Rare Variants in IFFO1, DTNB and NLRC3 Associate with Alzheimer's
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supp Material.Pdf
Simon et al. Supplementary information: Table of contents p.1 Supplementary material and methods p.2-4 • PoIy(I)-poly(C) Treatment • Flow Cytometry and Immunohistochemistry • Western Blotting • Quantitative RT-PCR • Fluorescence In Situ Hybridization • RNA-Seq • Exome capture • Sequencing Supplementary Figures and Tables Suppl. items Description pages Figure 1 Inactivation of Ezh2 affects normal thymocyte development 5 Figure 2 Ezh2 mouse leukemias express cell surface T cell receptor 6 Figure 3 Expression of EZH2 and Hox genes in T-ALL 7 Figure 4 Additional mutation et deletion of chromatin modifiers in T-ALL 8 Figure 5 PRC2 expression and activity in human lymphoproliferative disease 9 Figure 6 PRC2 regulatory network (String analysis) 10 Table 1 Primers and probes for detection of PRC2 genes 11 Table 2 Patient and T-ALL characteristics 12 Table 3 Statistics of RNA and DNA sequencing 13 Table 4 Mutations found in human T-ALLs (see Fig. 3D and Suppl. Fig. 4) 14 Table 5 SNP populations in analyzed human T-ALL samples 15 Table 6 List of altered genes in T-ALL for DAVID analysis 20 Table 7 List of David functional clusters 31 Table 8 List of acquired SNP tested in normal non leukemic DNA 32 1 Simon et al. Supplementary Material and Methods PoIy(I)-poly(C) Treatment. pIpC (GE Healthcare Lifesciences) was dissolved in endotoxin-free D-PBS (Gibco) at a concentration of 2 mg/ml. Mice received four consecutive injections of 150 μg pIpC every other day. The day of the last pIpC injection was designated as day 0 of experiment. -

17 - 19 October 2019
THE 12TH INTERNATIONAL SYMPOSIUM ON HEALTH INFORMATICS AND BIOINFORMATICS T G T A A A T G A G A A G T T G G G T A A A A A A A A T T T A A A A A A G G A A A A A A A G G G G G G G G A A A G G G G G G T T G G G G G G G T T T T G G T T G G G T T T G G T A A T T G G T T T A A A A A A A A T T T A A A A A A T T A A A A A A A T A T T T T T T A A A T T T T G T A G A A T T T A A 17 - 19 OCTOBER 2019 HIBIT 2019 ABSTRACT BOOK THE 12TH INTERNATIONAL SYMPOSIUM ON HEALTH INFORMATICS AND BIOINFORMATICS TABLE OF CONTENTS 1 8 WELCOME MESSAGE KEYNOTE LECTURERS 2 19 ORGANIZING COMMITEE INVITED SPEAKERS 3 29 SCIENTIFIC COMMITEE SELECTED ABSTRACTS FOR ORAL PRESENTATIONS 6 61 PROGRAM POSTER PRESENTATIONS Welcome Message The International Symposium on Health Informatics and Bioinformatics, (HIBIT), now in its twelfth year HIBIT 2019, aims to bring together academics, researchers and practitioners who work in these popular and fulfilling areas and to create the much- needed synergy among medical, biological and information technology sectors. HIBIT is one of the few conferences emphasizing such synergy. -

Supp Table 6.Pdf
Supplementary Table 6. Processes associated to the 2037 SCL candidate target genes ID Symbol Entrez Gene Name Process NM_178114 AMIGO2 adhesion molecule with Ig-like domain 2 adhesion NM_033474 ARVCF armadillo repeat gene deletes in velocardiofacial syndrome adhesion NM_027060 BTBD9 BTB (POZ) domain containing 9 adhesion NM_001039149 CD226 CD226 molecule adhesion NM_010581 CD47 CD47 molecule adhesion NM_023370 CDH23 cadherin-like 23 adhesion NM_207298 CERCAM cerebral endothelial cell adhesion molecule adhesion NM_021719 CLDN15 claudin 15 adhesion NM_009902 CLDN3 claudin 3 adhesion NM_008779 CNTN3 contactin 3 (plasmacytoma associated) adhesion NM_015734 COL5A1 collagen, type V, alpha 1 adhesion NM_007803 CTTN cortactin adhesion NM_009142 CX3CL1 chemokine (C-X3-C motif) ligand 1 