 10 major cities around the world, and can easily connect to frequent domestic flights to Nagasaki Airport. Flight time between Haneda and Nagasaki is approximately two hours. (3) Connecting at Narita International Airport The other international airport in the Tokyo area is Narita International Airport (formerly also known as New Tokyo International Airport). While Narita International Airport handles more international air traffic than Haneda Airport, any connecting flights to Nagasaki Airport are NOT available. Thus, you need to take a limousine bus to Haneda Airport for connection. The buses depart every 20 minutes and the ride takes 65 to 85 minutes. -

Road to Ichinobo, Matsushima from Tokyo and Sendai
Road to Matsushima CASE (A): Sendai airport (SDJ) Sendai sta. Matsushima SDJ Immigration at Narita International airport Domestic flight Arrive at Sendai airport (SDJ) Train #1 to Sendai station (Sendai Airport Line) Change train at Sendai station Train #2 to Matsushima station (JR Tohoku line) Arrive at Matsushima station Bus or TAXI or Walk NRT Tokyo Ichinobo (venue) HND CASE (B1): Narita airport (NRT) Sendai sta. Matsushima SDJ Immigration at Narita International airport Train #1 to Tokyo station (JR Narita Express) Change train at Tokyo station Train #2 to Sendai station (JR Tohoku Shinkansen) Change train at Sendai station Train #3 to Matsushima station (JR Tohoku line) Arrive at Matsushima station Bus or TAXI or Walk NRT Tokyo Ichinobo (venue) HND CASE (B2): Narita airport (NRT) Sendai sta. Matsushima SDJ Immigration at Narita International airport Train #1 to Ueno station (Keisei SKY liner) Change train at Ueno station (10 min. walk) Train #2 to Sendai station (JR Tohoku Shinkansen) Change train at Sendai station Train #3 to Matsushima station (JR Tohoku line) Arrive at Matsushima station Bus or TAXI or Walk NRT Tokyo Ichinobo (venue) HND CASE (C): Haneda airport (HND) Sendai sta. Matsushima SDJ Immigration at Haneda International airport Train #1 to Hamamatsucho station (Tokyo monorail) Change train at Hamamatsucho station Train #2 to Tokyo station (JR Yamanote line) Change train at Tokyo station Train #3 to Sendai station (JR Tohoku Shinkansen) Change train at Sendai station Train #4 to Matsushima station (JR Tohoku line) NRT Tokyo Arrive at Matsushima station HND Bus or TAXI or Walk Ichinobo (venue) Sendai station Time table Sendai station (Saturday and Holiday) Tohoku Line for Matsushima mark does not stop at Matsushima station.