Annual Performance Plan for 2012-13
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Restorica 22 1987.Pdf
South Africa's architectural heritage is constantly respect for the preservation of our traditional skills. threatened by sad neglect and - often - demolition. By combining our inherent expertise with modern There is, therefore, a continuing need for the project management techniques, the name of Gordon dedicated restoration and refurbishing of our beautiful Verhoef & Krause has become synonymous with the historical buildings. superior and efficient craftsmanship vital for the For 25 years, our commitment has been to fill that preservation of our buildings. need. Today, the company is striving to maintain this Throughout the country, Gordon Verhoef &Krause leading position as a major developer of restored has established teams of ~--don~l...-.-&.. properties and as a main con- experienced artisans, all \:1\..11 1 I 1\.1\:1 ' 7.. tractor in the recycling of buildings, craftsmen in their individual raUSC! .. endeavouring to improve the overan fields. They all have a quality of life in our environment. 25 Johannesburg 6146511 • Cape Town 45 5575 • Port Elizabeth 52 4094 • Durban 30 14317 • Pretoria 26 0555 • Windhoek 2 5641 London 735 8636 • Manchester 789 7105 Editorial Stigting Simon van der Stel Foundation (Ingelyfde Vereniging sander winsoogmerk Cape St. Francis Lighthouse Incorporated Association not for gain.) H. L. Huisman Opgerig/Established 8 Aprill959. Reg. No. 60/00005/08 The architectural background to the restoration of the Magtigingsnommer/Fundraising number: Schreiner House, Cradock F02 200215 000 8 Prof. ]. C. Radford Posbus/P.0. Box 17 43, Pretoria 000 l Briewe Nasionale Raad/National Council Nasionale Voorsitter!National Chairman Prince Albert se gewelhuise het wonderlik behoue gebly. Prof. -

13 Mpumalanga Province
Section B: DistrictProfile MpumalangaHealth Profiles Province 13 Mpumalanga Province Gert Sibande District Municipality (DC30) Overview of the district The Gert Sibande District Municipalitya is a Category C municipality located in the Mpumalanga Province. It is bordered by the Ehlanzeni and Nkangala District Municipalities to the north, KwaZulu-Natal and the Free State to the south, Swaziland to the east, and Gauteng to the west. The district is the largest of the three districts in the province, making up almost half of its geographical area. It is comprised of seven local municipalities: Govan Mbeki, Chief Albert Luthuli, Msukaligwa, Dipaleseng, Mkhondo, Lekwa and Pixley Ka Seme. Highways that pass through Gert Sibande District Municipality include the N11, which goes through to the N2 in KwaZulu-Natal, the N17 from Gauteng passing through to Swaziland, and the N3 from Gauteng to KwaZulu-Natal. Area: 31 841km² Population (2016)b: 1 158 573 Population density (2016): 36.4 persons per km2 Estimated medical scheme coverage: 13.5% Cities/Towns: Amersfoort, Amsterdam, Balfour, Bethal, Breyten, Carolina, Charl Cilliers, Chrissiesmeer, Davel, Ekulindeni, Embalenhle, Empuluzi, Ermelo, Evander, Greylingstad, Grootvlei, Kinross, Leandra, Lothair, Morgenzon, Perdekop, Secunda, Standerton, Trichardt, Volksrust, Wakkerstroom, eManzana, eMkhondo (Piet Retief). Main Economic Sectors: Manufacturing (57.4%), agriculture (41.4%), trade (25.8%), transport (24.5%), finance (21.2%), mining (14.1%), community services (12.3%), construction (2.1%). Population distribution, local municipality boundaries and health facility locations Source: Mid-Year Population Estimates 2016, Stats SA. a The Local Government Handbook South Africa 2017. A complete guide to municipalities in South Africa. Seventh edition. Accessible at: www. -

