Seasonal Malaria Chemoprevention Coverage Survey, Guinea, 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Quarterly Progress Report on U.S. Government International Ebola Response and Preparedness Activities
USAID Office of HHS Office of Inspector General Inspector General Quarterly Progress Report on U.S. Government International Ebola Response and Preparedness Activities Fiscal Year 2016, First Quarter | December 31, 2015 An Ebola response team from the Bong County Ebola treatment unit educates a town in Bong Mines, Liberia about Ebola. (Morgana Wingard for USAID, October 9, 2015) QUARTERLY REPORT ON EBOLA RESPONSE AND PREPAREDNESS ACTIVITIES Quarterly Progress Report on U.S. Government International Ebola Response & Preparedness December 31, 2015 FISCAL YEAR 2016, FIRST QUARTER ii QUARTERLY REPORT ON EBOLA RESPONSE AND PREPAREDNESS ACTIVITIES TABLE OF CONTENTS Executive Summary 1 Ebola Outbreak in West Africa 2 U.S. Government Response to the Ebola Outbreak 3 Funding Response, Preparedness, and Recovery Efforts 4 U.S. Government Efforts to Control the Outbreak 10 Transition from Response to Recovery 14 U.S. Government Recovery Efforts to Mitigate Second-Order Impacts 14 Food Security 14 Health Systems and Critical Non-Ebola Health Services 16 Governance and Economic Crisis Mitigation 19 Innovation and Communication Technology 20 U.S. Government Efforts to Strengthen Global Health Security 21 Oversight Activities 23 U.S. Agency for International Development OIG 24 Department of Health and Human Services OIG 27 Department of Defense OIG 28 Department of State OIG 29 Department of Homeland Security OIG 30 Government Accountability Office 30 Investigations 30 Appendix A: Telected Ebola Diagnostic Tools and Medical Countermeasures Supported by U.S. Government Agencies 31 Appendix B: USAID Ebola-related Programs by Pillar and Geographical Focus as of December 31, 2015 (Unaudited) 33 Appendix C: Acronyms 59 Appendix D: Endnotes 61 FISCAL YEAR 2016, FIRST QUARTER iii Children and families waiting to be screened at the Ola Children’s Hospital in Freetown, Sierra Leone. -

Emergency Appeal Operation Update Ebola Virus Disease Emergency Appeals (Guinea, Liberia, Sierra Leone and Global Coordination & Preparedness)
Emergency Appeal Operation Update Ebola Virus Disease Emergency Appeals (Guinea, Liberia, Sierra Leone and Global Coordination & Preparedness) Combined Monthly Ebola Operations Update No 281 15 December 2015 Current epidemiological situation + country-specific information The spread of Ebola in West Africa has slowed intensely, but enormous challenges remain in conquering this scourge while re-establishing basic social services and building resilience in Guinea, Liberia and Sierra Leone. This unparalled outbreak has hit some of the most vulnerable communities in some of the world’s poorest countries. School children practicing proper handwashing before classes begin in Montserrado, Liberia in October 2015. LNRCS supported by IFRC has been distributing handwashing kits, soap, chlorine and no-touch thermometers to over On 20 November 2015, the Government 500 schools across the country. Photo: IFRC of Liberia confirmed three new cases of IFRC’s Ebola virus disease (EVD) strategic framework is organised around five Ebola from a family of six living in an area outcomes: of Monrovia. All the cases were transferred to an Ebola Treatment Unit (ETU). One of 1. The epidemic is stopped; the three confirmed cases, a boy, died on 2. National Societies (NS) have better EVD preparedness and stronger long-term capacities; 23 November. His brother and father continued with the treatment. 