Zimbabwe Developing Subnational Estimates of Hiv Prevalence and the Number of People
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Midlands Province
School Province District School Name School Address Level Primary Midlands Chirumanzu BARU KUSHINGA PRIMARY BARU KUSHINGA VILLAGE 48 CENTAL ESTATES Primary Midlands Chirumanzu BUSH PARK MUSENA RESETTLEMENT AREA VILLAGE 1 MUSENA Primary Midlands Chirumanzu BUSH PARK 2 VILLAGE 5 WARD 19 CHIRUMANZU Primary Midlands Chirumanzu CAMBRAI ST MATHIAS LALAPANZI TOWNSHIP CHIRUMANZU Primary Midlands Chirumanzu CHAKA NDARUZA VILLAGE HEAD CHAKA Primary Midlands Chirumanzu CHAKASTEAD FENALI VILLAGE NYOMBI SIDING Primary Midlands Chirumanzu CHAMAKANDA TAKAWIRA RESETTLEMENT SCHEME MVUMA Primary Midlands Chirumanzu CHAPWANYA HWATA-HOLYCROSS ROAD RUDUMA VILLAGE Primary Midlands Chirumanzu CHIHOSHO MATARITANO VILLAGE HEADMAN DEBWE Primary Midlands Chirumanzu CHILIMANZI NYONGA VILLAGE CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHIMBINDI CHIMBINDI VILLAGE WARD 5 CHIRUMANZU Primary Midlands Chirumanzu CHINGEGOMO WARD 18 TOKWE 4 VILLAGE 16 CHIRUMANZU Primary Midlands Chirumanzu CHINYUNI CHINYUNI WARD 7 CHUKUCHA VILLAGE Primary Midlands Chirumanzu CHIRAYA (WYLDERGROOVE) MVUMA HARARE ROAD WASR 20 VILLAGE 1 Primary Midlands Chirumanzu CHISHUKU CHISHUKU VILAGE 3 CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHITENDERANO TAKAWIRA RESETTLEMENT AREA WARD 11 Primary Midlands Chirumanzu CHIWESHE PONDIWA VILLAGE MAPIRAVANA Primary Midlands Chirumanzu CHIWODZA CHIWODZA RESETTLEMENT AREA Primary Midlands Chirumanzu CHIWODZA NO 2 VILLAGE 66 CHIWODZA CENTRAL ESTATES Primary Midlands Chirumanzu CHIZVINIRE CHIZVINIRE PRIMARY SCHOOL RAMBANAPASI VILLAGE WARD 4 Primary Midlands -

MASHONALAND EAST PROVINCE - Basemap
MASHONALAND EAST PROVINCE - Basemap Mashonaland Central Karanda Chimandau Guruve MukosaMukosa Guruve Kamusasa Karanda Marymount Matsvitsi Marymount Mary Mount Locations ShinjeShinje Horseshoe Nyamahobobo Ruyamuro RUSHINGA CentenaryDavid Nelson Nyamatikiti Nyamatikiti Province Capital Nyakapupu M a z o w e CENTENARY Mazowe St. Pius MOUNT DARWIN 2 Chipuriro Mount DarwinZRP NyanzouNyanzou Mt Darwin Chidikamwedzi Town 17 GoromonziNyahuku Tsakare GURUVE Jingamvura MAKONDE Kafura Nyamhondoro Place of Local Importance Bepura 40 Kafura Mugarakamwe Mudindo Nyamanyora Chingamuka Bure Katanya Nyamanyora Bare Chihuri Dindi ARDA Sisi Manga Dindi Goora Mission M u s e n g e z i Nyakasoro KondoKondo Zvomanyanga Goora Wa l t o n Chinehasha Madziwa Chitsungo Mine Silverside Donje Madombwe Mutepatepa Nyamaruro C o w l e y Chistungo Chisvo DenderaDendera Nyamapanda Birkdale Chimukoko Nyamapanda Chindunduma 13 Mukodzongi UMFURUDZI SAFARI AREA Madziwa Chiunye KotwaKotwa 16 Chiunye Shinga Health Facility Nyakudya UZUMBA MARAMBA PFUNGWE Shinga Kotwa Nyakudya Bradley Institute Borera Kapotesa Shopo ChakondaTakawira MvurwiMvurwi Makope Raffingora Jester H y d e Maramba Ayrshire Madziwa Raffingora Mvurwi Farm Health Scheme Nyamaropa MUDZI Kasimbwi Masarakufa Boundaries Rusununguko Madziva Mine Madziwa Vanad R u y a Madziwa Masarakufa Shutu Nyamukoho P e m b i Nzvimbo M u f u r u d z i Madziva Teacher's College Vanad Nzvimbo Chidembo SHAMVA Masenda National Boundary Feock MutawatawaMutawatawa Mudzi Rosa Muswewenhede Chakonda Suswe Mutorashanga Madimutsa Chiwarira -

