Case: 1:17-Md-02804-DAP Doc #: 1026 Filed: 10/05/18 1 of 236. Pageid #: 24910
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
1835. EXECUTIVE. *L POST OFFICE DEPARTMENT
1835. EXECUTIVE. *l POST OFFICE DEPARTMENT. Persons employed in the General Post Office, with the annual compensation of each. Where Compen Names. Offices. Born. sation. Dol. cts. Amos Kendall..., Postmaster General.... Mass. 6000 00 Charles K. Gardner Ass't P. M. Gen. 1st Div. N. Jersey250 0 00 SelahR. Hobbie.. Ass't P. M. Gen. 2d Div. N. York. 2500 00 P. S. Loughborough Chief Clerk Kentucky 1700 00 Robert Johnson. ., Accountant, 3d Division Penn 1400 00 CLERKS. Thomas B. Dyer... Principal Book Keeper Maryland 1400 00 Joseph W. Hand... Solicitor Conn 1400 00 John Suter Principal Pay Clerk. Maryland 1400 00 John McLeod Register's Office Scotland. 1200 00 William G. Eliot.. .Chie f Examiner Mass 1200 00 Michael T. Simpson Sup't Dead Letter OfficePen n 1200 00 David Saunders Chief Register Virginia.. 1200 00 Arthur Nelson Principal Clerk, N. Div.Marylan d 1200 00 Richard Dement Second Book Keeper.. do.. 1200 00 Josiah F.Caldwell.. Register's Office N. Jersey 1200 00 George L. Douglass Principal Clerk, S. Div.Kentucky -1200 00 Nicholas Tastet Bank Accountant Spain. 1200 00 Thomas Arbuckle.. Register's Office Ireland 1100 00 Samuel Fitzhugh.., do Maryland 1000 00 Wm. C,Lipscomb. do : for) Virginia. 1000 00 Thos. B. Addison. f Record Clerk con-> Maryland 1000 00 < routes and v....) Matthias Ross f. tracts, N. Div, N. Jersey1000 00 David Koones Dead Letter Office Maryland 1000 00 Presley Simpson... Examiner's Office Virginia- 1000 00 Grafton D. Hanson. Solicitor's Office.. Maryland 1000 00 Walter D. Addison. Recorder, Div. of Acc'ts do.. -

INTERIOR BOARD of INDIAN APPEALS Kickapoo Tribe Of
INTERIOR BOARD OF INDIAN APPEALS Kickapoo Tribe of Indians of the Kickapoo Reservation in Kansas v. Southern Plains Regional Director, Bureau of Indian Affairs 42 IBIA 258 (03/29/2006) United States Department of the Interior OFFICE OF HEARINGS AND APPEALS INTERIOR BOARD OF INDIAN APPEALS 801 NORTH QUINCY STREET SUITE 300 ARLINGTON, VA 22203 KICKAPOO TRIBE OF INDIANS OF : Order Affirming Decision THE KICKAPOO RESERVATION : IN KANSAS, : Appellant, : : v. : Docket No. IBIA 04-98-A : SOUTHERN PLAINS REGIONAL : DIRECTOR, BUREAU OF INDIAN : AFFAIRS, : Appellee. : March 29, 2006 The Kickapoo Tribe of Indians of the Kickapoo Reservation in Kansas (Tribe) seeks review of an April 2, 2004 decision of the Southern Plains Regional Director, Bureau of Indian Affairs (Regional Director; BIA), in which the Regional Director concluded that BIA was not statutorily required to accept certain property in trust for the Tribe. The property at issue consists of three tracts of land, consisting of 74.81 acres, more or less, located in Brown County, Kansas. The property is generally referred to as the “Highway 75 (Simon) tract.” For the reasons discussed below, we affirm the Regional Director’s decision. Background On January 5, 1979, the United States Court of Claims awarded judgment to the Tribe in Indian Claims Commission Docket No. 315, see The Kickapoo Tribe of Kansas, The Kickapoo Tribe of Oklahoma v. United States, 219 Ct. Cl. 719, 618 F.2d 119 (1979), and Congress subsequently appropriated funds to pay the judgment. As required by the Indian Tribal Judgment Funds Use or Distribution Act, 25 U.S.C. -

To: Chairman Lance Kinzer and Members of the House Judiciary Committee
To: Chairman Lance Kinzer And Members of the House Judiciary Committee From: Steve Cadue Tribal Chairman Kickapoo Tribe in Kansas 1107 Goldfinch Road Horton, Kansas 66439 Re: HB 2553 – Nemaha-Brown Watershed Funding Bill Date: February 29, 2012 Good afternoon Chairman Kinzer and Members of the House Judiciary Committee. I am Steve Cadue, Tribal Chairman of the sovereign Kickapoo Nation and I appear before you today to oppose HB 2553. I am opposed to the continuing damaging effort of the Nemaha Brown Watershed District to prevent the Kickapoo Tribe of securing a safe and dependable water supply. Water is life and yes, for the Kickapoo people it is a matter of Life or Perish. We depend on water for a total