Application for Clinical Privileges
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fast Facts Hong Kong
Member Organisation – Fast Facts Hong Kong: Name of Member Organisation Canossa Hospital (Caritas) Location Hong Kong ACHSI Accredited Since September 2011 Website Link http://www.canossahospital.org.hk/ Sector Private Type Hospital Number of Beds 146 Name of Member Organisation Caritas Medical Centre Location Kowloon, Hong Kong ACHSI Accredited Since October 2011 Website Link http://www.ha.org.hk/visitor/ha_hosp_details.asp?C ontent_ID=100163&Lang=ENG Sector Public Type Hospital Number of Beds 1,206 Name of Member Organisation Castle Peak Hospital Location Hong Kong ACHSI Accredited Since August 2014 Website Link http://www3.ha.org.hk/cph/en/ Sector Public Type Hospital Number of Beds 1156 Name of Member Organisation Dental Implant & Maxillofacial Centre DIMFC Location Hong Kong ACHSI Accredited Since January 2016 Website Link http://www.aboc.com.hk/ Sector Private Type Day Procedure Centre Number of Beds N/A Name of Member Organisation Evangel Hospital Location Hong Kong ACHSI Accredited Since April 2014 Website Link http://www.evangel.org.hk/eng/ Sector Private Type Hospital Number of Beds 70 Name of Member Organisation Fresenius Medical Care Hong Kong Limited - NephroCare Tuen Mun Dialysis Clinic (NCTM) Location Tuen Mun, Hong Kong ACHSI Accredited Since July 2015 Website Link http://www.freseniusmedicalcare.com Sector Private Type Day Procedure Centre Number of Beds 15 Updated February 2018 Name of Member Organisation Fresenius Medical Care Hong Kong Limited - NephroCare Wan Chai Dialysis Clinic (NCWC) Location Wan Chai, Hong Kong -

Inauguration of the Provisional HK Academy of Nursing
Inauguration of the Provisional HK Academy of Nursing (Cover) 1 Inauguration Program for The Provisional Hong Kong Academy of Nursing and Academy Colleges of Nursing 12 May 2012 Inauguration of the Provisional HK Academy of Nursing (Inside Cover) 2 Hong Kong College of Cardiac Nursing 香港心臟護士專科學院 Hong Kong College of Community and Public Health Nursing 香港社區及公共健康護理學院 Hong Kong College of Critical Care Nursing 香港危重病護理學院 Hong Kong College of Education and Research in Nursing 香港護理教育及科研學院 Hong Kong College of Emergency Nursing 香港急症科護理學院 Hong Kong College of Gerontology Nursing 香港老年學護理專科學院 Hong Kong College of Medical Nursing 香港內科護理學院 Inauguration of the Provisional HK Academy of Nursing Hong Kong College of Mental Health Nursing 3 香港精神健康護理學院 Hong Kong College of Midwives 香港助產士學院 Hong Kong College of Nursing and Health Care Management Hong Kong College of Orthopaedic Nursing 香港骨科護理學院 Hong Kong College of Paediatric Nursing 香港兒科護理學院 Hong Kong College of Perioperative Nursing 香港圍手術護理學院 Hong Kong College of Surgical Nursing 香港外科護理學院 Inauguration of the Provisional HK Academy of Nursing President Message 4 I am delighted to welcome you all here on this auspicious day of the inauguration of the Provisional Hong Kong Academy of Nursing (the “PHKAN”). It is my great pleasure to celebrate and witness together with you the inauguration of the Academy and its 14 specialty academy colleges, as well as the conferment of honorary/founding fellows and fellows of the Hong Kong Academy of Nursing. The aims of the PHKAN are: (1.) establish the Hong Kong Academy of Nursing as a statutory body to regulate the nursing profession; and (2.) enhance excellence in nursing service and health care in Hong Kong through promotion of specialist nursing education and practices. -

