Hospital Authority Annual Plan 2005/06 I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WTO GPA Statistical Report 2010-Revised 3Rd Version (
STATISTICS REPORTED UNDER ARTICLE XIX : 5 OF THE AGREEMENT ON GOVERNMENT PROCUREMENT OF THE WORLD TRADE ORGANIZATION, GENEVA PERIOD : 1.1.2010 - 31.12.2010 HONG KONG, CHINA ENTITY: HOSPITAL AUTHORITY Table of Content Part A - Reports Report No. 1 - Statistics on estimated number and value of contracts awarded for products and services, both equal or above and below the threshold value Report No. 2 - Statistics on total number and value of contracts awarded equal or above the threshold value, broken down by categories of products and services, under open, selective and limited tendering procedures Report No. 3 - Statistics on total number and value of contracts awarded under each of the cases of Article XV, paragraph 1 - limited tendering, broken down by categories of products and services Report No. 4 - Statistics on total number and value of contracts awarded for products and (where necessary) services under derogations to the Agreement Part B - Global Statistics and Details on Contracts Awarded for Products and Services to Individual Countries/Regions Part A Report No. 1 Article XIX Paragraph 5(a) Statistics on estimated number and value of contracts awarded, both equal or above and below the threshold value Tendering Procedures Equal or Above the Threshold Value Below the Threshold Value Total Construction Construction Construction Goods Services Services Goods Services Services Goods Services Services Open (No.) 99 12 - - - - 99 12 - (Value in 180,640.59 95,881.70 - - - - 180,640.59 95,881.70 - '000 SDR) Selective(No.) 1 - 2 - - - 1 - 2 (Value in 1,269.54 - 31,229.86 - - - 1,269.54 - 31,229.86 '000 SDR) Limited (No.) 76 1 - - - - 76 1 - (Value in 186,083.54 745.89 - - - - 186,083.54 745.89 - '000 SDR) Grand Total :(No.) 176 13 2 - - - 176 13 2 (Value in 367,993.67 96,627.59 31,229.86 - - - 367,993.67 96,627.59 31,229.86 '000 SDR) Notes : There may be a slight discrepancy between the sum of individual items and the total as shown in the tables owing to rounding. -
BMJ Open Is Committed to Open Peer Review. As Part of This Commitment We Make the Peer Review History of Every Article We Publish Publicly Available
BMJ Open: first published as 10.1136/bmjopen-2018-023070 on 15 October 2018. Downloaded from BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email [email protected] http://bmjopen.bmj.com/ on September 29, 2021 by guest. Protected copyright. BMJ Open BMJ Open: first published as 10.1136/bmjopen-2018-023070 on 15 October 2018. Downloaded from 10-year Risk Prediction Models of Complications and Mortality of Diabetes Mellitus in Chinese Patients in Primary Care in Hong Kong study protocol ForJournal: peerBMJ Open review only Manuscript ID bmjopen-2018-023070 Article Type: Protocol Date Submitted by the Author: 19-Mar-2018 Complete List of Authors: -

Infrastructure Development and Heritage Conservation
213 Chapter 12 Infrastructure Development and Heritage Conservation While developing the infrastructure for Hong Kong’s economic growth, the Government is enriching the city’s living environment at the same time through conservation and revitalisation. Organisational Framework The Development Bureau was established on July 1, 2007 following the reorganisation of the Government Secretariat’s Policy Bureaux. It consists of two policy branches: Planning and Lands, and Works. The Development Opportunities Office was set up under the Bureau in 2009. The Planning and Lands Branch is responsible for policy governing planning, development, land use and supply, urban renewal, building safety, and land registration. Its policy objectives are to facilitate Hong Kong’s continual development through effective planning and use of land, a steady and sufficient supply of land, efficient registration of land, promoting and ensuring building safety and timely maintenance, and expediting urban renewal. The Works Branch is responsible for formulating public works policies and co-ordinating and monitoring the implementation of public works projects. It also takes charge of policy matters concerning greening, water supply, slope safety, and flood prevention as well as heritage conservation. The Development Bureau oversees the Planning Department, Lands Department, Buildings Department, Land Registry, Architectural Services Department, Civil Engineering and Development Department, Drainage Services Department, Electrical and Mechanical Services Department, and Water Supplies Department. The reorganisation of these nine government departments under one roof ensures more efficient co-ordination and resolution of inter-departmental issues relating to infrastructure development at an early stage. The Development Bureau is also responsible for enhancing the Government’s heritage conservation work and striking a balance between development and 214 Infrastructure Development and Heritage Conservation conservation. -