life-sustaining need including drinking water, health conditions and spiritual blessings. Our Kickapoo people utilized and are dependent on water before the coming of the white man. The United States Supreme Court, Winters v. United States (1908) cited Indian tribal rights original use of water and declared Indian tribe’s use of water before the coming of the white man. Our Kickapoo treaty is the Supreme Law of the Land and is under the protection of the federal trust responsibility of the United States to Indian tribes. Water is a sacred element in our Kickapoo traditions. Water is life. Our Kickapoo tribal reservation homeland is a federally recognized reservation and exists due to treaty agreements with the United States of America. We settled in the land that was called the Kansas territory in the treaty of l832 on the western banks of the Missouri river at Leavenworth. -
AIHREA2012 Annual Report
AIHREA The American Indian Health Education is important and we we have established an academic Research & Education Alliance want to increase the number of pipeline to improve the educational (AIHREA) is an alliance of organi- American Indians entering the attainment of all American Indians. zations whose mission is to partner health professions and conducting We have scholarships available and collaborate with American health research. To meet this goal, to help! Indian peoples, Nations, communi- ties, and organizations to improve the physical, mental, emotional, and spiritual wellbeing of American Indians throughout the United States through quality participatory research and education. The two primary organizations involved are the Center for American Indian Community Health (CAICH) at the University of Kansas Medical Center and the Center for American Indian Studies (CAIS) at AIHREA Collaborators: Johnson County Community American Indian Council, Inc. College. We partner and collabo- Cheyenne River Sioux Tribe Title 1 Program rate with numerous other organiza- Chickasaw Nation tions, conducting research with and Children's Mercy Hospital Center for Environmental Health providing services to the American Choctaw Nation of Oklahoma Indian community in the Denver Indian Health and Family Resources Heartland and around the country. First Nations Student Association (University of Kansas) We use community-based partic- Haskell Indian Nations University Iowa Tribe of Kansas and Nebraska ipatory research (CBPR) in all of Kansas City Indian Center our studies. CBPR is a type of Kickapoo Diabetes Coalition research that involves community Kickapoo Head Start members in all parts of the research Kickapoo Tribe in Kansas process. Almost 80% of our team Minnesota Indian Women's Resource Center members are American Indians Oglala Lakota Nation from many different Nations across Omaha Tribe of Nebraska Ponca Tribe of Nebraska the United States. -

The Modoc Nation (Formerly Known As the “Modoc Tribe”), A
The Modoc Nation (formerly known as the “Modoc Tribe”), a federally recognized native nation by virtue of the Lakes Treaty of 1864 and the Klamath Tribe Restoration Act of 1986 We can no longer tolerate outright refusal of protecting our best interest. If the current conditions were to continue the outright extermination of our people would be complete. Our Ancestral land and water rights will be non- existent and we will be unable to hunt fish and gather as we have always done since time immemorial. We have always been the Modoc Tribe of Northern California and Southern Oregon. We have always been a separate tribe, we were never a band of the Klamath’s and we have never relinquished our Federal Recognition. Our Tribe existed long before there was a California or Oregon. Our tribe is a Federally Recognized Tribe, instead of taking things out of context and stating we are not separate from the Klamath Tribe. (Although the short terminology refers to the Klamath Tribe or Tribes, the long definition has always stated 3 separate tribes in all treaties). There is the Modoc Tribe of Oklahoma, who was forced there not by choice and chose to stay rather than be forced to live with the Klamath tribe. There are Modocs enrolled in the Klamath Tribe(s) as “Klamath”, since the Klamath tribe refuses to acknowledge the Modoc tribe (except when there is financial gain by using our name). We represent all Modoc people of Northern California and Southern Oregon who are enrolled in The Modoc Nation as “Modoc” as we are the Modoc Tribe who have existed in our Ancestral Homelands for over fourteen thousand years or more. -