13-1 13 LANDSCAPE and VISUAL IMPACT 13.1 Introduction 13.1.1
Agreement No. CE 35/2006(CE) Kai Tak Development Engineering Study cum Design and Construction of Advance Works Kai Tak Development – Investigation, Design and Construction Environmental Impact Assessment Report 13 LANDSCAPE AND VISUAL IMPACT 13.1 Introduction 13.1.1 This Section outlines the landscape and visual impact assessment associated with the Kai Tak Development in accordance with the EIA Study Brief No. ESB-152/2006, the criteria and guidelines as stated in Annexes 10 and 18 of the TM and EIAO Guidance Note No. 8/2002 on “Preparation of Landscape and Visual Impact Assessment under the Environmental Impact Assessment Ordinance” for evaluating and assessing combined landscape and visual impacts of the Project and associated works. The assessment shall identify, describe and quantify any potential landscape and visual impacts, evaluate the significance of such impacts on sensitive receivers and propose measures to avoid or mitigate these impacts. 13.1.2 This section covers the Schedule 3 LVIA. The following Schedule 2 Designated Projects are identified under the Kai Tak Development: x DP1 - New distributor roads serving the planned KTD, x DP2 - New sewage pumping stations serving the hinterland and the planned KTD, x DP3a - Decommissioning of the remaining parts (Ex-GFS Building and Radar Station) of the former Kai Tak Airport, x DP3b - Decommissioning of the remaining parts (HKAC site and existing EMSD Headquarters) of the former Kai Tak Airport, x DP4 - Decommissioning of the former Kai Tak Airport other than the North Apron, x -

Birth Record
eHR Sharable Data - Birth Record May 2018 © HKSAR Government eHR Sharable Data - Birth Record Form Category 1 Entity Name Entity ID Definition Data Type Data Type Validation Rule Repeated Code Table Remark Data requirement Data requirement Data requirement Example (Certified Example (Certified Example (Certified (code) (description) Data (Certified Level 1) (Certified Level 2) (Certified Level 3) Level 1) Level 2) Level 3) Birth Birth datetime 100310 The birth date or birth datetime of a patient TS Time stamp M M M 11/02/2012 20/12/2011 21:22 09/12/2001 23:59 Record Birth Birth Birth institution code 1003346 [eHR value] of the "Birth institution" code table, to define CE Coded Birth institution NA NA M PMH Record Institution the healthcare institution who reported the birth data to element the Immigration Department Birth Birth Birth institution description 1003107 [eHR description] of the "Birth institution" code table, it ST String Birth institution NA NA M Princess Margaret Record Institution should be the corresponding description of the selected Hospital [Birth institution code]. Birth institution description is to define the healthcare institution who reported the birth data to the Immigration Department. Birth Birth Birth institution local description 1003108 The local description of the healthcare institution who ST String M M M St. Paul Hospital St. Paul Hospital Princess Margaret Record Institution reported the birth data to the Immigration Department. Hospital Birth Birth Birth location code 1003102 [eHR value] of the "Birth location" code table, to define CE Coded Birth location NA NA O BBA Record Location the location where the patient was born element Birth Birth Birth location description 1003103 [eHR description] of the "Birth location" code table, it ST String Birth location NA NA M if [Birth location code] Born before arrival Record Location should be the corresponding description of the selected is given [Birth location code]. -