3. IFRC operations are well coordinated; 4. Safe and Dignified Burials (SDB) are effectively carried out by all actors; 5. Recovery of community life and livelihoods. There have not been any additional/new Helping stop the epidemic, the EVD operations employ a five pillar approach confirmed cases so far. A total of 166 comprising: (i) Beneficiary Communication and Social Mobilization; (ii) Contact contacts related to the current cluster were Tracing and Surveillance; (iii) Psychosocial Support; (iv) Case Management; and (v) Safe and Dignified Burials (SDB) and Disinfection; and the revision has listed and continued with daily follow-up. -

UN EBOLA RESPONSE MPTF ANNUAL PROJECT NARRATIVE REPORT Year: ___2017______
UN EBOLA RESPONSE MPTF ANNUAL PROJECT NARRATIVE REPORT Year: ___2017________ Project Number and Title: PROJECT START AMOUNT RECIPIENT #65- Enhancing the post-Ebola national DATE1: ALLOCATED by ORGANIZATION preparedness capacity to efficiently 30-08-2017 MPTF UNDP, UNFPA, respond to future health outbreaks (please indicate different Project ID: 00106881 (Gateway ID) UNICEF, WHO, WFP tranches if applicable) $2,500,000 UNICEF: $446,033 UNDP: $795,031 UNFPA: $446,757 IMPLEMENTING WFP: $188,146 PARTNER(S): WHO: $624,033 Ministry of Health and Project Focal Point: EXTENSION DATE: FINANCIAL Public Hygiene Name: Theoneste Ganza N/A COMMITMENTS Ministry of Local Crisis Recovery/Humanitarian Administration and Coordination Specialist, RCO UNICEF: 125,500 US$ Decentralization UNDP: 0 US$ (MATD) Tel. +224 624 76 41 74 UNFPA: 208,724 US$ E-mail: [email protected] National Public Health WFP: 0 US$ Security Agency (ANSS) WHO: 0 US$ International Strategic Objective (STEPP) PROJECTED END EXPENDITURES Organization for SO5 – Prevent Outbreaks in countries DATE: as of [01/01/2018] Migrations (OIM)- not currently affected Recovery UNICEF: 134,285 US$ Central Pharmacy of 31-08-2018 Strategic Objectives UNDP: 175,857 US$ Guinea (PCG) RSO# - Description UNFPA: 0 US$ Ministry of Internal WFP: 0 US$ Security/Department of WHO: 60,000 US$ Civil Protection Ministry of Environment/National Mission Critical Action Center for MCA13 – Multi-faceted preparedness Environmental Risk Management Location: Sub-National Coverage Areas: Guinea nationwide All the 38 prefectures of Guinea Report Submitted by: Report Cleared by: o Name: Theoneste Ganza o Name: (Head of Agency): Lionel Laurens, Country Director o Title: Crisis Recovery Specialist o Date of Submission: 21-03-2018 o Date of Submission: 17-03-2018 o Participating Organization (Lead): UNDP o Participating Organization (Lead): UNDP o Email address: [email protected] o Email address: [email protected] 1 The date project funds were first transferred. -

Usaid/Guinea Annual Report Fy 2002
USAID/GUINEA ANNUAL REPORT FY 2002 March 2002 Please Note: The attached RESULTS INFORMATION is from the FY 2002 Annual report, and was assembled and analyzed by the country or USAID operating unit identified on the cover page. The Annual Report is a “pre-decisional” USAID document and does not reflect results stemming from formal USAID review(s) of this document. Related document information can be obtained from: USAID Development Experience Clearinghouse 1611 N. Kent Street, Suite 200 Arlington, VA 22209-2111 Telephone: 703/351-4006 Ext. 106 Fax: 703/351-4039 Email: [email protected] Internet: http://www.dec.org Released on or after July 1, 2002 3 Annual Report Part III: Performance Narrative