adhesion NM_031174 DSCAM Down syndrome cell adhesion molecule adhesion NM_145158 EMILIN2 elastin microfibril interfacer 2 adhesion NM_001081286 FAT1 FAT tumor suppressor homolog 1 (Drosophila) adhesion NM_001080814 FAT3 FAT tumor suppressor homolog 3 (Drosophila) adhesion NM_153795 FERMT3 fermitin family homolog 3 (Drosophila) adhesion NM_010494 ICAM2 intercellular adhesion molecule 2 adhesion NM_023892 ICAM4 (includes EG:3386) intercellular adhesion molecule 4 (Landsteiner-Wiener blood group)adhesion NM_001001979 MEGF10 multiple EGF-like-domains 10 adhesion NM_172522 MEGF11 multiple EGF-like-domains 11 adhesion NM_010739 MUC13 mucin 13, cell surface associated adhesion NM_013610 NINJ1 ninjurin 1 adhesion NM_016718 NINJ2 ninjurin 2 adhesion NM_172932 NLGN3 neuroligin -
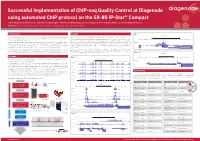
Successful Implementation of Chip-Seq Quality Control At
Successful implementation of ChIP-seq Quality Control at Diagenode using automated ChIP protocol on the SX-8G IP-Star® Compact Jan Hendrickx, Géraldine Goens, Catherine D’andrea, Ignacio Mazon, Geoffrey Berguet, Sharon Squazzo, Céline Sabatel, Miklos Laczik, Dominique Poncelet. Diagenode sa, CHU, Tour GIGA B34, 3ème étage 1 Avenue de l’Hôpital, 4000 Liège, Sart-Tilman, Belgium Introduction Results Figure 3 ZNF12 Chromatin immunoprecipitation (ChIP) is the most widely used method to study protein-DNA We have validated 19 of the Diagenode ChIP-grade antibodies using ChIP-seq (see table 1). interactions. A successful ChIP, however, is largely depending on the use of well characterised, Scale 100 kb Figure 1 shows the profiles obtained with antibodies against (1) H3K4me3, H3K9ac and H3K9/14ac, chr7: 6620000 6630000 6640000 6650000 6660000 6670000 6680000 6690000 6700000 6710000 6720000 6730000 6740000 6750000 6760000 6770000 6780000 6790000 6800000 highly specific ChIP-grade antibodies. histone modifications that are present at active promoters, (2) H3K4me2 which is surrounding 35 - We have established a robust QC procedure to be able to provide researchers with the highest quality promoters of active genes, (3) H3K79me3 present at promoters of active genes and extending into H3K9me3 ChIP-grade antibodies. The recent development of high throughput sequencing (HTS) technologies the gene body, and (4) H3K36me3, present at the gene bodies of active genes. The screenshots below 1 _ has also opened new possibilities for epigenetic research. ChIP followed by HTS (ChIP-seq) enables show the peak distribution along the complete X-chromosome and in a 75 kb region surrounding the C7orf26 AK123300 ZNF12 PMS2CL RSPH10B C7orf26 ZNF12 RSPH10B the extension of the target directed analysis of ChIP results to a genome wide analysis. -

Chromatin Accessibility and the Regulatory Epigenome
REVIEWS EPIGENETICS Chromatin accessibility and the regulatory epigenome Sandy L. Klemm1,4, Zohar Shipony1,4 and William J. Greenleaf1,2,3* Abstract | Physical access to DNA is a highly dynamic property of chromatin that plays an essential role in establishing and maintaining cellular identity. The organization of accessible chromatin across the genome reflects a network of permissible physical interactions through which enhancers, promoters, insulators and chromatin-binding factors cooperatively regulate gene expression. This landscape of accessibility changes dynamically in response to both external stimuli and developmental cues, and emerging evidence suggests that homeostatic maintenance of accessibility is itself dynamically regulated through a competitive interplay between chromatin- binding factors and nucleosomes. In