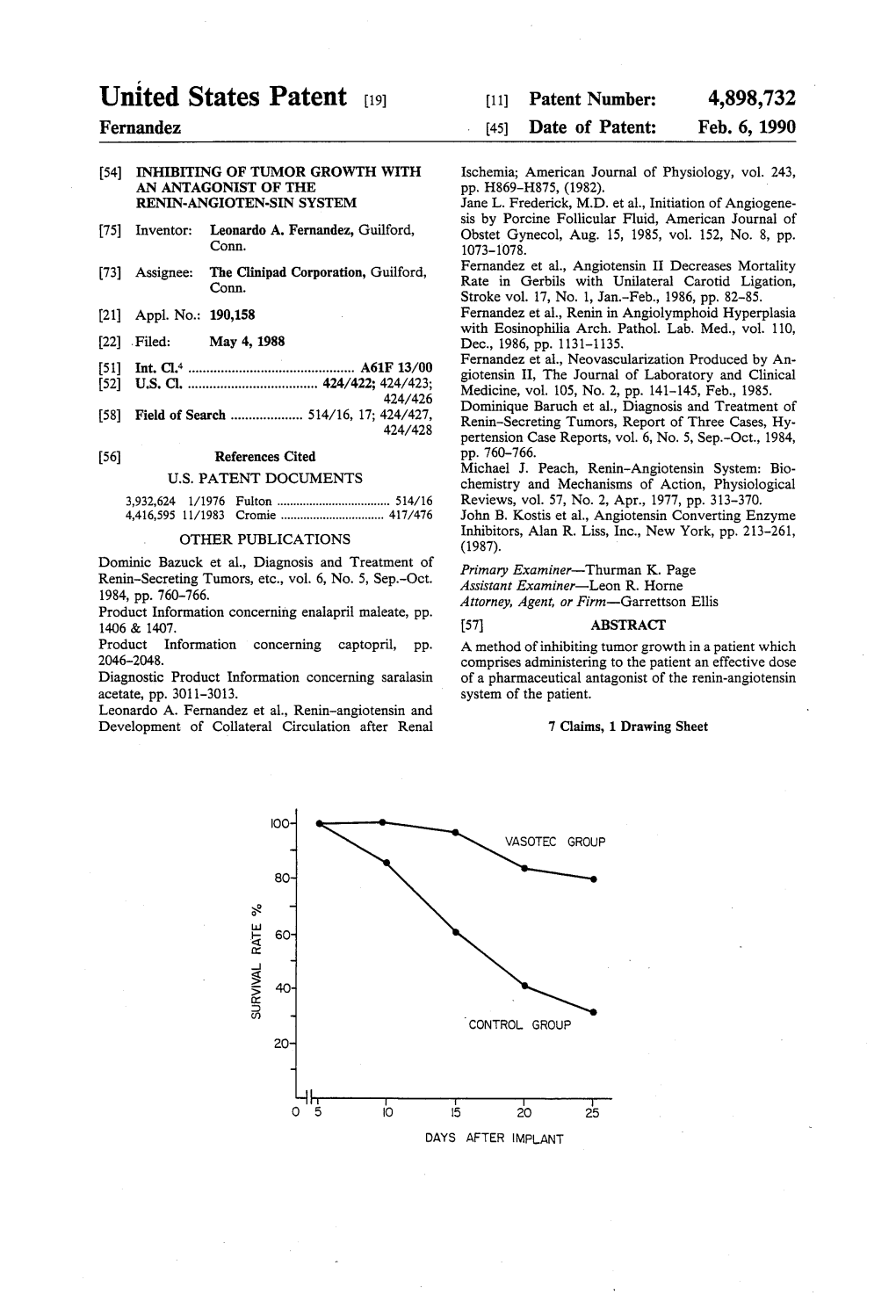
Survival Rate%
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Title 16. Crimes and Offenses Chapter 13. Controlled Substances Article 1
TITLE 16. CRIMES AND OFFENSES CHAPTER 13. CONTROLLED SUBSTANCES ARTICLE 1. GENERAL PROVISIONS § 16-13-1. Drug related objects (a) As used in this Code section, the term: (1) "Controlled substance" shall have the same meaning as defined in Article 2 of this chapter, relating to controlled substances. For the purposes of this Code section, the term "controlled substance" shall include marijuana as defined by paragraph (16) of Code Section 16-13-21. (2) "Dangerous drug" shall have the same meaning as defined in Article 3 of this chapter, relating to dangerous drugs. (3) "Drug related object" means any machine, instrument, tool, equipment, contrivance, or device which an average person would reasonably conclude is intended to be used for one or more of the following purposes: (A) To introduce into the human body any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (B) To enhance the effect on the human body of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (C) To conceal any quantity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; or (D) To test the strength, effectiveness, or purity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state. (4) "Knowingly" means having general knowledge that a machine, instrument, tool, item of equipment, contrivance, or device is a drug related object or having reasonable grounds to believe that any such object is or may, to an average person, appear to be a drug related object. -

Drugs for Primary Prevention of Atherosclerotic Cardiovascular Disease: an Overview of Systematic Reviews
Supplementary Online Content Karmali KN, Lloyd-Jones DM, Berendsen MA, et al. Drugs for primary prevention of atherosclerotic cardiovascular disease: an overview of systematic reviews. JAMA Cardiol. Published online April 27, 2016. doi:10.1001/jamacardio.2016.0218. eAppendix 1. Search Documentation Details eAppendix 2. Background, Methods, and Results of Systematic Review of Combination Drug Therapy to Evaluate for Potential Interaction of Effects eAppendix 3. PRISMA Flow Charts for Each Drug Class and Detailed Systematic Review Characteristics and Summary of Included Systematic Reviews and Meta-analyses eAppendix 4. List of Excluded Studies and Reasons for Exclusion This supplementary material has been provided by the authors to give readers additional information about their work. © 2016 American Medical Association. All rights reserved. 1 Downloaded From: https://jamanetwork.com/ on 09/28/2021 eAppendix 1. Search Documentation Details. Database Organizing body Purpose Pros Cons Cochrane Cochrane Library in Database of all available -Curated by the Cochrane -Content is limited to Database of the United Kingdom systematic reviews and Collaboration reviews completed Systematic (UK) protocols published by by the Cochrane Reviews the Cochrane -Only systematic reviews Collaboration Collaboration and systematic review protocols Database of National Health Collection of structured -Curated by Centre for -Only provides Abstracts of Services (NHS) abstracts and Reviews and Dissemination structured abstracts Reviews of Centre for Reviews bibliographic -

(12) Patent Application Publication (10) Pub. No.: US 2007/0293552 A1 Gorczynski (43) Pub