List of Buildings with Confirmed / Probable Cases of COVID-19
List of Buildings With Confirmed / Probable Cases of COVID-19 List of Residential Buildings in Which Confirmed / Probable Cases Have Resided (Note: The buildings will remain on the list for 14 days since the reported date.) Related Confirmed / District Building Name Probable Case(s) Yau Tsim Mong Grand Austin Block 2 1276 North The Royal Oaks 1276 Yau Tsim Mong Fook Cheung Building 1283 9 cases notified by the Kwai Tsing Dorsett Tsuen Wan Mainland authority Kwun Tong Lai Tat House, On Tat Estate 1289 Wong Tai Sin Choi Wah House, Choi Fai Estate 1291 Sha Tin Tak Wo House, Wo Che Estate 1292 Sha Tin Mei Wo House, Wo Che Estate 1293 Sha Tin Ming Chuen House, Shui Chuen O Estate 1294 Wong Tai Sin Choi Wah House, Choi Fai Estate 1295 Tuen Mun Siu Lung Court 1296 Yau Tsim Mong Cherry Mansion, 39A Oak Street 1297 Yau Tsim Mong Block 3 Hampton Place 1297 No. 6, 8, 10, 12 Po Ming Lane & No. 11 Po Wong Tai Sin 1298 Wai Lane Kwai Tsing Dorsett Tsuen Wan 1299 Kwai Tsing Dorsett Tsuen Wan 1300 Wong Tai Sin Lai Yuen House, Chuk Yuen South Estate 1301 No. 6, 8, 10, 12 Po Ming Lane & No. 11 Po Wong Tai Sin 1302 Wai Lane Wong Tai Sin Choi Wah House, Choi Fai Estate 1304 Kwun Tong Yuk Shek House, Ping Shek Estate 1305 Wong Tai Sin Ching Yuen House, Tsz Ching Estate 1306 No. 6, 8, 10, 12 Po Ming Lane & No. 11 Po Wong Tai Sin 1307 Wai Lane Kwai Tsing Dorsett Tsuen Wan 1309 Wong Tai Sin 5 Tsz Wah Lane 1310 Wong Tai Sin Manning Theatre Building 1311 Wong Tai Sin Block A, Gomme House 1312 1 Related Confirmed / District Building Name Probable Case(s) Tsuen Wan Block 1, Bayview Garden 1313 Yau Tsim Mong Hoi Wen House , Hoi Fu Court 1314 Wong Tai Sin Pik Fung House, Fung Tak Estate 1315 No. -

HOKLAS Accredited Organisations and Scope of Accreditation
Hong Kong Accreditation Service (HKAS) HOKLAS Accredited Organisations and Scope of Accreditation HOKLAS Name of Accredited Laboratory Certificate Reg. No. 001 Government Laboratory - Analytical and Advisory Services Division Download 003 The Hong Kong Standards and Testing Centre Ltd. Download 004 CMA Industrial Development Foundation Limited Download 005 Intertek Testing Services Hong Kong Ltd. Download 006 Sun Creation Engineering Limited - Calibration & Testing Laboratory Download 007 Hong Kong Aircraft Engineering Co. Ltd. - Calibration and Metrology Centre Download 009 SGS Hong Kong Limited Download 010 Civil Engineering and Development Department - Public Works Laboratories Download 011 Concrete Services Limited Download 012 Hong Kong Testing Company Limited Download 015 Fugro Technical Services Limited Download 016 Housing Department - Materials Testing Laboratory Download 019 Quality Control Consultants Ltd. Download 021 Stanger Asia Limited Download 022 ETS-Testconsult Limited Download 024 Geotechnics & Concrete Engineering (Hong Kong) Ltd. Download 026 Labour Department - Occupational Safety and Health Branch - Occupational Hygiene Download Laboratory 028 Soils & Materials Engineering Co. Ltd. Download 030 Chow Sang Sang Jewellery Co. Ltd. - Chow Sang Sang Precious Metal Laboratory Download 032 Castco Testing Centre Ltd. Download 034 Environmental Protection Department - Acoustic Testing Laboratory Download 036 UL VS Hong Kong Limited Download 037 Green Island Cement Company Limited Download 039 Hong Kong Productivity Council -