this Review , we examine how the accessible genome is measured and explore the role of transcription factors in initiating accessibility remodelling; our goal is to illustrate how chromatin accessibility defines regulatory elements within the genome and how these epigenetic features are dynamically established to control gene expression. Chromatin- binding factors Chromatin accessibility is the degree to which nuclear The accessible genome comprises ~2–3% of total Non- histone macromolecules macromolecules are able to physically contact chroma DNA sequence yet captures more than 90% of regions that bind either directly or tinized DNA and is determined by the occupancy and bound by TFs (the Encyclopedia of DNA elements indirectly to DNA. topological organization of nucleosomes as well as (ENCODE) project surveyed TFs for Tier 1 ENCODE chromatin- binding factors 13 Transcription factor other that occlude access to lines) . With the exception of a few TFs that are (TF). A non- histone protein that DNA. -

Ku70 Is Associated with the Frequency of Chromosome Translocation in Human Lymphocytes After Radiation and T-Cell Acute Lymphoblastic Leukemia
Ku70 is Associated with the Frequency of Chromosome Translocation in Human Lymphocytes After Radiation and T-Cell Acute Lymphoblastic Leukemia Zhenbo Cheng Central South University Third Xiangya Hospital https://orcid.org/0000-0001-6674-2697 Yupeng Wang Hunan Provincial People's Hospital Lihuang Guo Central South University Third Xiangya Hospital Jiancheng Li Central South University Third Xiangya Hospital Wei Zhang Central South University Third Xiangya Hospital Conghui Zhang Central South University Third Xiangya Hospital Yangxu Liu Central South University Third Xiangya Hospital Yue Huang Central South University Third Xiangya Hospital Keqian Xu ( [email protected] ) Central South University, Changsha Research Keywords: Ku70, chromosome translocation, human lymphocytes, radiation, T-cell acute lymphoblastic leukemia, radiation damage biomarker, therapy target Posted Date: September 3rd, 2021 DOI: https://doi.org/10.21203/rs.3.rs-858112/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/18 Abstract Background: Chromosome translocation is one of the most common chromosomal causes to T-cell acute lymphoblastic leukemia (T-ALL). Ku70 is one of the key factors of error-prone DNA repair that may end in translocation. So far, the direct correlation between Ku70 and translocation has not been assessed. Our study aimed to investigate the association of Ku70 and translocation in human lymphocytes after radiation and T-ALL. Methods: Peripheral blood lymphocytes (PBLs) from volunteers and human lymphocyte cell line AHH- 1were irradiated with X-rays to form chromosome translocations. The frequency of translocation was detected by uorescence in situ hybridization (FISH), meanwhile, the expression of Ku70 was also detected by reverse transcription-quantitative polymerase chain reaction (RT-qPCR) and western blot. -

Anticancer Effect of Natural Product Sulforaphane by Targeting MAPK Signal Through Mirna-1247-3P in Human Cervical Cancer Cells