School Level Province District School Name School Address Secondary
School Level Province District School Name School Address Secondary Midlands Chirumanzu CHAMAKANDA LYNWOOD CENTER TAKAWIRA RESETTLEMENT Secondary Midlands Chirumanzu CHENGWENA RAMBANAPASI VILLAGE, CHIEF HAMA CHIRUMANZU Secondary Midlands Chirumanzu CHISHUKU VILLAGE 2A CHISHUKU RESETLEMENT Secondary Midlands Chirumanzu CHIVONA DENHERE VILLAGE WARD 3 MHENDE CMZ Secondary Midlands Chirumanzu CHIWODZA VILLAGE 38 CHIWODZA RESETTLEMENT MVUMA Secondary Midlands Chirumanzu CHIZHOU WARD 5 MUZEZA VILLAGE, HEADMAN BANGURE , CHIRUMANZU Secondary Midlands Chirumanzu DANNY DANNY SEC Secondary Midlands Chirumanzu DRIEFONTEIN DRIEFONTEIN MISSION FARM Secondary Midlands Chirumanzu GONAWAPOTERA CHAKA BUSINESS CENTRE MVUMA MASVINGO ROAD Secondary Midlands Chirumanzu HILLVIEW HILLVIEW VILLAGE1, LALAPANZI Secondary Midlands Chirumanzu HOLY CROSS HOLY CROSS MISSION WARD 6 CHIRUMANZU Secondary Midlands Chirumanzu LALAPANZI 42KM ALONG GWERU-MVUMA ROAD Secondary Midlands Chirumanzu LEOPOLD TAKAWIRA LEOPOLD TAKAWIRA 2KM ALONG CENTRAL ESTATES ROAD Secondary Midlands Chirumanzu MAPIRAVANA MAPIRAVANA VILLAGE WARD 1CHIRUMANZU Secondary Midlands Chirumanzu MUKOMBERANWA MUWANI VILLAGE HEADMAN MANHOVO Secondary Midlands Chirumanzu MUSENA VILLAGE 8 MUSENA RESETTLEMENT Secondary Midlands Chirumanzu MUSHANDIRAPAMWE RUDHUMA VILLAGE WARD 25 CHIRUMANZU Secondary Midlands Chirumanzu MUTENDERENDE DZORO VILLAGE CHIEF HAMA Secondary Midlands Chirumanzu NEW ENGLAND LOVEDALE FARMSUB-DIVISION 2 MVUMA Secondary Midlands Chirumanzu ORTON'S DRIFT ORTON'S DRIFT FARM Secondary Midlands -

Midlands ZIMBABWE POPULATION CENSUS 2012
Zimbabwe Provincial Report Midlands ZIMBABWE POPULATION CENSUS 2012 Population Census Office P.O. Box CY342 Causeway Harare Tel: 04-793971-2 04-794756 E-mail: [email protected] Census Results for Midlands Province at a Glance Population Size Total 1 614 941 Males 776 787 Females 838 154 Annual Average Increase (Growth Rate) 2.2 Average Household Size 4.5 1 2 Table of Contents Table of Contents...............................................................................................................................3 List of Tables.....................................................................................................................................4 Foreword ...........................................................................................................................................9 Executive Summary.........................................................................................................................10 Midlands Fact Sheet (Final Results) .................................................................................................13 Chapter 1: ........................................................................................................................................14 Population Size and Structure .......................................................................................................14 Chapter 2: ........................................................................................................................................24 Population Distribution -

National Rapid Response Team Contacts