Greylingstad Mpumalanga Done by Do
Archaeological investigations, done at Bakkiesfontein 568 IR, (Dipaliseng Local Municipality) Greylingstad Mpumalanga Done by Domonique-Marie Verkerk BHSC (Heritage and Cultural Tourism), 2011, UP BA Archaeology, 2012, UP Tel: 012 3333931 E-mail: [email protected] Department of Anthropology and Archaeology, University of Pretoria 5 October 2015 Summary Concentration camps were a tactic created by the British to end the South African War (1899- 1902). Many innocent Boer and African families were sent to these camps where they died of diseases, such as, poor conditions and lack of shelters. Boer families were sent to concentration camps in Heidelberg. Africans, on the other hand, were sent to the concentration camp in Greylingstad. A possible location for the African concentration camp in Greylingstad is Bakkiesfontein 568 IR. Unfortunately, there is nothing to show where this camp is as a fire destroyed many of the records. Bakkiesfontein 568 IR was chosen as a possible location for the African concentration camp in Greylingstad because of the old house, stream, stone walls, railway, SR fort and the African cemetery. Bakkiesfontein was surveyed by foot. The aim was to find the location of the concentration camp. Areas where pedestrian surveys were conducted included the house, barn, possible midden, graves, stone walls and stone circle. The pedestrian survey showed that Iron Age communities also lived on the farm. Three test-pits were also conducted. Areas where the test-pits were conducted included the midden, between stone walls and on a slope near a stone wall. The test-pits were not that successful. The artefacts found during the test- pits and surveys include; metal, ceramic pieces and pottery, glass pieces and even plastic. -
Table of Contents
GERT SIBANDE DISTRICT MUNICIPALITY FINAL IDP 2011/12 TO 2013/14 A DISTRICT MUNICIPALITY STRIVING TO EXCEL IN GOOD GOVERNANCE AND QUALITY INFRASTRUCTURE Gert Sibande District Municipality i Foreword by the Executive Mayor It gives me great pleasure to present the Draft Integrated Development Plan for the 2011/12 to 2013/14 Financial Years, in the last year of this Current Term of Office. In reviewing our 2010/11 IDP and subsequently drafting our IDP and Budget respectively for 2011/12 to 2013/14 and beyond, we have consulted quite extensively with our communities in all our constituent Local Municipalities through their varying groupings using our IDP Representative Forum and other IGR structures institutionalised within our Municipality. Culminating from the state of the Nation and state of the Province Addresses respectively, and aforementioned consultation and engagements with varying stakeholders the following Key Development objectives were identified as pertinent in bringing about improved quality of life for our entire populace:- Facilitate creation of more jobs and descent work; Form strategic partnerships in fighting hunger and poverty; Advocate for access to quality education for all our citizens; Ensure proper health care for all our communities; Ensure sustainable development of all rural communities within our jurisdictional area; Harness the building of safer and secure communities To date resounding success has been realised in number of areas, where many of our people are living decent lives as a result of the services provided by the District in collaboration with its social partners. Whilst much has been achieved, there is still much that needs to be done to reverse and ultimately eradicate undesired consequences of underdevelopment, inequality, unemployment, HIV/AIDS and poverty. -