US 20070293552A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2007/0293552 A1 Gorczynski (43) Pub. Date: Dec. 20, 2007 (54) ANTIHYPERTENSIVE THERAPY METHOD Publication Classification (76) Inventor: Richard J. Gorczynski, Westminster, (51) Int. Cl. CO (US) A6II 3/42 (2006.01) (52) U.S. Cl. .............................................................. S14/378 Correspondence Address: (57) ABSTRACT HARNESS, DICKEY, & PIERCE, P.L.C Methods and therapeutic combinations are provided for 7700 BONHOMME, STE 400 lowering blood pressure in a Subject exhibiting resistance to ST. LOUIS, MO 63105 (US) a baseline antihypertensive therapy with one or more drugs, or a subject having diabetes and/or chronic kidney disease. A method of the invention comprises administering, in some (21) Appl. No.: 11/761,499 embodiments adjunctively with a modified baseline therapy, a compound of formula (I) as defined herein. A therapeutic (22) Filed: Jun. 12, 2007 combination of the invention comprises a compound of formula (I); at least one diuretic; and at least one antihy pertensive drug selected from ACE inhibitors, angiotensin II Related U.S. Application Data receptor blockers, beta-adrenergic receptor blockers and calcium channel blockers; wherein the at least one diuretic (60) Provisional application No. 60/813.966, filed on Jun. and/or the at least one antihypertensive drug are present at 15, 2006. substantially less than a full dose. US 2007/0293552 A1 Dec. 20, 2007 ANTHYPERTENSIVE THERAPY METHOD signaling pathways. While antagonism of the ETA receptor is known to reduce endothelin-mediated vasoconstriction, 0001. This application claims the benefit of U.S. provi antagonism of the endothelin-B (ET) receptor can block sional application Ser. -

ACE2 As a Therapeutic Target for COVID-19; Its Role in Infectious Processes and Regulation by Modulators of the RAAS System
Journal of Clinical Medicine Review ACE2 as a Therapeutic Target for COVID-19; Its Role in Infectious Processes and Regulation by Modulators of the RAAS System Veronique Michaud 1,2, Malavika Deodhar 1, Meghan Arwood 1, Sweilem B Al Rihani 1, Pamela Dow 1 and Jacques Turgeon 1,2,* 1 Tabula Rasa HealthCare Precision Pharmacotherapy Research & Development Institute, Orlando, FL 32827, USA; [email protected] (V.M.); [email protected] (M.D.); [email protected] (M.A.); [email protected] (S.B.A.R.); [email protected] (P.D.) 2 Faculty of Pharmacy, Université de Montréal, Montreal, QC H3C 3J7, Canada * Correspondence: [email protected]; Tel.: +856-938-8793 Received: 11 June 2020; Accepted: 2 July 2020; Published: 3 July 2020 Abstract: Angiotensin converting enzyme 2 (ACE2) is the recognized host cell receptor responsible for mediating infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). ACE2 bound to tissue facilitates infectivity of SARS-CoV-2; thus, one could argue that decreasing ACE2 tissue expression would be beneficial. However, ACE2 catalytic activity towards angiotensin I (Ang I) and II (Ang II) mitigates deleterious effects associated with activation of the renin-angiotensin-aldosterone system (RAAS) on several organs, including a pro-inflammatory status. At the tissue level, SARS-CoV-2 (a) binds to ACE2, leading to its internalization, and (b) favors ACE2 cleavage to form soluble ACE2: these actions result in decreased ACE2 tissue levels. Preserving tissue ACE2 activity while preventing ACE2 shredding is expected to circumvent unrestrained inflammatory response. Concerns have been raised around RAAS modulators and their effects on ACE2 expression or catalytic activity. -