National Register Nomination
NPS Form 10-900 OMB No. 1024-0018 United States Department of the Interior Listed in the National Park Service National Register June 27, 2016 National Register of Historic Places Registration Form This form is for use in nominating or requesting determinations for individual properties and districts. See instructions in National Register Bulletin, How to Complete the National Register of Historic Places Registration Form. If any item does not apply to the property being documented, enter "N/A" for "not applicable." For functions, architectural classification, materials, and areas of significance, enter only categories and subcategories from the instructions. Place additional certification comments, entries, and narrative items on continuation sheets if needed (NPS Form 10-900a). 1. Name of Property Historic name Iowa Tribe Community Building Other names/site number KHRI # 013-238 Name of related Multiple Property Listing New Deal-Era Resources of Kansas 2. Location th Street & number 330 Road not for publication City or town White Cloud X vicinity State Kansas Code KS County Brown Code 013 Zip code 66094 3. State/Federal Agency Certification As the designated authority under the National Historic Preservation Act, as amended, I hereby certify that this x nomination _ request for determination of eligibility meets the documentation standards for registering properties in the National Register of Historic Places and meets the procedural and professional requirements set forth in 36 CFR Part 60. In my opinion, the property x_ meets _ does not meet the National Register Criteria. I recommend that this property be considered significant at the following level(s) of significance: national statewide x local Applicable National Register Criteria: x A B C ___D See file. -

In the Recent Dear Colleague Letter 99-30, OCSE Notified You of A
Location Codes Workgroup FIPS Coding Scheme Recommendation Summary Position 1 Position 2 Positions 3-5 Interstate Case FIPS State Identifier County/Functional Entity 9 0 BIA Tribe Identifier Tribal Case (Federally recognized) 8 0 ISO Country Identifier International Case Exception 0-9, A-Z (Canada – sub- jurisdiction) Tribal and International Case Location Codes 1 OCSE Case Locator Code Data Standards Tribal locator codes coding scheme Tribal Case Locator Codes • Classification code - 9 in position 1 • “0”(zero) in position 2 • Tribe Identification - BIA code in positions 3-5 Example: Chickasaw Nation 90906 • Addresses for tribal grantees– provided by tribes to IRG staff List of current tribal grantees: http://ocse.acf.hhs.gov/int/directories/index.cfm?fuseaction=main.tribalivd • Link to tribal government addresses web site: http://www.doi.gov/leaders.pdf 11/15/2006 2 OCSE Case Locator Code Data Standards Tribal Identification Codes Code Name 001 Eastern Band of Cherokee Indians of North Carolina 006 Onondaga Nation of New York 007 St. Regis Band of Mohawk Indians of New York 008 Tonawanda Band of Seneca Indians of New York 009 Tuscarora Nation of New York 011 Oneida Nation of New York 012 Seneca Nation of New York 013 Cayuga Nation of New York 014 Passamaquoddy Tribe of Maine 018 Penobscot Tribe of Maine 019 Houlton Band of Maliseet Indians of Maine 020 Mashantucket Pequot Tribe of Connecticut 021 Seminole Tribe of Florida, Dania, Big Cypress, Brighton, Hollywood & Tampa Reservations 026 Miccosukee Tribe of Indians of Florida 027 Narragansett -

Indian Lands of Federally Recognized Tribes of the United States