A. Challenges and Responses: In addition to successfully responding to a formidable set of development conditions, USAID’s Guinea program was further challenged this year as the impact of the cross-border conflicts that continued into 2001 played out. Implementing partners working in the conflict- affected areas rapidly regrouped to mobilize resources to either start up in other parts of Guinea, or to concentrate efforts in other existing intervention zones. While the negative impacts of the disruption on achievements could not be avoided in all instances, significant results were nonetheless achieved in each Strategic Objective (SO) area and, overall, the program is on track. Encouraged by a successful formal Country Strategy Program mid-term review held in Washington, management attention turned to more closely aligning the program to the Global Pillars. To this end, working groups were established to more clearly reflect conflict prevention, HIV/AIDS and economic growth in current activities. -

Modeling Spatial Invasion of Ebola in West Africa
Modeling Spatial Invasion of Ebola in West Africa Jeremy P D'Silvay and Marisa C. Eisenbergyz y Department of Epidemiology, School of Public Health, University of Michigan, Ann Arbor, z Department of Mathematics, University of Michigan, Ann Arbor Address correspondence to: [email protected]. Abstract The 2014-2015 Ebola Virus Disease (EVD) epidemic in West Africa was the largest ever recorded, representing a fundamental shift in Ebola epidemiology with unprecedented spatiotemporal complex- ity. We developed spatial transmission models using a gravity-model framework to explain spatiotem- poral dynamics of EVD in West Africa at both the national and district-level scales, and to compare effectiveness of local interventions (e.g. local quarantine) and long-range interventions (e.g. border- closures). Incorporating spatial interactions, the gravity model successfully captures the multiple waves of epidemic growth observed in Guinea. Model simulations indicate that local-transmission re- ductions were most effective in Liberia, while long-range transmission was dominant in Sierra Leone. The model indicates the presence of spatial herd protection, wherein intervention in one region has a protective effect on surrounding regions. The district-level intervention analysis indicates the pres- ence of intervention-amplifying regions, which provide above-expected levels of reduction in cases and deaths beyond their borders. The gravity-modeling approach accurately captured the spatial spread patterns of EVD at both country and district levels, and helps to identify the most effective locales for intervention. This model structure and intervention analysis provides information that can be used by public health policymakers to assist planning and response efforts for future epidemics. -
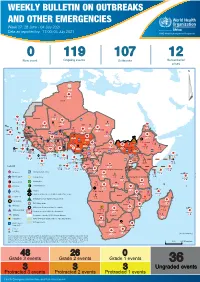
04 July 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 27: 28 June - 04 July 2021 Data as reported by: 17:00; 04 July 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 119 107 12 New event Ongoing events Outbreaks Humanitarian crises 64 0 141 471 3 755 Algeria ¤ 1 008 0 6 116 181 Mauritania 14 449 527 48 0 110 0 43 768 1 174 Niger 21 076 489 6 088 25 Mali 21 0 9 0 Cape Verde 6 471 16 4 951 174 Chad Eritrea Senegal 5 506 194 Gambia 66 0 32 705 287 1 414 8 Guinea-Bissau 847 17 Burkina Faso 2 060 56 276 435 4 331 167 859 2 121 Guinea 13 494 168 13 0 3 881 69 2 2 Benin 198 0 Nigeria 1 189 4 61 0 30 0 Ethiopia 13 2 6 995 50 556 