Comparative Study of an Angiotensin-II Analog and a Converting Enzyme Inhibitor
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Kidney International, Vol. 17 (1980), pp. 647-653 Comparative study of an angiotensin-JI analog and a converting enzyme inhibitor ROBERT H. FAGARD, ANTOON K. AMERY, PAUL J. LIJNEN, and TONY M. REYBROUCK Hypertension and Cardiovascular Rehabilitation Unit, Department of Pathophysiology, University of Leuven, Leuven, Belgium Comparative study of an angiotensin-Il analog and a converting The angiotensin-Il (All) analog sar1 ala8-angioten- enzyme inhibitor. The effects of an angiotensin-Il analog (sarala- sin II, a specific antagonist of the vascular effects of sin, iv.) and of a converting enzyme inhibitor (captopril, oral) were compared in 12 sodium-depleted patients with hyper- All [1], has been studied intensively in patients with tension. The decrease of the mean intraarterial pressure (MAP) hypertension, and is a powerful hypotensive agent with captopril (—21.5 [sEM] 4.3mm Hg) was more pronounced in sodium-volume-depleted hypertensive patients (P <0.001)than the change of MAP during saralasin (—10.5 4.0mm Hg). The pretreatment arterial plasma renin activity (log except in patients with low plasma renin values. Its PRA) was closely related to the change of MAP during saralasin effect to lower blood pressure is indeed closely re- (r =—0.94;P <0.001)and also to the captopril-induced change lated to the plasma levels of renin or All [2-5], and of MAP(r —0.82; P <0.001); similar results were obtained for the log plasma angiotensin (PA) I and II levels. -

Medication for Military Aircrew: Current Use, Issues
RTO-TR-014 AC/323(HFM-014)TP/14 NORTH ATLANTIC TREATY ORGANIZATION RTO-TR-014 RESEARCH AND TECHNOLOGY ORGANIZATION BP 25, 7 RUE ANCELLE, F-92201 NEUILLY-SUR-SEINE CEDEX, FRANCE RTO TECHNICAL REPORT 14 Medication for Military Aircrew: Current Use, Issues, and Strategies for Expanded Options (les M´edicaments pour les equipages´ militaires : Consommation actuelle, questions et strat´egies pour des options elargies)´ Report of the Human Factors and Medicine Panel (HFM) Working Group 26. Published June 2001 Distribution and Availability on Back Cover 7KLVSDJHKDVEHHQGHOLEHUDWHO\OHIWEODQN 3DJHLQWHQWLRQQHOOHPHQWEODQFKH RTO-TR-014 AC/323(HFM-014)TP/14 NORTH ATLANTIC TREATY ORGANIZATION RESEARCH AND TECHNOLOGY ORGANIZATION BP 25, 7 RUE ANCELLE, F-92201 NEUILLY-SUR-SEINE CEDEX, FRANCE RTO TECHNICAL REPORT 14 Medication for Military Aircrew: Current Use, Issues, and Strategies for Expanded Options (les M´edicaments pour les equipages´ militaires : Consommation actuelle, questions et strat´egies pour des options elargies)´ Authors: EDIGER Mark, M.D. (US) Working Group Chairman BENSON, Alan J. (UK), DANESE, Daniele (IT), DAVIDSON, Ronald A., (CA), DOIREAU, Philippe (FR), ELIOPOULOS, Themis (GR), GRAY, Gary W. (CA), LAM, Berry (NL), NICHOLSON, Anthony A., (UK), PARIS, Jean-Fran¸cois, (FR), PICKARD, Jeb S., (US), PIERARD, C. (FR) Co-Authors: GOURBAT, Jean-Pierre (FR), LAGARDE, D. (FR), LALLEMENT G., (FR), PERES, M. (FR), RODIG,¨ E. (GE), STONE, Barbara M. (UK), TURNER, Claire (UK) Report of the Human Factors and Medicine Panel (HFM) Working Group 26. The Research and Technology Organization (RTO) of NATO RTO is the single focus in NATO for Defence Research and Technology activities. Its mission is to conduct and promote cooperative research and information exchange. -