Accreditated Shooting Ranges
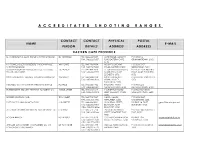
A C C R E D I T A T E D S H O O T I N G R A N G E S CONTACT CONTACT PHYSICAL POSTAL NAME E-MAIL PERSON DETAILS ADDRESS ADDRESS EASTERN CAPE PROVINCE D J SURRIDGE T/A ALOE RIDGE SHOOTING RANGE DJ SURRIDGE TEL: 046 622 9687 ALOE RIDGE MANLEY'S P O BOX 12, FAX: 046 622 9687 FLAT, EASTERN CAPE, GRAHAMSTOWN, 6140 6140 K V PEINKE (SOLE PROPRIETOR) T/A BONNYVALE WK PEINKE TEL: 043 736 9334 MOUNT COKE KWT P O BOX 5157, SHOOTING RANGE FAX: 043 736 9688 ROAD, EASTERN CAPE GREENFIELDS, 5201 TOMMY BOSCH AND ASSOCIATES CC T/A LOCK, T C BOSCH TEL: 041 484 7818 51 GRAHAMSTAD ROAD, P O BOX 2564, NOORD STOCK AND BARREL FAX: 041 484 7719 NORTH END, PORT EINDE, PORT ELIZABETH, ELIZABETH, 6056 6056 SWALLOW KRANTZ FIREARM TRAINING CENTRE CC WH SCOTT TEL: 045 848 0104 SWALLOW KRANTZ P O BOX 80, TARKASTAD, FAX: 045 848 0103 SPRING VALLEY, 5370 TARKASTAD, 5370 MECHLEC CC T/A OUTSPAN SHOOTING RANGE PL BAILIE TEL: 046 636 1442 BALCRAIG FARM, P O BOX 223, FAX: 046 636 1442 GRAHAMSTOWN, 6140 GRAHAMSTOWN, 6140 BUTTERWORTH SECURITY TRAINING ACADEMY CC WB DE JAGER TEL: 043 642 1614 146 BUFFALO ROAD, P O BOX 867, KING FAX: 043 642 3313 KING WILLIAM'S TOWN, WILLIAM'S TOWN, 5600 5600 BORDER HUNTING CLUB TE SCHMIDT TEL: 043 703 7847 NAVEL VALLEY, P O BOX 3047, FAX: 043 703 7905 NEWLANDS, 5206 CAMBRIDGE, 5206 EAST CAPE PLAINS GAME SAFARIS J G GREEFF TEL: 046 684 0801 20 DURBAN STREET, PO BOX 16, FORT [email protected] FAX: 046 684 0801 BEAUFORT, FORT BEAUFORT, 5720 CELL: 082 925 4526 BEAUFORT, 5720 ALL ARMS FIREARM ASSESSMENT AND TRAINING CC F MARAIS TEL: 082 571 5714 -
Amazon Missions
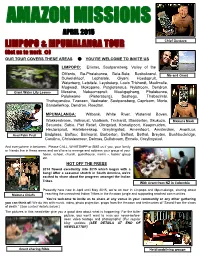
AMAZON MISSIONS APRIL 2015 LIMPOPO & MPUMALANGA TOUR Chief Gustavo (Get us to work ) OUR TOUR COVERS THESE AREAS YOU’RE WELCOME TO INVITE US LIMPOPO: Ellisras, Soutpansberg, Valley of the Olifants, Ba-Phalaborwa, Bela-Bela, Bosbokrand, Me and Grant Duiwelskloof, Lephalale, Giyani, Hoedspruit, Waterberg, Letsitele, Leydsdorp, Louis Trichardt, Modimolle, Mogwadi, Mokopane, Potgietersrus, Nylstroom, Dendron, Giant Water Lily Leaves Messina, Naboomspruit, Mookgophong, Phalaborwa, Polokwane (Pietersburg), Seshego, Thabazimbi, Thohoyandou, Tzaneen, Vaalwater, Soutpansberg, Capricorn, Moria, Bandelierkop, Dendron, Roedtan. MPUMALANGA: Witbank, White River, Waterval Boven, Wakkerstroom, Volksrust, Vaalbank, Trichardt, Standerton, Skukuza, Makuna Mask Secunda, Sabie, Piet Retief, Ohrigstad, Komatipoort, Kaapmuiden, Hectorspruit, Hartebeeskop, Greylingstad, Amersfoort, Amsterdam, Avontuur, Asai Palm Fruit Badplaas, Balfour, Balmoral, Barberton, Belfast, Bethal, Breyten, Bushbuckridge, Carolina, Chrissiesmeer, Delmas, Dullstroom, Ermelo, Greylingstad. And everywhere in between. Please CALL, WHATSAPP or SMS us if you, your family or friends live in these areas and we’d love to arrange and address your group at your home, school, church, guesthouse, men’s -, ladies’ group etc. HOT OFF THE PRESS 2014 flowed excellently into 2015 which began with a bang! After a seasonal stretch in South America, we’re excited to share about the progress amongst the Indian Tribes. With Grant from NZ in Colombia Presently here now in April until May 2015, we’re on tour in Limpopo and Mpumalanga, sharing about reaching the unreached Indian Tribes in the Amazon jungle and supporting reached communities. Makuna Chiefs You’re welcome to invite us to share at any venue in your community or any other gathering you can think of! We do this with music, video, photo projection, props from the Amazon and testimonies of “Saved from the claws of death.” (See contact details below.) The pictures in this newsletter give you a good idea about what is happening. -