National Rapid Response Team Contacts City/Town Contact Person Mobile Number Toll free Number Institution/Role Ace Ambulance +263 782999901-4 (0) 8080412 Harare ZRP (0242) 777777 ZRP Harare - Wilkins (0242) 741872 Wilkins Hosp Harare - Wilkins (0242) 740404 Wilkins Hosp Harare Dr Chonzi +263 712860777 Harare Dr Bara +263 734322293 Harare Dr Mudariki +263 772974314 Bulawayo Ms Sibanda +263 772677476 Bulawayo Dr Nyathi +263 776248128 Bulawayo Dr Ncube +263 772424812 Bulawayo Dr E Sibanda +263 772880581 Director Health Services Bulilima Dr Hapanyengwi +263 772907621 Beitbridge Dr Samhere +263 772386895 Bindura Mr Karisa +263 773271670 DMO Bikita Dr Mungwari +263 715411650 Centenary/Muzarabani Mr Kangundu +263 777366045 DNO Chegutu Dr Masvosva +263 772720190 Chiredzi Dr Dhlandhlara +263 775094360 Chirumanzu Dr S Maunga +263 772286685 (0) 8080435 Chirumanzu Mr Mukomberanwa +263 773 394 154 (0) 8080435 Chirumanzu Sr Mutumwa +263 772 911 454 (0) 8080435 Concession Dr Sosera +263 774736753 Gokwe North DR Chikara +263 775 428800 Gokwe North E Muchenje +263772 575437 City/Town Contact Person Mobile Number Toll free Number Institution/Role Gokwe South DR Mashoko +263 774 074739 Gokwe South D Mukotsi +263 774 002 934 Goromonzi Dr Karim +263 772347378 Guruve Zvomuya +263 772641444 DNO Gwanda Dr Gwarimbo +263 775735679 Gweru Dr Mhene +263 773258210 (0) 8080435 Gweru Provincial Hosp Toll free +263 787822276 (0) 8080435 Gweru Provincial Hospital Gweru& City G Shariwa +263 773 639 797 (0) 8080435 Gweru& City Mr Sekanhamo +263 715017014 (0) 8080435 Gweru& -

Zimbabwe Lean Season Assistance – Januar Y - Apr Il 2021
Zimbabwe Lean Season assistance – Januar y - Apr il 2021 This map aims to represent the level of achievement related to food assistance response for the period Jan-Apr 2021. The selection of the period derives from two major factors: 1) data are available for all actors, and 2) the period coincides with the peak and end of the lean season response plan of major aid agencies. The gradient of the colours shows the ratio of the achievement at district level, calculated considering all beneficiaries reached against the estimation of people in need elaborated in October 2020, and according to the following criteria: People reached:for each agency, it was considered the maximum number of beneficiaries reported in any month. This is because food assistance is supposed to operate by monthly cycle for the same households being served every month of the programme. Both government and non-governmental agencies, including the UN, are included in this map. People in need:it was used the estimation of people in need from the ZimVAC rural assessment, and the WFP CARI report for the urban areas. This choice was made in order to consider all people in need who were supposed to be reached by the implementation of all programmes. Mbire Hurungwe Centenary/ Muzarabani Kariba Urban Mount Rushinga Guruve Darwin Karoi Kariba Bindura Mvurwi Mudzi Mashonaland Shamva Mashonaland West Chinhoyi Bindura Urban UMP East Makonde Mazowe Mutoko Gokwe North Zvimba Goromonzi Harare Binga Harare Murehwa Victoria Chegutu NortonHarare Rural Falls Sanyati Chitungwiza Gokwe Chegutu -

From Blood Diamonds to Blood Gold - a Report on Machete Violence in Zimbabwe’S ASM Gold Sector Introduction