5 872 15 Sierra Leone Togo 626 0 80 858 1 324 Ghana 7 141 98 Côte d'Ivoire 10 879 117 19 000 304 81 0 45 0 Liberia 17 0 South Sudan Central African Republic 1 313 2 0 25 0 50 14 0 96 317 796 6 738 221 Cameroon 23 807 294 3 0 48 594 315 35 173 196 7 0 58 0 199 2 1 411 30 9 1 620 1 185 868 3 675 2 0 168 0 1 1 5 748 104 14 069 131 2 0 8 759 122 Equatorial Guinea Uganda 867 2 827 9 Sao Tome and Principe 4 0 4 520 133 78 394 903 Kenya Gabon Legend Congo 3 307 90 305 26 Rwanda 8 199 104 2 376 37 42 585 470 25 076 159 Democratic Republic of the Congo 12 790 167 Burundi Measles Humanitarian crisis 5 521 8 Seychelles 42 181 960 435 0 693 57 Monkeypox Yellow fever United Republic of Tanzania 197 0 16 259 57 Meningitis Lassa fever 509 21 241 1 6 257 229 Leishmaniasis Cholera 95 703 913 164 282 2 443 Comoros Plague 304 3 cVDPV2 Angola Malawi Diarrhoeal disease in children under five years 36 926 1 208 726 0 3 -

Ethnic Marginalization and (Non)Compliance in Public Health Emergencies
Ethnic Marginalization and (Non)Compliance in Public Health Emergencies Leonardo R. Arriola Allison N. Grossman [email protected] [email protected] Associate Professor PhD Candidate Department of Political Science Department of Political Science University of California Berkeley University of California Berkeley Forthcoming in the Journal of Politics ABSTRACT Health crises can reveal the inability of governments to induce compliance with policy interventions. While lack of compliance is conventionally attributed to individual mistrust in government, resistance to such interventions is often found clustered among entire communities, particularly in ethnically divided societies. We account for such patterns by explaining how citizens adjust their responses to state authority according to their shared ethnicity with those in power. We assess the effect of ethnicity on citizen compliance with a public health advisory on HIV/AIDS issued by different authority types through a survey-based field experiment in the West African country of Guinea. Members of a politically marginalized ethnic group, the Peul, are significantly less likely to comply with a public health advisory from a national government representative, the president, when compared to local or religious leaders. We show that perceived ethnic discrimination conditions both trust in and compliance with different authority types. KEYWORDS Public Health, Political Marginalization, Ethnicity, HIV Authors are listed in alphabetical order and contributed equally to the project. We are grateful for financial support from the West African Research Association. This research was approved by the UC Berkeley Office for the Protection of Human Subjects under protocol number 2016-04-8721. The pre-analysis plan for this project is registered at the Evidence in Governance and Politics (EGAP) design registry under protocol ID 20160907AA. -

Une Subvention D'un Montant De GNF 12 778 665
ARRETE Article 1er: Une subvention d’un montant de GNF 12 778 665 750 (Douze milliards sept cent soixante dix huit millions six cent soixante cinq mille sept cent cinquante Francs Guinéens) est accordée aux Collectivités Décentralisées du Ministère de l’Administration du Territoire et de la Décentralisation, au titre du 1er trimestre de l’exercice 2017. Article 2: La subvention visée à l’article 1er du présent arrêté, servira à couvrir les dépenses liées au fonctionnement desdites Collectivités et sera virée dans les comptes des Communes urbaines et rurales conformément à l’état de ventilation ci-après: N° Désignation Banques MONTANTS I- REGION DE CONAKRY 437 500 000 1 1 C.U KALOUM BCRG 87 500 000 2 2 C.U DIXINN BCRG 87 500 000 3 3 C.U MATAM BCRG 87 500 000 4 4 C.U MATOTO BCRG 87 500 000 5 5 C.U RATOMA BCRG 87 500 000 II - REGION DE BOKE 356 250 000 6 1. C.U BOKE BICIGUI 75 000 000 7 1 BINTIMODIA BICIGUI 31 250 000 8 2 DABISS BICIGUI 31 250 000 9 3 KAMSAR BICIGUI 31 250 000 10 4 KANFARANDE BICIGUI 31 250 000 11 5 KOLABOUI BICIGUI 31 250 000 12 6 MALAPOUYAH BICIGUI 31 250 000 13 7 SANGAREDI BICIGUI 31 250 000 14 8 SANSALE BICIGUI 31 250 000 15 9 TANENE BICIGUI 31 250 000 2. C.U BOFFA 281 250 000 16 C.U BOFFA SGBG 62 500 000 17 1 KOLIAH BICIGUI 31 250 000 18 2 DOUPROU SGBG 31 250 000 19 3 KOBA BICIGUI 31 250 000 20 4 LISSO BICIGUI 31 250 000 21 5 MANKOUNTAN BICIGUI 31 250 000 +224 654 00 11 11 / +224 661 00 11 11 - Conakry, République de Guinée - BP : 519 www.mbudget.gov.gn 22 6 TAMITA BICIGUI 31 250 000 23 7 TOUGNIFILY BICIGUI 31 250 000 3. -

The Africa Solidarity Trust Fund (ASTF)
Africa Solidarity Trust Fund (ASTF) Transforming resources into development solutions Final report 2014–2018 Africa Solidarity Trust Fund (ASTF) Transforming resources into development solutions Final report 2014–2018 Food and Agriculture Organization of the United Nations Rome, 2019 Required citation: FAO. 2019. Africa Solidarity Trust Fund (ASTF). Transforming resources into development solutions. Final report 2014–2018. Rome. 84 pp. Licence: CC BY-NC-SA 3.0 IGO. The designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations (FAO) concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or products of manufacturers, whether or not these have been patented, does not imply that these have been endorsed or recommended by FAO in preference to others of a similar nature that are not mentioned. The views expressed in this information product are those of the author(s) and do not necessarily reflect the views or policies of FAO. © FAO, 2019 Some rights reserved. This work is made available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo/legalcode/legalcode). Under the terms of this licence, this work may be copied, redistributed and adapted for non-commercial purposes, provided that the work is appropriately cited. In any use of this work, there should be no suggestion that FAO endorses any specific organization, products or services. -

Page 1 S.NO Sub-Prefecture Non 00 10 17 18 Alassoya Albadaria
S.No Sub-prefecture 1 Alassoya 2 Albadaria 3 Arfamoussaya 4 Babila 5 Badi 6 Baguinet 7 Balaki 8 Balandougou 9 Balandougouba, Kankan 10 Balandougouba, Siguiri 11 Balato 12 Balaya 13 Balizia 14 Banama 15 Banankoro 16 Banfélé 17 Bangouyah 18 Banguingny 19 Banian 20 Banié 21 Banko 22 Bankon 23 Banora 24 Bantignel 25 Bardou 26 Baro 27 Bate-Nafadji 28 Beindou, Faranah 29 Beindou, Kissidougou 30 Benty 31 Beyla-Centre 32 Bheeta 33 Bignamou 34 Binikala 35 Bintimodiya 36 Bissikrima 37 Bodié 38 Boffa-Centre 39 Bofossou 40 Boké-Centre 41 Bolodou 42 Boola 43 Bossou 44 Boula 45 Bouliwel 46 Bounouma www.downloadexcelfiles.com 47 Bourouwal 48 Bourouwal-Tappé 49 Bowé 50 Cisséla 51 Colia 52 Coyah-Centre 53 Dabiss 54 Dabola-Centre 55 Dalaba-Centre 56 Dalein 57 Damankanyah 58 Damaro 59 Daralabe 60 Daramagnaky 61 Daro 62 Dialakoro, Faranah 63 Dialakoro, Kankan 64 Diara-Guerela 65 Diari 66 Diassodou 67 Diatiféré 68 Diécké 69 Dinguiraye-Centre 70 Dionfo 71 Diountou 72 Ditinn 73 Dixinn 74 Dogomet 75 Doko 76 Donghol-Sigon 77 Dongol-Touma 78 Douako 79 Dougountouny 80 Dounet 81 Douprou 82 Doura 83 Dubréka-Centre 84 Fafaya 85 Falessade 86 Fangamadou 87 Faralako 88 Faranah-Centre 89 Farmoriah 90 Fassankoni 91 Fatako 92 Fello-Koundoua 93 Fermessadou-Pombo www.downloadexcelfiles.com 94 Firawa 95 Forécariah-Centre 96 Fouala 97 Fougou 98 Foulamory 99 Foumbadou 100 Franwalia 101 Fria-Centre 102 Friguiagbé 103 Gadha-Woundou 104 Gagnakali 105 Gama 106 Gaoual-Centre 107 Garambé 108 Gayah 109 Gbakedou 110 Gbangbadou 111 Gbessoba 112 Gbérédou-Baranama 113 Gnaléah 114 Gongore -