List of Buildings with Confirmed / Probable Cases of COVID-19
List of Buildings With Confirmed / Probable Cases of COVID-19 List of Residential Buildings in Which Confirmed / Probable Cases Have Resided (Note: The buildings will remain on the list for 14 days since the reported date.) Related Confirmed / District Building Name Probable Case(s) Tsuen Wan Iau Kin Building 11009 Kwun Tong Chi Tai House, On Tai Estate 11010 Kwun Tong Sau Yat House, Sau Mau Ping Estate 11010 Kwun Tong Chi Tai House, On Tai Estate 11011 North On Po Tsuen 11012 Yau Tsim Mong Seawide Mansion 11014 Sai Kung Man Sau Sun Tsuen 11015 Kwai Tsing Lok King House, Lai King Estate 11016 Sham Shui Po Mei Wui House, Shek Kip Mei Estate 11017 Kwai Tsing Kwai On House, Kwai Fong Estate 11019 Matilda International Hospital Domestic Central & Western 11020 Quarters New Lai King Building, 48-56 Choi Hung Wong Tai Sin 11026 Road Kwun Tong Chi Tai House, On Tai Estate 11027 Yau Tsim Mong Cheung Fung Mansion 11028 Yau Tsim Mong Marco Polo Hongkong Hotel 11028 Kwun Tong Sau Hong House, Sau Mau Ping Estate 11029 Tower 7, Hong Kong University of Science Sai Kung 11030 and Technology Senior Staff Quarters Sha Tin Block 10, City One Shatin 11031 Kwun Tong Sau Yat House, Sau Mau Ping Estate 11032 Case notified by the Sai Kung Block 3, Residence Oasis National Health Commission Wong Tai Sin Cambridge Building 11034 Kowloon City Mun Ching House, Kai Ching Estate 11035 Kwai Tsing Block 6, Kwai Shing West Estate 11036 Southern Fu Heng Yuen, Chi Fu Fa Yuen 11038 Sha Tin Kam Lan House, Kam Fung Court 11039 Kowloon City Tower 1, The Zumurud 11040 1 Related -

Hong Kong Island (By Alphabetical Order of Name of Doctor)
Hong Kong Island (By alphabetical order of name of doctor) Service Provider Practice Name and Address District 1. AI, HIU FAY DAWN Chan &Tse Family Medicine Practice CW Room 503, 5/F, Chinachem Tower, 34-37 Connaught Road Central, CENTRAL, HONG KONG 2. AU YEUNG, YING KIT Dr Jeff Au Yeung EAST JEFF Shop U6, Fitfort, 560 King's Road, NORTH POINT, HONG KONG 3. AU, CHI LAP Dr Simon C L Au EAST Shop 2, 36 Hoi Kwong Street, QUARRY BAY, HONG KONG 4. AU -YEUNG, SHIU Dr Au Yeung ShiuHing EAST HING Shop 1, G/F, Yeung On Building, 50-54 Shau Kei Wan Road, SHAU KEI WAN, HONG KONG 5. BALLANTINE, DrVio& Partners CW ALISTAIR NIGEL 3/F, New World Tower 2, 18 Queen's Road Central, CENTRAL, STUART HONG KONG 6. CHAIN, CHI WOO Chains Medicare Centre CW DAVID 15/F, Regent Centre, 88 Queen's Road Central, CENTRAL, HONG KONG 7. CHAN, CHI WANG Dr Chan Chi Wang (Med-Link Medical Centre) WC Shop E, G/F, EIB Tower, 4-6 Morrison Hill Road, WAN CHAI, HONG KONG 8. CHAN, CHO YIN Dr Chan Cho Yin CW Shop B, G/F, New Start Building, 330-336 Queen's Road West, SAI YING PUN, HONG KONG 9. CHAN, FOOK CHUEN Dr Chan FookChuen CW G/F, 1D Sands Street, KENNEDY TOWN, HONG KONG 10. CHAN, HING WAI Hang Seng Medical Practice EAST 114A Shau Kei Wan Road, SHAU KEI WAN, HONG KONG 11. CHAN, HO TING Dr George medical clinics CW Shop 8, Level 1 (Basement), Hong Kong Station, Airport Express, CENTRAL, HONG KONG 12. -

Locations Routes