Direct Renin Inhibitor: Aliskiren in Chronic Kidney Disease
Direct Renin Inhibitor: Aliskiren in Chronic Kidney Disease 1* 1 Yoshiyuki Morishita , Eiji Kusano 1 Division of Nephrology, Department of Medicine, Jichi Medical University, Tochigi, Japan * Corresponding author: Yoshiyuki Morishita, Division of Nephrology, Department of Medicine, Jichi Medical University, 3311-1, Yakushiji, Shimotsuke-city, 329-0498, Tochigi, Japan. Tel.: + 81-285447346, Fax: +81-285444869, E-mail: [email protected] ABSTRACT The renin-angiotensin-aldosterone system (RAAS) plays pivotal roles in the pathogenesis of chronic kidney disease (CKD) progression and its increased complications such as hypertension (HT) and cardiovascular diseases (CVD). Previ- ous studies suggested that aliskiren a direct renin inhibitor, blocks RAAS and may be effective for the management of CKD and its complications. This review focuses on the effects of aliskiren on CKD. Keywords: Kidney Failure, Chronic; Renin-Angiotensin System; Aliskiren; Blood Pressure; Cardiovascular Diseases Copyright © 2013, Kowsar Corp.; Published by Kowsar Corp. 1. Introduction prevent the development and progression of CKD and its complications such as HT and CVD (9-14). Recent evi- Aliskiren is an orally active nonpeptide direct renin in- dences suggest that aliskiren would be effective for CKD hibitor, which acts by binding to the active site of renin management and its complications such as HT and CVD (1). Aliskiren directly inhibits plasma renin activity (PRA), (15-21). This review focuses on clinical studies that have which acts at the initial and rate-limiting step in the re- demonstrated the effects of aliskiren on CKD. nin-angiotensin-aldosterone system (RAAS), unlike the blockade of RAAS by angiotensin I-converting enzyme 2. RAAS in CKD inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) which cause a reactive rise in PRA (2). -
Telmisartan Versus Angiotension-Converting
Journal of Human Hypertension (2009) 23, 339–349 & 2009 Macmillan Publishers Limited All rights reserved 0950-9240/09 $32.00 www.nature.com/jhh ORIGINAL ARTICLE Telmisartan versus angiotension- converting enzyme inhibitors in the treatment of hypertension: a meta-analysis of randomized controlled trials Z Zou1,3, G-L Xi2,3, H-B Yuan1, Q-F Zhu1 and X-Y Shi1 1Department of Anesthesiology, Changzheng Hospital, Second Military Medical University, Shanghai, People’s Republic of China and 2Center for New Drug Evaluation, Institute of Basic Medical Science, Second Military Medical University, Shanghai, People’s Republic of China Telmisartan and angiotensin-converting enzyme inhibi- 0.33–2.62). Telmisartan also showed a greater DBP tors (ACEIs) are both effective and widely used response rate than enalapril (relative risk (RR) 1.15, antihypertensive drugs targeting renin–angiotensin– 95% CI 1.05–1.26), ramipril (RR 1.34, 95% CI 1.11–1.61) aldosterone system. The study aimed to estimate the and perindopril (RR 1.22, 95% CI 1.05–1.41). There was efficacy and tolerability of telmisartan in comparison no statistical