Guinea-Bissau " 0 0 ' ' 0 0 ° ° 2 2 1 1
G U I N E A - B O K E R E G I O N f h Logistics and Health Facilities Overview as of 13 February 2015 SENEGAL Sambailo Youkounkoun N N " " 0 0 ' ' 0 0 3 3 ° Koundara ° 2 2 1 1 Koundara Kamaby Guingan KOUNDARA Termesse Touba Foulamory Bafata MALI N N " GUINEA-BISSAU " 0 0 ' ' 0 0 ° ° 2 2 1 1 Dougountouny Kounsitel Koumbia Gaoual Linsan BOKE GAOUAL LABE Manda Tyanguel-Bori Touba N N " " 0 0 ' ' 0 0 3 3 ° ° 1 1 1 Malanta Djountou 1 Wendou M'Bour Balaya Lelouma Parawol LABE Deliganjan Kakony LELOUMA Kandiafara Timbi Madina BOKE Sangaredi Wuansa Diaga, N N " " 0 TELIMELE Sogorayah 0 ' Touma Misside ' 0 0 ° ° 1 1 1 Donghol 1 BARALANDE Ley Miro Boke Danton Pellel Telimele MAMOU PITA Kamsar Tonkoya Madina N Toumbeta N " " 0 0 ' ' 0 Songoron 0 3 3 ° ° 0 0 1 FRIA 1 Sokoutou Dankharan Khissling Fria Balandougou Donde BOFFA FRIA Bel-Air KINDIA Boffa Sougeta DUBREKA Koulente KINDIA Koluhare Koubia Siguiton Maleya Wassou Kindia N N " " 0 0 ' Damakania ' 0 0 ° Segueya ° 0 Koab 0 1 1 Toureya Saboya Friguibe SENEGAL Koliagbe Bamako !. Camara-Bouyni GUINEA-BISSAU Gbnkli MALI !. Mambya LABE Dubreka BOKE Kouryia ± Balahn Gomokouri 0 12.5 25 50 COYAH MAMOU Coyah FARANAH KANKAN Kilometers CONAKRY KINDIA CONAKRY GF Ebola Treatment Unit, Open .! National Capital (!o International Airport Highway International boundary Sekourou ConakCryO!.NAKRY Louis Pasteur b WFP Country Office (! Major Town o Domestic Airport Primary Road Region boundary / National Reference CONAKRY Lab o N !( N " k WFP Sub Office Intermediate Town Airstrip Secondary Road Prefecture boundary " 0 0 ' FORECARIAH ' 0 0 3 3 ° Conakry ° 9 !. -

Région De Boké 2018
REPUBLIQUE DE GUINEE Travail - Justice- Solidarité MINISTERE DU PLAN ET DU DEVELOPPEMENT ECONOMIQUE La région de Boké en chiffres Edition 2020 GEOGRAPHIE ET ORGANISATION ADMINISTRATIVE Géographie 0rganisation administrative en 2018 5 préfectures ; 32 sous-préfectures ; 5 communes urbaines, Superficie = 31 207 km2 394 districts/quartiers ; 2 045 secteurs 32 communes rurales Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) Préfectures Sous-préfectures Boffa Colia Douprou, Koba-Tatema, Lisso, Mankountan, Tamita, Tougnifili Boké Bintimodya, Dabiss, Kamsar, Kanfarande, Kolaboui, Malapouyah, Sangaredi, Sansale, Tanènè Fria Baguinet, Banguingny, Tormelin Gaoual Foulamory, Kakony, Koumbia, Kounsitel, Malanta, Touba, Wendou M'bour Koundara Guingan, Kamaby, Koundara-, Sambailo, Sareboido, Termesse, Youkounkou Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) STATISTIQUES DEMOGRAPHIQUES Populations des RGPH 1983 1996 2014 Population région de Boké 508 724 760 119 1 083 147 Population de la principale préfecture : Boké 168 924 293 917 450 278 Part de la population nationale en 2014 : 10,3 % Rang régional en 2014 : 5/8 Sources : Institut national de la statistique/RGPH Population au 1er juillet 2016 2017 2018 Population région de Boké 1 157 540 1 190 724 1 224 571 Sources : Institut national de la statistique (Perspectives démographiques de la Guinée, décembre 2017) STATISTIQUES SUR LES CONDITIONS DE VIE DES MENAGES 1994/1995