Article Volume 11, Issue 1, 2021, 7943 - 7972 https://doi.org/10.33263/BRIAC111.79437972 Anticancer Effect of Natural Product Sulforaphane by Targeting MAPK Signal through miRNA-1247-3p in Human Cervical Cancer Cells Meng Luo 1 , Dian Fan 2 , Yinan Xiao 2 , Hao Zeng 2 , Dingyue Zhang 2 , Yunuo Zhao 2 , Xuelei Ma 1,* 1 Department of Biotherapy, State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, P.R. China; [email protected] (L.M.); 2 West China Medical School, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, P.R. China; [email protected] (F.D.); [email protected] (X.Y.N.); [email protected] (Z.H.); [email protected] (Z.D.Y.); [email protected] (Z.Y.N.); * Correspondence: [email protected]; Scopus Author ID 55523405000 Received: 11.06.2020; Revised: 3.07.2020; Accepted: 5.07.2020; Published: 9.07.2020 Abstract: The prognosis of cervical cancer remains poor. Sulforaphane, an active ingredient from cruciferous plants, has been identified as a potential anticancer agent in various cancers. However, there is little information about its effect on cervical cancer. Here, we conducted a present study to uncover the effect and the potential mechanisms of sulforaphane on cervical cancer. HeLa cells were treated with sulforaphane, and cell proliferation and apoptosis were assessed by Cell Counting Kit-8, Western blot, flow cytometry, and immunofluorescence. Then, next-generation sequencing (NGS) and bioinformatics tools were used to analyze mRNA-seq, miRNA-seq, and potential pathways. Finally, qRT-PCR, Cell Counting Kit-8, flow cytometry, small RNAs analysis, and Western blot were performed to evaluate the biological function of miR1247-3p and MAPK pathway in HeLa cell lines. -
A New Parsimonious Method for Classifying Cancer Tissue-Of-Origin Based on DNA Methylation 450K Data
A new parsimonious method for classifying Cancer Tissue-of-Origin Based on DNA Methylation 450K data Shen Jia1#, Yulin Zhang2#, Yiming Mao1, Jiawei Gao1, Yixuan Chen1, Yuxuan Jiang1, Haochen Luo3, Kebo Lv4*, Jionglong Su5* 1 Department of Mathematics, University of Liverpool, Liverpool, UK 2 College of Mathematics and Systems Science, Shandong University of Science and Technology, Qingdao, China 3 Department of Computer Science, University of Liverpool, UK 4School of Mathematical Sciences, Ocean University of China, Qingdao, China 5 School of AI and Advanced Computing, XJTLU Entrepreneur College(Taicang), Xi’an Jiaotong- Liverpool University, Suzhou, China # These authors contribute equally to the work *Corresponding author: Kebo Lv (e-mail: [email protected]), Jionglong Su (email: [email protected]) Abstract DNA methylation is a well-studied genetic modification that regulates gene transcription of Eukaryotes. Its alternations have been recognized as a significant component of cancer development. In this study, we use the DNA methylation 450k data from The Cancer Genome Atlas to evaluate the efficacy of DNA methylation data on cancer classification for 30 cancer types. We propose a new method for gene selection in high dimensional data(over 450 thousand). Variance filtering is first introduced for dimension reduction and Recursive feature elimination (RFE) is then used for feature selection. We address the problem of selecting a small subsets of genes from large number of methylated sites, and our parsimonious model is demonstrated to be efficient, achieving an accuracy over 91%, outperforming other studies which use DNA micro-arrays and RNA-seQ Data . The performance of 20 models, which are based on 4 estimators (Random Forest, Decision Tree, Extra Tree and Support Vector Machine) and 5 classifiers (k-Nearest Neighbours, Support Vector Machine, XGboost, Light GBM and Multi-Layer Perceptron), is compared and robustness of the RFE algorithm is examined. -

Oxidized Phospholipids Regulate Amino Acid Metabolism Through MTHFD2 to Facilitate Nucleotide Release in Endothelial Cells