Location and Route Questions Booklet Amendment Notice The Transport Department has amended the Location and Route Questions Booklet (version of Jan 2020), the following amendment is applicable to test from 1 April 2020 onwards. Locations Location (Question) Place (Answer) 161. Butterfly on Wellington Wellington Street 177. Lan Kwai Fong Hotel @ Kau U Fong Central 181. Hotel Jen Hong Kong Sai Wan 210 The Ritz-Carlton, Hong Kong Austin Road West Routes Start (Question) Destination (Question) Most Direct Viable Route (Answer) Hong Kong Heritage Prosperous Garden, Yau Man Lam Road, Lion Rock Tunnel Road, 400. Lion Rock Tunnel, Waterloo Road, Ferry Museum Ma Tei Street and Public Square Street DRIVING SERVICES SECTION Taxi Written Test - Part B (Location and Route Questions Booklet) Note: This pamphlet is for reference only and has no legal authority. The Driving Services Section of Transport Department may amend any part of its contents at any time as required without giving any notice. 1 Location (Question) Place (Answer) Location (Question) Place (Answer) Hospitals 19. Caritas Medical Centre Cheung Sha Wan Princess Margaret 1. Queen Mary Hospital Pok Fu Lam 20. Lai King Hospital Prince of Wales 2. Sha Tin 21. Kwai Chung Hospital Lai King Hospital 3. Tsan Yuk Hospital Sai Ying Pun 22. Yan Chai Hospital Tsuen Wan United Christian 4. Tung Wah Hospital Sheung Wan 23. Sau Mau Ping Hospital TWGHs Fung Yiu Haven of Hope 5. Pok Fu Lam 24. Tseung Kwan O King Hospital Hospital Wong Chuk Tseung Kwan O 6. Grantham Hospital 25. Po Ning Lane Hang Hospital Pamela Youde A Kung Kok 7. -

Download Settling in Hong Kong
Settling-in Hong Kong 14 What’s Inside? The Basics Let’s Talk About Culture Settling in Tips Let’s Have Fun Need Help? The Basics About Hong Kong Hong Kong (Chinese: 香港), officially the Hong Kong Special Administrative Region of the People's Republic of China, is a special administrative region. With over 7.4 million people of various nationalities in a 1,104 km2 territory, Hong Kong is the world's fourth-most-densely-populated region. Hong Kong became a colony of the British Empire after Qing China ceded Hong Kong Island at the end of the First Opium War in 1842. The colony expanded to the Kowloon Peninsula in 1860 after the Second Opium War and was further extended when Britain obtained a 99-year lease of the New Territories in 1898. The territory was returned to China when the lease expired in 1997. As a special administrative region, Hong Kong's system of government is separated from that of mainland China. Formerly a sparsely populated area of farming and fishing villages, Hong Kong has become one of the world's most significant financial centers and commercial ports. It is the world's seventh-largest trading entity, and its legal tender (the Hong Kong dollar) is the world's 13th-most-traded currency. Although the city has one of the highest per capita incomes in the world, it has severe income inequality. The territory has the largest number of skyscrapers in the world, most surrounding Victo- ria Harbour. Hong Kong ranks seventh on the UN Human Development Index and has the seventh-longest life expectancy in the world. -

Kowloon (By Alphabetical Order of Name of Doctor)