Report of the Steering Committee on Review of Hospital Authority
Report of the Steering Committee on Review of Hospital Authority July 2015 CONTENTS Glossary .................................................................................................................. iii Executive Summary ................................................................................................ v Chapter 1 Introduction ...................................................................................... 1 Chapter 2 Work of the Steering Committee ...................................................... 6 Chapter 3 Major Challenges Facing the Hospital Authority ............................ 9 Chapter 4 Management and Organisation Structure ....................................... 13 Chapter 5 Resource Management ................................................................... 26 Chapter 6 Staff Management .......................................................................... 42 Chapter 7 Cost Effectiveness and Service Management ................................ 59 Chapter 8 Overall Management and Control .................................................. 87 Chapter 9 Conclusion ...................................................................................... 96 Annex 1 Membership of the Steering Committee on Review of Hospital Authority ....................................................................................... 102 Annex 2 Report of the Public Engagement Programme ............................. 103 Annex 3 Clustering of Hospitals and Institutions ...................................... -
活化@Heritage Issue No. 11
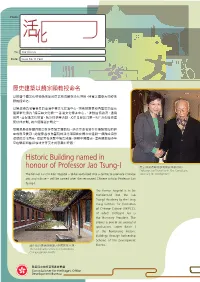
From: 活化歷史建築通訊 A Newsletter on Revitalisation To: Our friends Date: Issue No.11 February 2010 歷史建築以饒宗頤教授命名 以推廣中國文化藝術為宗旨的原荔枝角醫院活化項目,將會以國學大師饒宗 頤 教 授 命 名。 以饒教授為名譽會長的香港中華文化促進中心,將會把原荔枝角醫院的歷史 建 築 群 化 身 為「饒 宗 頤 文 化 館 — 香港文化傳承中心」,推動國情教育、通識 教育,並促進文化欣賞,陶冶性情等活動。項目是發展局第一期「活化歷史建 築伙伴計劃」的六個獲選計劃之一。 發展局局長林鄭月娥日前拜會饒宗頤教授。她表示命名旨在表揚饒教授的超 卓成就及貢獻。她說原荔枝角醫院的活化項目旨在鬧市中建設一個融合自然 環境的文化園林,使訪客在休閒中增長知識,瞭解中國歷史。這與饒教授多年 來在學術和藝術領域作育英才的宏願相呼應。 Historic Building named in honour of Professor Jao Tsung-I 饒宗頤教授與發展局局長林鄭月娥。 Professor Jao Tsung-I with Mrs Carrie Lam, The former Lai Chi Kok Hospital – to be revitalised into a centre to promote Chinese Secretary for Development. arts and culture – will be named after the renowned Chinese scholar Professor Jao Tsung-I. The former hospital is to be transformed into the Jao Tsung-I Academy by the Hong Kong Institute for Promotion of Chinese Culture (HKIPCC), of which Professor Jao is the Honorary President. The project is one of six successful applications under Batch I of the Revitalising Historic Buildings Through Partnership Scheme of the Development 活化後的建築群將融入中國園林主題。 Bureau. The revitalised premise will incorporate Chinese garden motifs. 發展局文物保育專員辦事處 Commissioner for Heritage’s Office 1 Development Bureau 饒宗頤教授是享負盛名的國學大師,從事學術研究和藝術創作超過八十 年。饒 教 授 治 學 範 圍 廣 泛,涉及 文、史、哲、藝 各 個 領 域,集 歷 史 學 家、考 古 學 家、文 學 家、經 學 家、教 育 家 和 書 畫 家 於 一 身。年 屆 九十 多 歲 的 饒 教 授近年仍創作不斷,例如以古意渾穆的筆法製作裝置於大嶼山的「心經簡 林」。饒教授曾先後於香港大學、新加坡大學及香港中文大學任教,並獲 多所著名學府委任為客座教授。 政府將於今年第二季就「饒宗頤文化館」活化工程向立法會申請撥款,整 個項目可望在2012年 中 落 成。 The Secretary for Development, Mrs Carrie Lam, recently met with Professor Jao. -