ARTICLE DOI: 10.1038/s41467-018-04602-0 OPEN Oxidized phospholipids regulate amino acid metabolism through MTHFD2 to facilitate nucleotide release in endothelial cells Juliane Hitzel1,2, Eunjee Lee3,4, Yi Zhang 3,5,Sofia Iris Bibli2,6, Xiaogang Li7, Sven Zukunft 2,6, Beatrice Pflüger1,2, Jiong Hu2,6, Christoph Schürmann1,2, Andrea Estefania Vasconez1,2, James A. Oo1,2, Adelheid Kratzer8,9, Sandeep Kumar 10, Flávia Rezende1,2, Ivana Josipovic1,2, Dominique Thomas11, Hector Giral8,9, Yannick Schreiber12, Gerd Geisslinger11,12, Christian Fork1,2, Xia Yang13, Fragiska Sigala14, Casey E. Romanoski15, Jens Kroll7, Hanjoong Jo 10, Ulf Landmesser8,9,16, Aldons J. Lusis17, 1234567890():,; Dmitry Namgaladze18, Ingrid Fleming2,6, Matthias S. Leisegang1,2, Jun Zhu 3,4 & Ralf P. Brandes1,2 Oxidized phospholipids (oxPAPC) induce endothelial dysfunction and atherosclerosis. Here we show that oxPAPC induce a gene network regulating serine-glycine metabolism with the mitochondrial methylenetetrahydrofolate dehydrogenase/cyclohydrolase (MTHFD2) as a cau- sal regulator using integrative network modeling and Bayesian network analysis in human aortic endothelial cells. The cluster is activated in human plaque material and by atherogenic lipo- proteins isolated from plasma of patients with coronary artery disease (CAD). Single nucleotide polymorphisms (SNPs) within the MTHFD2-controlled cluster associate with CAD. The MTHFD2-controlled cluster redirects metabolism to glycine synthesis to replenish purine nucleotides. Since endothelial cells secrete purines in response to oxPAPC, the MTHFD2- controlled response maintains endothelial ATP. Accordingly, MTHFD2-dependent glycine synthesis is a prerequisite for angiogenesis. Thus, we propose that endothelial cells undergo MTHFD2-mediated reprogramming toward serine-glycine and mitochondrial one-carbon metabolism to compensate for the loss of ATP in response to oxPAPC during atherosclerosis. -
Statistical and Bioinformatic Analysis of Hemimethylation Patterns in Non-Small Cell Lung Cancer Shuying Sun1* , Austin Zane2, Carolyn Fulton3 and Jasmine Philipoom4
Sun et al. BMC Cancer (2021) 21:268 https://doi.org/10.1186/s12885-021-07990-7 RESEARCH ARTICLE Open Access Statistical and bioinformatic analysis of hemimethylation patterns in non-small cell lung cancer Shuying Sun1* , Austin Zane2, Carolyn Fulton3 and Jasmine Philipoom4 Abstract Background: DNA methylation is an epigenetic event involving the addition of a methyl-group to a cytosine- guanine base pair (i.e., CpG site). It is associated with different cancers. Our research focuses on studying non-small cell lung cancer hemimethylation, which refers to methylation occurring on only one of the two DNA strands. Many studies often assume that methylation occurs on both DNA strands at a CpG site. However, recent publications show the existence of hemimethylation and its significant impact. Therefore, it is important to identify cancer hemimethylation patterns. Methods: In this paper, we use the Wilcoxon signed rank test to identify hemimethylated CpG sites based on publicly available non-small cell lung cancer methylation sequencing data. We then identify two types of hemimethylated CpG clusters, regular and polarity clusters, and genes with large numbers of hemimethylated sites. Highly hemimethylated genes are then studied for their biological interactions using available bioinformatics tools. Results: In this paper, we have conducted the first-ever investigation of hemimethylation in lung cancer. Our results show that hemimethylation does exist in lung cells either as singletons or clusters. Most clusters contain only two or three CpG sites. Polarity clusters are much shorter than regular clusters and appear less frequently. The majority of clusters found in tumor samples have no overlap with clusters found in normal samples, and vice versa. -