Dlm Final Idp 2017/22
INTEGRATED DEVELOPMENT PLAN 2017 – 2022 FINANCIAL YEARS DLM FINAL IDP 2017/22 FOREWORD BY THE EXECUTIVE MAYOR “IT IS NOT GIVEN TO EVERY GENERATION THAT IT SHOULD BE PRESENT DURING AND PARTICIPATE IN THE ACT OF CREATION” PRESIDENT THABO MBEKI, APRIL 1997” This draft IDP is indeed an act of creation. The beginning of something great and good for all our Communities. It will illustrate our commitment as Government to the needs of our people. It will set clear goals and targets for all of us, i.e. the Municipality and the Community it serves. More even it will demonstrate our will to put infrastructure and services in place that will ensure a better life for all our people. In this, the decade of Freedom, we’ll strive to play our role as Developmental Local Government to the best of our ability. We will create an environment for economic growth and job creation, as tools for the eradication of Poverty and Unemployment. The IDP will also bring with it some important challenges, which includes funding for projects and programmes. We believe as a team, Government and its people, we will turn this around by going all out in promoting our IDP and its objectives. It’s with great pleasure that we present to you our contribution to “a people’s contract, which will create work and fight poverty”. The road ahead may seem long and daunting but we are confident that with Dipaleseng Municipality at the helm, we will succeed in ensuring that people’s issues are effectively dealt with to pave the way for efficient delivery of services _________________ CLR M.L.MAKHUBU EXECUTIVE MAYOR 1 OVERVIEW BY THE ACCOUNTING OFFICER The Municipal Systems Act 32 of 2000 requires municipalities to adopt an Integrated Development Plan. -

Greylingstad
Greylingstad There are only 19 ads for the city Greylingstad, so we don't split them by categories. Tuesday, 20 November 2018. Get fresh clean tight pussy. A nice clean shaved pussy i welcome all you horny guys how about me on top of your dick catch me on⦠Mpumalanga ⺠Greylingstad ⺠Personals ⺠Women looking for Men. Come get the best pussy. Clean warm tight pussy to meet all your sexual desires i offer the best sex session with no rush⦠Mpumalanga ⺠Greylingstad ⺠Personals ⺠Women looking for Men. Greylingstad (Afrikaans for Greyling City) is a small farming town west of Standerton in Mpumalanga, South Africa. During the Boer War the Scottish Rifles built a number of small forts overlooking the town and the farms beyond the hills. The Scottish Rifles laid out the initials "SR" on the hill overlooking the town, and it was always clearly visible from the main street of Greylingstad. The town was founded in 1909 by the Dutch Reformed Church and named after PJ Greyling. Today Greylingstad is almost a ghost town, with many vacant buildings and houses, in a varying state of disrepair. The farming community, maize and dairy, however is still big and growing and constantly doing business. The department of Arts and Culture published the name change of Greylingstad to Nthorwane in their government notice No. 238 of Gazette No. 36299 on the 28th of March 2013. Dutch Reformed Church in Greylingstad. Entering the residential area. The Mills. You will find below the horoscope of Anni-Frid Lyngstad with her interactive chart, an excerpt of her astrological portrait and her planetary dominants. -