Kowloon (By alphabetical order of name of doctor) Disclaimer: The information provided by the Department of Health, the Government of the Hong Kong Special Administrative Region ("the Government") on this webpage is for general reference only. The information contained therein reflects the updated information of the relevant participating doctors as at 16 May 2014 only. Whilst the Government endeavours to ensure the accuracy of the information on this page, the list also contains information provided by other parties which may be changed, deleted or edited at any time by the Government at its absolute discretion if updated information is available. Service Provider Practice Name and Address District 1. AU, KA KUI Dr Au Ka Kui KWUN GARY Shop 8-9, G/F, Hong Ning Court, 55 Hong Ning Road, TONG KWUN TONG, KOWLOON 2. AU, TAI KWAN University Health Service, The Hong Kong Polytechnic KOWLOON EVA University CITY (For PolyU Staff/ Staff Dependent Only) University Health Service, The Hong Kong Polytechnic University, HUNG HOM, KOWLOON 3. AU YEUNG, KAR Dr Au Yeung Kar Wai KOWLOON WAI ALEXANDER Shop 3B, G/F, Chung Man House, Oi Man Estate, HO CITY MAN TIN, KOWLOON 4. BIEN, TSE FANG Medical Clinic of Dr Bien Tse Fang Barry YAU TSIM BARRY Room 1615, 16/F, Argyle Centre Phase One, 688 Nathan MONG Road, MONGKOK, KOWLOON 5. CHAIN, CHI WOO Dr David Chain Chi Woo SHAM SHUI DAVID Room 219, Podium Floor, Nam Lok House, Nam Shan PO Estate, SHAM SHUI PO, KOWLOON 6. CHAK, NGAI Health & Treasure International Company Limited WONG TAI CHUEN (For Designated Clients only) Room 08, 17/F, Yip SIN Fung Industrial Building, 7 Sheung Hei Street, SAN PO KONG, KOWLOON 7. -
Information for Centres Providing Services Under the EHAPP.Xlsx
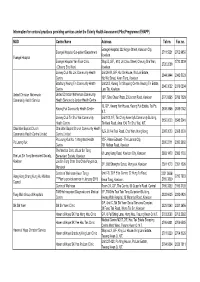
Information for centres/ practices providing services under the Elderly Health Assessment Pilot Programme (EHAPP) NGO Centre Name Address Tel no. Fax no. Evangel Hospital, 222 Argyle Street, Kowloon City, Evangel Hospital Out-patient Department 2711 5221 2762 9856 Kowloon Evangel Hospital Evangel Hospital Yan Fook Clinic Shop B, G/F., 418, Un Chau Street, Cheung Sha Wan, 2720 3309 2720 2038 (Cheung Sha Wan) Kowloon Jockey Club Wo Lok Community Health Unit 26-33, G/F, Kui On House, Wo Lok Estate, 2344 3444 2342 5023 Centre Hip Wo Street, Kwun Tong, Kowloon Bradbury Kwong Tin Community Health Unit 203, Kwong Tin Shopping Centre, Kwong Tin Estate, 2340 3022 2379 6234 Centre Lam Tin, Kowloon United Christian Nethersole United Christian Nethersole Community 13/F, Sino Cheer Plaza, 23 Jordan Road, Kowloon 2770 8365 2783 7528 Community Health Service Health Service c/o Jordan Health Centre 19, G/F, Kwong Yan House, Kwong Fuk Estate, Tai Po, Kwong Fuk Community Health Centre 2638 3846 2638 0142 N.T. Jockey Club Tin Shui Wai Community Unit 103, 1/F, Tin Ching Amenity& Community Building, 3156 9000 3543 5041 Health Centre Tin Kwai Road, Area 104, Tin Shui Wai, N.T. Chai Wan Baptist Church Chai Wan Baptist Church Community Health 1LG, 30 Fei Tsui Road, Chai Wan, Hong Kong 2965 3000 2965 3099 Community Health Centre Limited Centre Limited Po Leung Kuk No. 1 Integrated Health 17/F, Prince Edward - The Lamma City, Po Leung Kuk 2390 2711 2390 2962 Centre 761 Nathan Road, Kowloon The Medical Clinic of Lok Sin Tong 61 Lung Kong Road, Kowloon City, Kowloon 2383 1470 2383 1709 The Lok Sin Tong Benevolent Society, Benevolent Society, Kowloon Kowloon Lok Sin Tong Chan Cho Chak Polyclinics, 3/F, 688 Shanghai Street, Mongkok, Kowloon 2391 1073 2391 1095 Mongkok Centre of Wellness (Kwun Tong) Unit 7-8, 20/F Elite Centre, 22 Hung To Road, 2251 3636/ Hong Kong Sheng Kung Hui Welfare 2750 7903 ***Plan to provide service in January 2015 2169 3399 Council Kwun Tong, Kowloon.