132°W 131°W 130°W 129°W 128°W 127°W 126°W 125°W 124°W 123°W 122°W 121°W 120°W 119°W 118°W 117°W 116°W 115°W 114°W 113°W 112°W 111°W 110°W 109°W 108°W 107°W 106°W 105°W 104°W 103°W 102°W 101°W 100°W 99°W 98°W 97°W 96°W 95°W 94°W 93°W 92°W 91°W 90°W 89°W 88°W 87°W 86°W 85°W 84°W 83°W 82°W 81°W 80°W 79°W 78°W 77°W 76°W 75°W 74°W 73°W 72°W 71°W 70°W 69°W 68°W 67°W 66°W 65°W 64°W 63°W 48°N 46°N 47°N Neah Bay 4 35 14 45°N Everett 46°N Taholah CANADA Seattle Nespelem 40 Aberdeen 44°N Wellpinit Browning Spokane 45°N Harlem Belcourt WAS HIN Box Wagner E GTO Plummer Elder IN N MA 10 Pablo E SUPER Wapato IO Poplar K R Toppenish A 43°N New L Town Fort Totten Red Lake NT 44°N O Lapwai RM Portland VE Sault MO Sainte Marie NTANA Cass Lake Siletz Pendleton 42°N K NH NORTH DAKOTA Ashland YOR EW 43°N Warm N Springs LA KE No H r Fort U t Yates Boston hw Billings R TS e Crow ET 41°N s Agency O S t HU Worcester O R N AC RE eg Lame Deer OTA NTARIO SS GON io MINNES E O MA 42°N n Sisseton K A Providence 23 Aberdeen L N I 39 Rochester R A Springfield Minneapolis 51 G Saint Paul T SIN I C WISCON Eagle H 40°N IDA Butte Buffalo Boise HO C I 6 41°N R M o E cky M SOUTH DAKOTA ou K AN ntai ICHIG n R A M egion Lower Brule Fort Thompson L E n Grand Rapids I io New York g 39°N e Milwaukee R Fort Hall R west 24 E d Detroit Mi E 40°N Fort Washakie K WYOMING LA Rosebud Pine Ridge Cleveland IA Redding Wagner AN Toledo LV 32 NSY PEN Philadelphia 38°N Chicago NJ A 39°N IOW Winnebago Pittsburgh Fort Wayne Elko 25 Great Plains Region Baltimore Des Moines MD E NEBRASKA OHIO D -

EMS P- *Treaties: Tribes
DOCUMENT RESUME 310 175 612 RC 011 603 TITLE Beyond Bows and Arrows. Resource Manual. INSTITUTION Civil Service Commission, Washington, D. C. Bureau of Intergovernaental Personaal Programs. PUB DATE Nay 79 NOTE 148p.; Prepared for the Dallas Region "Symposium on the American Indian" EMS P- E OF01 Plus Postage. PC Not Available from EDRS. DESCRIL 1S American History: *American Indian Culture: American Indian Education: *American Indians: Civil Rights: Education: Employment: Federal Government: *Federal Indian Relationship: *Government Role: Health: Housing: Population Trends: Reservations (Indian): *Treaties: Tribes IDENTIFIMIS *American Irlian History: Bureau of Indian Affairs: Cultural Contributions ABSTRACT In spite of their visible prominence and influence on almost emery aspect of our society, Aserican Indians remain theleast understood group of people. To acquaint symposium participantswith the American Indian and to produce greater understanding,this resource manual docuaents the historical treatmentand present status of Indians. Presented are: the constitutional status ofAmerican Indians, including soarces of federal power, tribalsovereignty, , powers of tribal self-government, hunting andfishing rights, domestic relations, taxation, legal statas of Indian individuals, constitutional immunity, the 1968 Indian Bill of Rights, rights and privileges of state citizenship, and wardship:American Indian tribes, Eskimo and Aleut groups for which the Bureau of Indian Affairs has responsibility: federal Indian policiesfrom the colonial period through the early 19701s: administrators of U.S. Federal Indian Policy: Cosmissioners of Indian Affairs from 1832 tothe present: important dates in federal Indian relationships:labor statistics: employment: education: health: relevance of Indianlife %* civilisation: housing: Indian population byregions: location of Adian lands and communities: and Indian tribes andorganization, including names and addresses of each leader. -

2010 Census CPH-T-6. American Indian and Alaska Native Tribes in the United States and Puerto Rico: 2010
2010 Census CPH-T-6. American Indian and Alaska Native Tribes in the United States and Puerto Rico: 2010 Description of Table 1. This table shows data for American Indian and Alaska Native tribes alone and alone or in combination for the United States. Those respondents who reported as American Indian or Alaska Native only and one tribe are shown in Column 1. Respondents who reported two or more American Indian or Alaska Native tribes, but no other race, are shown in Column 2. Those respondents who reported as American Indian or Alaska Native and at least one other race and one tribe are shown in Column 3. Respondents who reported as American Indian or Alaska Native and at least one other race and two or more tribes are shown in Column 4. Those respondents who reported