Center for Natural Resources Governance ISSUE 01 Thursday 30 July 2020 www.cnrgzim.org From Blood Diamonds to Blood Gold - A report on machete violence in Zimbabwe’s ASM gold sector Introduction Contributors • Farai Maguwu • Simiso Mlevu • Tapuwa O’bren Nhachi • Henry Nyapokoto Centre for Natural Resource Governance Tel: +263715387417/+263718365908 Email: [email protected] www.cnrgzim.org Twitter @CNRG_ZIM Introduction hurugwi is a beautiful scenic town in Zimbabwe`s Midlands Province which sits on the famous mineral rich Great Dyke belt. A drive through the small town justifies why Zimbabweans believe their country is the most beautiful in the world. The Great Dyke, which is up to 8 miles wide and about 330 miles long, consists of Sseveral precious minerals which include gold, silver, chromium, platinum, and nickel. Other types of minerals include but not limited to mica, asbestos, and tin. It is almost as if Shurugwi enjoys an unfair advantage over other towns in Zimbabwe. However, before the Covid-19 induced lockdown, the name Shurugwi was the subject of a violent narrative sweeping over the country’s mining sector; a phenomenon of terror synonymous with towns and communities where artisanal gold mining is done. Since then, Zimbabwe’s gold mining communities in particular, have been living in fear of terror gangs whose modus operandi is said to have originated in the Midlands Province, which is the place where Shurugwi is found. The term “MaShurugwi,” as Machete violence gangs are being called, has become a codename describing a group of young and middle-aged men and, in some instances women, unleashing a reign of terror in gold mining communities. -

MASVINGO PROVINCE - Basemap
MASVINGO PROVINCE - Basemap Mashonaland East Mpinda Musuma Msilahove Ntabamhlope Ntabamhlope 30 Hunters Mlezu 19 27 Chikwava 8 Munyanyi Chipfatsura Mushunje Rowa 6 C h i c a m b a e a l 3 Road 15 31 4 33 R 25 23 12 Lancashire Chipwanya 1 31 13 Gunde Chapwanya 10 15 Burma Madilisa Nkululeko Connemara Murezi Mombeyarara 4 Gunde Central Garamwera Bepe 2 11 Valley Locations Nyama Masvori Chirinda 12 14 Connemara St Patricks Estates 8 14 CHIKOMBA 2 11 Chiweshe Zumbare KWEKWE 7 12 7 Nyama 12 Gombe 13 Chiwenga 9 Berzerly 9 St. Muchakata 13 Maburutse 3 Matanda Bridge 11 St. Gwindingwi 10 3 Patricks Chiundura 5 Makumbe Richards Marange Madhikani 16 Murambinda Nyashanu Bazeley Province Capital 2 Maboleni Marange 24 7 Mvuma 24 Nyashanu Murambinda Nyashanu 18 Bridge 20 Mambwere Maboleni 2 Nerutanga 10 Mvuma 13 Denhere 8 O Cambrai 20 Bakorenhema Athens d Netherburn N y a m a f u f u 36 21 4 z Broadside Buhera Nhamo i Chitora Chipendeke s 15 Lalapanzi d 22 Buhera 18 Nyangani Zvipiripiri 17 Chikwariro 19 Chitora BANTI n 6 Lalapanzi 6 14 Town a 17 Mtao Bambazonke l W h i t e w a t e r Whahwa 16 Bwizi O 5 1 Mudanda 20 Nzvenga d d Fairfield z i Gutaurare Lower i Hlabano Mangwande Insukamini Dambara Betera 26 Mpudzi M Gweru 8 16 14 1 I n s u k a m i n i BUHERA MUTARE Muromo 19 4 Mudanda 22 Makepesi O M Vungu Sino Rukundo 11 Lynwood Driefontein Nyazvidzi Viriri 17 23 Place of Local Importance Lower 25 d Zimbabwe Driefontein St Andrews z 27 a Gweru Welcome i n Totonga Isolation 1 Nyazvidzi i Muwonde Felixburg 16 Madzimbashuro Zvipiripiri Masasi c Soti a Mkoba -
Zimbabwe Program Map 2/19/09
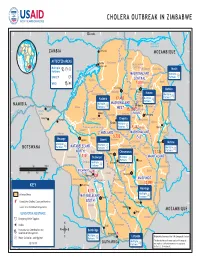