difference in DBP reduction or therapeutic with different ACEIs as monotherapy in the treatment of response rate between telmisartan and lisinopril (WMD hypertension. Cochrane Central Register of Controlled À0.30, 95% CI À0.65 to 0.05; RR 0.99, 95% CI 0.80–1.23, Trials, PubMed and Embase were searched for relevant respectively). Telmisartan had fewer drug-related studies. A meta-analysis of all randomized controlled adverse events than enalapril (RR 0.57, 95% CI 0.44–0.74), trials fulfilling the predefined criteria was performed. -
AHRQ%Systematic%Review%Surveillance% Program%
AHRQ%Systematic%Review%Surveillance% Program% " CER$#34:$Angiotensin"Converting"Enzyme"Inhibitors" (ACEIs),"Angiotensin"II"Receptor"Antagonists"(ARBs)," and"Direct"Renin"Inhibitors"for"Treating"Essential" Hypertension"–"An"Update"" $ $ Original$Release$Date:$June"2011""" Surveillance$Report$Date:$March"2016"" $ Summary$of$Key$Findings$from$Surveillance$ Report:$ 1)" Key"Question"1:"Conclusions"on"the"effectiveness"of"the"ACEIs" and"ARBs"included"in"the"original"systematic"review"are"likely" current."However,"one"new"RCT"found"that"the"ARB"azilsartan"–" approved"after"the"original"systematic"review"was"published,"may" be"more"effective"than"ramipril"(ACEI)"at"improving"systolic"BP."In" addition,"one"new"RCT"found"that"aliskiren"(DRI)"and"irbesartan" (ARB)"had"similar"effects"on"glucose"and"lipid"profiles."No" evidence"had"previously"been"identified."Finally,"while"the"original" review"found"no"evidence"comparing"ACEIs"or"ARBs"on" progression"to"type"II"diabetes,"we"identified"one"retrospective" cohort"study"which"found"a"lower"risk"of"type"II"diabetes"onset" associated"with"candesartan"(ARB)"as"compared"to"enalapril" (ACEI)."All"other"conclusions"are"likely"current.""" 2)" Key"Question"2:"Conclusions"on"withdrawal"rates"due"to"adverse" events"associated"with"the"ACEIs"and"ARBs"included"in"the" original"systematic"review"are"likely"current."However,"we" identified"an"RCT"examining"the"new"ARB"azilsartan,"which"found" lower"withdrawal"rates"associated"with"azilsartan"as"compared"to" ramipril"(ACEI)."All"other"conclusions"are"likely"current."Of"note," -

Harmonized Tariff Schedule of the United States (2004) -- Supplement 1 Annotated for Statistical Reporting Purposes
Harmonized Tariff Schedule of the United States (2004) -- Supplement 1 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2004) -- Supplement 1 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABACAVIR 136470-78-5 ACEXAMIC ACID 57-08-9 ABAFUNGIN 129639-79-8 ACICLOVIR 59277-89-3 ABAMECTIN 65195-55-3 ACIFRAN 72420-38-3 ABANOQUIL 90402-40-7 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABCIXIMAB 143653-53-6 ACITEMATE 101197-99-3 ABECARNIL 111841-85-1 ACITRETIN 55079-83-9 ABIRATERONE 154229-19-3 ACIVICIN 42228-92-2 ABITESARTAN 137882-98-5 ACLANTATE 39633-62-0 ABLUKAST 96566-25-5 ACLARUBICIN 57576-44-0 ABUNIDAZOLE 91017-58-2 ACLATONIUM NAPADISILATE 55077-30-0 ACADESINE 2627-69-2 ACODAZOLE 79152-85-5 ACAMPROSATE 77337-76-9 ACONIAZIDE 13410-86-1 ACAPRAZINE 55485-20-6 ACOXATRINE 748-44-7 ACARBOSE 56180-94-0 ACREOZAST 123548-56-1 ACEBROCHOL 514-50-1 ACRIDOREX 47487-22-9 ACEBURIC ACID 26976-72-7 -
Karvea, INN-Irbesartan