20 Year Review of Local Government
Local Government Brief, November 2014 Local Government Briefs are monthly electronic updates for municipalities on critical areas of law, policy, facts and data affecting the sector. Author: Rachel Manxeba - Data Analyst: Municipal Barometer Edited by: Nomusa Ngwenya – Director Local Governance & Development Data (LGDD) Introduction The Municipal Barometer is a web-based portal that is aimed at collecting and packaging local level data including ward level data to municipalities. It is envisaged that municipalities will use the data for planning, oversight and benchmarking. SALGA analyses the data periodically and disseminates it in the form of briefs and other publications. This third edition of the publication focuses on Gert- Sibande District Municipality. Summary of the District • District Municipality in Mpumalanga Province • 7 local municipalities: Chief Alb ert Luthuli, Dip a leseng Govan Mbeki Lekwa Mkhond o Msuka ligwa Dr. Pixley Ka Seme • Towns Chief Albert Luthuli: Ca rolina , Bad p la a s, Eerstehoek, Loc hiel Dipaleseng: Balfour, Da sville, Greylingsta d , Grootvlei, Va l, Willemsda l. Govan Mbeki: Sec und a , Betha l, Bethel East, Bethelra nd , Cha rl Cilliers, Eva nd er, Kinross, Lea nd ra , Leslie, Rood eb a nk, Springbokdraai, Tric ha rd t, Winkelha a k Lekwa: Standerton, Bettiesda m, Elmtree, Holmd ene, Ma izefield , Meyerville, Morgenzon, Pla tra nd , Rob erts Drift, Sta nfield Hill Mkhondo: Piet Retief (Mkhondo), Amsterdam, Anysspruit, Berbic e, Bergen, Braunchweig, Commond a le, Dirkiesdorp , Iswep e, Moolma n, Panb ult, Wittenb erg Msukaligwa: Ermelo, Bankkop , Breyten, Ca md en, Chrissiesmeer, Da vel, Esta nc ia , Holb a n, Kafferspruit, Lotha ir, Sheep moor, Wa rb urton Dr. -

Greylingstad Mpumalanga Done by Do
Archaeological investigations, done at Bakkiesfontein 568 IR, (Dipaliseng Local Municipality) Greylingstad Mpumalanga Done by Domonique-Marie Verkerk BHSC (Heritage and Cultural Tourism), 2011, UP BA Archaeology, 2012, UP Tel: 012 3333931 E-mail: [email protected] Department of Anthropology and Archaeology, University of Pretoria 16 August 2016 Summary It can be argued that the African concentration camp was situated on the farm Bakkiesfontein 568 IR, Greylingstad, Mpumalanga, South Africa, due to the artefacts and graves found during the previous visits to the farm. Benneyworth also states that the African concentration camp was situated on Bakkiesfontein 568 IR, as he discovered another burial site belonging to the camp. These graves were very similar to the previous ones found during the earlier archaeological investigation, yet there are also many differences between them. This discovery between the graves indicate that at a certain time in history the British decided to move the old camp to a new location on the same farm. One reason for this move could have been due to the fact that the camp was overcrowded with internees. The findings also revealed that the stone walls were built by an Iron Age community. However, during the South African War, these stone walls could also have been used by the British as a fort and African internees as make-shift shelters. By, erecting a monument at Bakkiesfontein 568 IR, more people will want to protect their heritage. To protect the graves from damage, the owners can also fence the graves with strong barbed-wires. i Table of contents Summary ..................................................................................................................................... i List of Figures ......................................................................................................................... -