CHOLERA OUTBREAK IN ZIMBABWE 24° 25° 26° 27° 28° Lusaka 29° 30° 31° 32° 33° 34° K afue ezi Z mb am a b Z è Albufeira de z Cahora Bassa e 16° ZAMBIA Chirundu MOZAMBIQUE 16° Guruve i n AFFECTED AREAS Kariba Hurungwe a y Muzarambani Kariba Dam n u (centenary) Multiple H Mt Darwin Rushinga Mudzi Partners B aJ Lake Kariba S MASHONALANDMASHONALAND Multiple a n Partners J UNICEF y a a Kariba t CENTRALCENTRAL Z i 17° a Shamva Mudzi 17° m WHO 7,200 b B D e Bindura U.M.P. z Chinhoyi i Mbare Mutoko Makonde Bindura Zvimba Harare Gokwe North Mutoko Multiple Kadoma 17,483 Multiple Partners J Harare Partners J Nyanga Multiple MASHONALANDMASHONALAND NAMIBIA Harare Victoria Falls Binga Partners J WESTWEST Murehwa e 15,1587Goromonzi b G ho Victoria M 18° C w u 18° i Gokwe n HARAREHARARE nt Falls a y Chegutu Marondera y Kadoma a at y i i in Matetsi Seke L Hwange Gokwe South Chegutu Marondera Sengwa Makoni Kadoma Multiple Partners J 5,412 Wedza Nyanga Lupane i Sh z angani MIDLANDSMIDLANDS MASHONALANDMASHONALAND d Mutasa Hwange S O a 5,732 v Nkayi EASTEAST e Hwange Lupane Gweru Kwekwe 19° Chikomba Mutare Mutare 19° Multiple Multiple Chirumanzu BOTSWANA Partners J MATABELELANDMATABELELAND Partners J Buhera Mutare MultipleLago Gweru PartnersChicamba J NORTHNORTH Bubi Chirumanzu 11,124 Gweru Gutu Tsholotsho 1,110 Bulawayo Multiple MANICALANDMANICALAND G w Partners J M Gutu a Umguza u y Multiple Shurugwi i t i Partners Shurugwi r 0 50 100 mi J i k Chimanimani a w Nat BULAWAYOBULAWAYO i Bikita 7 R 20° 0 50 100 150 km u 20° Insiza n d Masvingo Bulawayo 439 e zi MASVINGOMASVINGO Bu Bulalimamangwe Umzingwane Zvishavane Rio Chivi Zaka e Chipinge 10,053 v Plumtree a KEY S Masvingo Masvingo 5,171 Mberengwa Affected Areas Multiple MATABELELANDMATABELELAND Gwanda Partners J Cumulative Cholera Cases per Province SOUTHSOUTH Triangle 21°# 21° S Matobo Source: U.N. -

MIDLANDS PROVINCE - Basemap
MIDLANDS PROVINCE - Basemap Mashonaland West Chipango Charara Dunga Kazangarare Charara Hewiyai 8 18 Bvochora 19 9 Ketsanga Gota Lynx Lynx Mtoranhanga Chibara 2 29 Locations A Chitenje 16 21 R I B 4 K A CHARARA 7 Mpofu 23 K E 1 Kachuta 4 L A 12 SAFARI Kapiri DOMA 1 Kemutamba Mwami Kapiri Chingurunguru SAFARI Kosana Guruve AREA Mwami Kapiri Green Matsvitsi Province Capital Mwami Mwami Bakwa AREA Valley 5 Guruve 6 KARIBA 26 Kachiva 1 Doro Shinje Nyaodza Dora Kachiva Shinje Ruyamuro B A R I Masanga Nyamupfukudza 22 Nyama A Nyamupfukudza C e c i l m o u r 22 Town E K Kachekanje Chiwore 18 Nyakapupu K Masanga Doma 2 7 L A Gache- Kachekanje Masanga 23 Lan Doma 3 Gatse Gache lorry 5 Doma Gatse Masanga B l o c k l e y Chipuriro 2 Maumbe Maumbe Rydings GURUVE Bumi 16 Maumbe Hills Gachegache Chikanziwe 8 Kahonde Garangwe Karoi 15 Place of Local Importance Magwizhu Charles Lucky Chalala Tashinga Kareshi Crown 5 Mauya 10 11 Clarke 7 10 3 Mauya Chalala Charles Nyangoma 11 1 Karambanzungu Chitimbe Clarke Magunje 8 Nyamhondoro Hesketh Bepura Chalala Kabvunde KAROI URBAN Mugarakamwe Karambanzungu Magunje Magunje Hesketh Nyangoma Mhangura 9 Kudzanai Army Government Ridziwi Mudindo Nyamhunga Sikona ARDA 9 Mission Nyamhunga Mahororo Charles Chisape HURUNGWE Mhangura Sisi MATUSADONA Murapa Sengwe Dombo Madadzi Nyangoma Mhangura 12 Clack Karoi Katenhe Arda Kanyati Nyamhunga Enterprise Tategura Mhangura NATIONAL 17 Kapare Katenhe Karoi Mine Mhangura Sisi Mola Makande Nyadara Muitubu Mola Nyamhunga 10 Enterprise 14 Mola PARK Makande 11 Mhangura Ramwechete 11 -

Zimbabwe News, Vol. 19, No. 8