as American Indian or Alaska Native in any combination of race(s) or tribe(s) are shown in Column 5, and is the sum of the numbers in Columns 1 through 4. For a detailed explanation of the alone and alone or in combination concepts used in this table, see the 2010 Census Brief, “The American Indian and Alaska Native Population: 2010” at <www.census.gov/prod/cen2010/briefs/c2010br-10.pdf>. Table 1. American Indian and Alaska Native Population by Tribe1 for the United States: 2010 Source: U.S. Census Bureau, 2010 Census, special tabulation. Internet release date: December 2013 Note: Respondents who identified themselves as American Indian or Alaska Native were asked to report their enrolled or principal tribe. Therefore, tribal data in this data product reflect the written tribal entries reported on the questionnaire. -

Supp 5 Title III and Title VI
ACL State by State Total for Covid Supplement #5 Consolidated Appropriations Act, 2021 supplemental funding for the OAA nutrition program under Title III-C2 of the Older Americans Act State Part C2. Home Meals Alabama $2,528,346 Alaska $840,000 Arizona $3,786,823 Arkansas $1,536,749 California $17,520,720 Colorado $2,569,933 Connecticut $1,890,526 Delaware $840,000 Dist. of $840,000 Columbia Florida $12,750,236 Georgia $4,604,882 Hawaii $840,000 Idaho $862,415 Illinois $6,145,904 Indiana $3,264,441 Iowa $1,635,969 Kansas $1,421,264 Kentucky $2,249,141 Louisiana $2,239,417 Maine $843,890 Maryland $2,906,228 Massachusetts $3,500,618 Michigan $5,303,695 Minnesota $2,775,861 Mississippi $1,457,813 Missouri $3,165,493 Montana $840,000 Nebraska $930,790 Nevada $1,471,240 New Hampshire $840,000 New Jersey $4,439,739 New Mexico $1,087,189 New York $9,810,549 North Carolina $5,202,534 North Dakota $840,000 Ohio $6,136,966 Oklahoma $1,890,839 Oregon $2,241,513 Pennsylvania $7,099,301 Rhode Island $840,000 South Carolina $2,755,035 South Dakota $840,000 Tennessee $3,406,138 Texas $11,414,900 Utah $1,104,103 Vermont $840,000 Virginia $4,077,856 Washington $3,628,725 West Virginia $1,072,295 Wisconsin $3,061,217 Wyoming $840,000 American $105,000 Samoa Guam $420,000 Northern $105,000 Marianas Puerto Rico $1,918,707 Virgin Islands $420,000 Total $168,000,000 Supplemental funding for the OAA nutrition and supportive services programs under the authority of OAA Title VI, Parts A & B Tribe State Tribe Name Total Award AK Aleutian Pribilof Islands Association, Inc. -
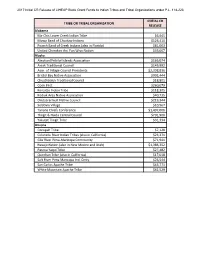
Initial CR Release of LIHEAP Block Grant Funds to Indian Tribes and Tribal Organizations Under P.L
2017 Initial CR Release of LIHEAP Block Grant Funds to Indian Tribes and Tribal Organizations under P.L. 114-223 INITIAL CR TRIBE OR TRIBAL ORGANIZATION RELEASE Alabama Ma-Chis Lower Creek Indian Tribe $6,945 Mowa Band of Choctaw Indians $126,410 Poarch Band of Creek Indians (also in Florida) $81,003 United Cherokee Ani-Yun Wiya Nation $33,007 Alaska Aleutian/Pribilof Islands Association $166,074 Aniak Traditional Council $149,992 Assn. of Village Council Presidents $2,398,836 Bristol Bay Native Association $902,444 Chuathbaluk Traditional Council $18,801 Cook Inlet $260,079 Kenaitze Indian Tribe $118,305 Kodiak Area Native Association $40,735 Orutsararmuit Native Council $219,344 Seldovia Village $10,967 Tanana Chiefs Conference $1,497,006 Tlingit & Haida Central Council $701,900 Yakutat Tlingit Tribe $31,334 Arizona Cocopah Tribe $7,128 Colorado River Indian Tribes (also in California) $23,271 Gila River Pima-Maricopa Community $71,941 Navajo Nation (also in New Mexico and Utah) $1,386,352 Pascua Yaqui Tribe $27,482 Quechan Tribe (also in California) $17,018 Salt River Pima Maricopa Ind. Cmty. $26,544 San Carlos Apache Tribe $43,771 White Mountain Apache Tribe $62,529 2017 Initial CR Release of LIHEAP Block Grant Funds to Indian Tribes and Tribal Organizations under P.L. 114-223 INITIAL CR TRIBE OR TRIBAL ORGANIZATION RELEASE California Berry Creek Rancheria $5,358 Big Valley Band of Pomo Indians $1,443 Bishop Paiute $20,194 Coyote Valley Pomo Band $4,451 Enterprise Rancheria $2,061 Hoopa Valley Tribe $36,927 Hopland Band $5,605 Karuk Tribe $26,789 Mooretown Rancheria $15,290 N.