Mp Dipaleseng Magisterial District Balfour.Pdf
# # !C # # ### !C^# !.!C# # # !C # # # # # # # # # # # ^!C # # # # # # # ^ # # ^ # # !C # ## # # # # # # # # # # # # # # # # !C# # # !C # # # # # # # # #!C # # # # # #!C# # # # # # !C ^ # # # # # # # ^ # # #!C # # # # # # # !C # #^ # # # # # # ## # #!C # # # # # ## # !C # # # # # # # !C# ## # # #!C # !C # # # # # # # # # ^ # # # # # # # # # # # !C# # # # # # # # # # # # # # # # # # #!C # # # # # # # # # ## # # # # # !C # # # ## # # # # # !C # # # ## # # # # # !C # # # # # # # # # # !C# # # #^ # # # # # # !C# # # # # # # # # # # # # # # # # # # # # ## # # # # #!C ## # ##^ # !C #!C# # # # # # # # # # # # # # # # # ## # # # # #!C ^ ## # # # # # # # # # # # # # # # ## # # # # # # # ## # # # # !C # #!C # # #!C # # # # # # # !C# # # # # # # !C## # # # # # # # # # # # # # # # ## ## # # # # # # # # # # # # # # # # # # # # # # # # # # # # #!C # ## # # # # # # # ## # # ^!C # # # # # # # # # # # # # # ^ # # # ## # # # # # # # # # # ## #!C # # # # # # #!C # !C # # # # !C # # # # !C# # # # # # # # # # # # ## # !C# # ## # # # # # ## # # # # # # # # # # # # # # # # !C# # # # # # ### !C # # # !C !C# # # ## # # # ## !C !C # !. # # # # # # # # # # # # # # ## # #!C # # # # ## # # # # # # # # # # # # # #^ # # # # # ## ## # # # # # !C ## # # ## # ^ # # # # # # !C## # # # # # # # # # ## # ## # ## ## # !C## !C## # # # !C # # # # ## # !C # # # ^ # # !C ### # # # !C# # #!C # !C # # ^ ## #!C ### # # !C # # # # # # # # ## # ## ## # # # # # !C # # # #!C # ## # # # # ## # # # # # # # !C # # ^ # ## # # # # !C # # # # # # # !. # # !C# ### # # # # !C # # # # # # # # -

(013) 7955241 6066895 Mpumalanga Aerorand Mi
PRACTICE PROVINCE PHYSICAL SUBURB PHYSICAL TOWN PHYSICAL ADDRESS PHARMACY NAME CONTACT NUMBER NUMBER MPUMALANGA ACORNHOEK ACORNHOEK CORNER MAIN ROAD AND OU ACORNHOEK PHARMACY (013) 7955241 6066895 ORPEN WEG MPUMALANGA AERORAND MIDDELBURG CORNER KEISKAMMEA AND CLICKS PHARMACY MIDWATER (013) 2442604 240680 ORANGE STREETS CENTRE MPUMALANGA BALFOUR BALFOUR 12 JOHNNY MOKOENA DRIVE GREYLINGSTAD PHARMACY (017) 7731364 284297 MPUMALANGA BALFOUR BALFOUR 18 JOHN MUKWENA STREET HOEVELD APTEEK (017) 7730019 6012221 MPUMALANGA BARBERTON BARBERTON CORNER GENERAL AND HILLARY CLICKS PHARMACY BARBERTON (013) 7123402 600830 STREETS MPUMALANGA BARBERTON BARBERTON 86 CROWN STREET M.G. EKSTEEN PHARMACY (013) 7122181 6012272 MPUMALANGA BELFAST BELFAST 23 FITZGERALD STREET VAN BILJON PHARMACY (013) 2531241 6012329 MPUMALANGA BETHAL BETHAL 44A CHRIS HANI STREET KARK APTEEK (017) 6475851 6012647 MPUMALANGA BUSHBUCKRIDGE BUSHBUCKRIDGE MAIN ROAD BOSBOKRAND PHARMACY (013) 7990143 6045693 MPUMALANGA CAROLINA CAROLINA 28 VOORTREKKER STREET DU PREEZ PHARMACY (017) 8431115 6029779 MPUMALANGA CLUBVILLE MIDDELBURG 26 DE VILLIERS STREET CLUBVILLE PHARMACY (013) 2825453 6064159 MPUMALANGA DELMAS DELMAS 32 SAREL CILLIERS STREET C.J. WILLIAMS PHARMACY (013) 6652281 6013384 MPUMALANGA DELMAS DELMAS CORNER SAMUEL ROAD AND CLICKS PHARMACY DELMAS (013) 6652413 367443 VAN DER WALT STREET MPUMALANGA DELMAS DELMAS 31B SAREL CILLIERS STREET LINK PHARMACY - DELMAS (013) 6652091 6013368 GEMS REO NETWORK PHARMACY – MPUMALANGA Page 1 of 9 PRACTICE PROVINCE PHYSICAL SUBURB PHYSICAL TOWN