Zimbabwe News, Vol. 19, No. 8 http://www.aluka.org/action/showMetadata?doi=10.5555/AL.SFF.DOCUMENT.nuzn198808 Use of the Aluka digital library is subject to Aluka’s Terms and Conditions, available at http://www.aluka.org/page/about/termsConditions.jsp. By using Aluka, you agree that you have read and will abide by the Terms and Conditions. Among other things, the Terms and Conditions provide that the content in the Aluka digital library is only for personal, non-commercial use by authorized users of Aluka in connection with research, scholarship, and education. The content in the Aluka digital library is subject to copyright, with the exception of certain governmental works and very old materials that may be in the public domain under applicable law. Permission must be sought from Aluka and/or the applicable copyright holder in connection with any duplication or distribution of these materials where required by applicable law. Aluka is a not-for-profit initiative dedicated to creating and preserving a digital archive of materials about and from the developing world. For more information about Aluka, please see http://www.aluka.org Zimbabwe News, Vol. 19, No. 8 Alternative title Zimbabwe News Author/Creator Zimbabwe African National Union Publisher Zimbabwe African National Union (Harare, Zimbabwe) Date 1988-08-00 Resource type Magazines (Periodicals) Language English Subject Coverage (spatial) Zimbabwe, South Africa Coverage (temporal) 1988 Source Northwestern University Libraries, L968.91005 Z711 v.19 Rights By kind permission of ZANU, the Zimbabwe African National Union Patriotic Front. Description Editorial: 1. 2. Comment. Letters. Department of External Affairs — ZANU (PF). -

The Mineral Industry of Zimbabwe in 2016
2016 Minerals Yearbook ZIMBABWE [ADVANCE RELEASE] U.S. Department of the Interior February 2020 U.S. Geological Survey The Mineral Industry of Zimbabwe By James J. Barry Zimbabwe’s real gross domestic product (GDP) increased Production by 2.3% in 2016 compared with a 0.6% rate of growth in 2015. The real GDP at market prices was about $14.2 billion in 2016. In 2016, production for a number of mineral commodities Zimbabwe’s mineral output included an estimated 7.8% of the increased owing largely to higher global prices, including world’s platinum production, an estimated 5.7% of the world’s production of nitrogen, which increased by 167%; PGMs, 21%; palladium output, and about 1.7% of the world’s diamond cement and cobalt, 15% each; gold and silver, 14% each; copper, production (by weight). The country was the world’s third- 11%; and nickel in concentrate, 10%. Production decreased for ranked producer of platinum, fifth-ranked producer of palladium, the following mineral commodities: coal (bituminous), by 62%; and eighth-ranked producer of diamond. Zimbabwe had the coke, 50%; diamond (gem and industrial), 40%; ferrochromium, world’s third largest platinum-group-metal (PGM) reserves 32%; and graphite, 12%. Reported and estimated production for (Kimberley Process Certification Scheme, 2017; Zimbabwe the other commodities produced was relatively unchanged. Data National Statistics Agency, 2017, p. 21; Loferski, 2018). on mineral production are in table 1. Minerals in the National Economy Structure of the Mineral Industry In 2016, the mining and quarrying sector accounted for about Domestic and international investment companies, domestic 9.9% of real GDP.