Probe Set Name Symbol 1598 G at Growth Arres
Supplementary Table 2. List of stroma related genes (i.e. probe sets overexpressed in core relative to FNA biopsies of the same cancer) Probe set Name Symbol 1598_g_at growth arrest-specific 6 GAS6 200048_s_at jumping translocation breakpoint JTB 200054_at zinc finger protein 259 ZNF259 200055_at TAF10 RNA polymerase II, TATA box binding protein (TBP)-associatedTAF10 factor, 30kDa 200059_s_at ras homolog gene family, member A RHOA 200060_s_at RNA binding protein S1, serine-rich domain RNPS1 200070_at chromosome 2 open reading frame 24 C2orf24 200613_at adaptor-related protein complex 2, mu 1 subunit AP2M1 200663_at CD63 molecule CD63 200665_s_at secreted protein, acidic, cysteine-rich (osteonectin) SPARC 200671_s_at spectrin, beta, non-erythrocytic 1 SPTBN1 200696_s_at gelsolin (amyloidosis, Finnish type) GSN 200704_at lipopolysaccharide-induced TNF factor LITAF 200738_s_at phosphoglycerate kinase 1 PGK1 200760_s_at ADP-ribosylation-like factor 6 interacting protein 5 ARL6IP5 200762_at dihydropyrimidinase-like 2 DPYSL2 200770_s_at laminin, gamma 1 (formerly LAMB2) LAMC1 200771_at laminin, gamma 1 (formerly LAMB2) LAMC1 200772_x_at prothymosin, alpha PTMA 200778_s_at septin 2 2-Sep 200782_at annexin A5 ANXA5 200784_s_at low density lipoprotein-related protein 1 (alpha-2-macroglobulin receptor)LRP1 200785_s_at low density lipoprotein-related protein 1 (alpha-2-macroglobulin receptor)LRP1 200795_at SPARC-like 1 (hevin) SPARCL1 200799_at heat shock 70kDa protein 1A HSPA1A 200807_s_at heat shock 60kDa protein 1 (chaperonin) HSPD1 200811_at -

Microarray Screening Reveals a Non-Conventional SUMO-Binding Mode Linked to DNA Repair by Non-Homologous End-Joining
bioRxiv preprint doi: https://doi.org/10.1101/2021.01.20.427433; this version posted January 20, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Microarray screening reveals a non-conventional SUMO-binding mode linked to DNA repair by non-homologous end-joining Maria Jose Cabello-Lobato1, Matthew Jenner2,3, Christian M. Loch4, Stephen P. Jackson5, Qian Wu6, Matthew J. Cliff7, Christine K. Schmidt1* 1Manchester Cancer Research Centre (MCRC), Division of Cancer Sciences, School of Medical Sciences, Faculty of Biology, Medicine and Health, University of Manchester, 555 Wilmslow Road, Manchester M20 4GJ, UK 2Department of Chemistry, University of Warwick, Coventry, CV4 7AL, UK 3Warwick Integrative Synthetic Biology (WISB) Centre, University of Warwick, Coventry, CV4 7AL, UK 4AVM Biomed, Pottstown, PA 19464, USA 5Wellcome/Cancer Research UK Gurdon Institute and Department of Biochemistry, University of Cambridge, Cambridge CB2 1QN, UK 6Astbury Centre for Structural Molecular Biology, School of Molecular & Cellular Biology, Faculty of Biological Sciences, University of Leeds, Leeds LS2 9JT, UK 7Manchester Institute of Biotechnology (MIB) and School of Chemistry, University of Manchester, Manchester M1 7DN, UK *Correspondence: [email protected] SUMOylation is critical for a plethora of cellular signalling pathways including the repair of DNA double-strand breaks (DSBs). If misrepaired, DSBs can lead to cancer, neurodegeneration, immunodeficiency and premature ageing. Based on systematic proteome microarray screening combined with widely applicable carbene footprinting and high-resolution structural profiling, we define two non-conventional SUMO2- binding modules on XRCC4, a DNA repair protein important for DSB repair by non- homologous end-joining (NHEJ).