SCIENTIFIC DISCUSSION This module reflects the initial scientific discussion and scientific discussion on procedures which have been finalised before 1 September 2004. For scientific information on procedures after this date please refer to module 8B. 1. Introduction Inhibition of the renin-angiotensin system is a well proven approach to the treatment of arterial hypertension. It can be achieved by inhibiting the angiotensin-converting enzyme (ACE) that converts angiotensin I into its active form angiotensin II, or by blockade of angiotensin II (type AT1) receptors. AprovelKarvea is an oral formulation containing irbesartan, a selective antagonist of the AT1 receptors. Two antihypertensive agents of the same class (angiotensin II receptor antagonist) have previously been authorised, losartan and valsartan. 2. Part II: Chemical and pharmaceutical aspects Composition The product is available in the form of tablets containing a dose of 75, 150 or 300 mg of irbesartan. Tablets containing each dosage are identified by a corresponding code. The quantitative and qualitative composition was adequately described. The accelerated and long-term stability data demonstrated the suitability and compatibility of irbesartan with the packaging system (opaque blister pack in polyvinylchloride with a coating of heat sealed polyvinylidene chloride). Clinical trials formulations Both capsules and tablets were used in clinical trials. The trial dosage formulations including injectable and oral solutions and their method of manufacture were adequately described. Data from three bioequivalence studies showed that irbesartan tablets and capsules used in the clinical trials were bioequivalent. Development pharmaceutics Irbesartan was successfully formulated into a stable, immediate release tablet. The excipients were selected on the basis of their functionality and compatibility with the active substance. -
Chemical Structure-Related Drug-Like Criteria of Global Approved Drugs
Molecules 2016, 21, 75; doi:10.3390/molecules21010075 S1 of S110 Supplementary Materials: Chemical Structure-Related Drug-Like Criteria of Global Approved Drugs Fei Mao 1, Wei Ni 1, Xiang Xu 1, Hui Wang 1, Jing Wang 1, Min Ji 1 and Jian Li * Table S1. Common names, indications, CAS Registry Numbers and molecular formulas of 6891 approved drugs. Common Name Indication CAS Number Oral Molecular Formula Abacavir Antiviral 136470-78-5 Y C14H18N6O Abafungin Antifungal 129639-79-8 C21H22N4OS Abamectin Component B1a Anthelminithic 65195-55-3 C48H72O14 Abamectin Component B1b Anthelminithic 65195-56-4 C47H70O14 Abanoquil Adrenergic 90402-40-7 C22H25N3O4 Abaperidone Antipsychotic 183849-43-6 C25H25FN2O5 Abecarnil Anxiolytic 111841-85-1 Y C24H24N2O4 Abiraterone Antineoplastic 154229-19-3 Y C24H31NO Abitesartan Antihypertensive 137882-98-5 C26H31N5O3 Ablukast Bronchodilator 96566-25-5 C28H34O8 Abunidazole Antifungal 91017-58-2 C15H19N3O4 Acadesine Cardiotonic 2627-69-2 Y C9H14N4O5 Acamprosate Alcohol Deterrant 77337-76-9 Y C5H11NO4S Acaprazine Nootropic 55485-20-6 Y C15H21Cl2N3O Acarbose Antidiabetic 56180-94-0 Y C25H43NO18 Acebrochol Steroid 514-50-1 C29H48Br2O2 Acebutolol Antihypertensive 37517-30-9 Y C18H28N2O4 Acecainide Antiarrhythmic 32795-44-1 Y C15H23N3O2 Acecarbromal Sedative 77-66-7 Y C9H15BrN2O3 Aceclidine Cholinergic 827-61-2 C9H15NO2 Aceclofenac Antiinflammatory 89796-99-6 Y C16H13Cl2NO4 Acedapsone Antibiotic 77-46-3 C16H16N2O4S Acediasulfone Sodium Antibiotic 80-03-5 C14H14N2O4S Acedoben Nootropic 556-08-1 C9H9NO3 Acefluranol Steroid