The Chinese University of Hong Kong Department of Psychiatry Schedule for November, 2018
for favour of posting dated on: 2018/11/01 The Chinese University of Hong Kong Department of Psychiatry Schedule for November, 2018 Date Time Activity Speaker/Team Nov 1 16:30-17:30 Clinical Neuroscience Seminar* Dr. Sandra Chan Journal Club - Pleasure system in the brain Nov 8 14:30-16:00 Academic Lecture* Dr. Kelly Lai Support for students with mental health problems in Associate Professor the school setting: an overview of the School Mental Department of Psychiatry Health Support Scheme in Hong Kong CUHK 16:00-17:30 Clinical Case Conference* Child Team A case from school mental health support scheme - “A Buddha like student” Nov 15 14:30-16:30 Quality Assurance Meeting (TPH) All Clinical Staff Nov 22 14:30-16:30 Quality Assurance Meeting (SH) All Clinical Staff 16:30-17:30 Clinical Forum/Research Meeting (SH) 14:30-16:00 Psychotherapy Case Conference* Dr. Iris Lai, Jenny Kwok, Teresa Good enough daughter Chan, Irene Kam 16:00-16:45 Psychotherapy Supervision* Dr. Teresa Chan, Irene Kam Nov 29 14:30-16:00 Academic Lecture* Prof. Tatia Lee Neurobiological basis of affective processing Head of Department Department of Psychology HKU 16:00-17:30 Skills Workshop*# Prof. Linda Lam, Dr. Victor Lui How to prepare a medical report #Please note there will be no CME credits. Venue: *Seminar Room TPH SH G/F, Multicentre Conference Room 1 Dining Room Tai Po Hospital G/F, Wing D Ward 7AB Tai Po, N.T. Tai Po Hospital Dept. of Psychiatry Tai Po, N.T. 7/F, Shatin Hospital Shatin, N.T. -

27 June 2011 Doctor the Honourable KL Leung Chairman, Panel On
LC Paper No. CB(2)2239/10-11(06) 27 June 2011 Doctor the Honourable KL Leung Chairman, Panel on Health Services Legislative Council Secretariat Legislative Council Building 8 Jackson Road, Central Hong Kong Dear Dr Leung, Re: Implementation of Hospital Accreditation in Hong Kong Public Hospitals We are writing to you as a group of local surveyors, trained and appointed by the Australian Council on Healthcare Standards (ACHS), involved in the hospital accreditation programme. We are grateful to you and the Panel on Health Services for inviting us to express our views regarding the implementation of hospital accreditation in Hong Kong. Hong Kong surveyors are an assemblage of healthcare professionals and executives with vast experience in clinical services and healthcare management. We come from diversified background of clinical, nursing, allied health and administrative disciplines, both in the private and public sectors. We have in particular one thing in common- we are all staunch advocates of quality and safety. We are keen to support and see the full implementation of hospital accreditation in Hong Kong. Hospital accreditation is a well recognized tool for continuous quality improvement in the healthcare setting. With rising concerns about patient safety and desire for quality healthcare, hospital accreditation is gaining popularity and wide acceptance globally. As surveyors, we can attest to the usefulness and relevance of hospital accreditation locally. Having been involved in the pilot scheme, we have witnessed the dedication and Page 1 of 7 commitment of healthcare workers in using accreditation as the tool to bolster quality in domains such as clinical safety, care efficacy and patient experience in alignment with international standards. -

Batch III of Revitalising Historic Buildings Through Partnership Scheme Press Conference
Batch III of Revitalising Historic Buildings Through Partnership Scheme Press Conference 7 October 2011 Background of Revitalising Historic Buildings Through Partnership Scheme z In the 2007-08 Policy Address, the Chief Executive announced a range of initiatives to enhance heritage conservation. z Launching of “Revitalising Historic Buildings Through Partnership Scheme” to put Government-owned historic buildings to good adaptive re-use. z The Government has reserved $2 billion for the “Revitalising Historic Buildings Through Partnership Scheme” (including revitalising the Former Police Married Quarters on Hollywood Road into “PMQ”). 2 2 1 Objectives of Revitalising Historic Buildings Through Partnership Scheme z To preserve and put historic buildings into good and innovative use. z To transform historic buildings into unique cultural landmarks. z To promote active public participation in the conservation of historic buildings. z To create job opportunities, in particular at the district level. 3 3 Set up of the Advisory Committee on Revitalisation of Historic Buildings z The Committee is chaired by Mr Bernard Chan with 9 non- official members from the fields of historical research, architecture, surveying, social enterprise, finance, etc. z To provide advice on the implementation of the Revitalisation Scheme and other revitalisation projects. z To help assess applications under the Scheme. z To monitor the subsequent operation of the selected projects. 4 4 2 Assessment Criteria of Revitalising Historic Buildings Through Partnership Scheme The Advisory Committee examines and assesses the applications in accordance with the following five assessment criteria: z Reflection of historical value and significance z Technical aspects z Social value and social enterprise operation z Financial viability z Management capability and other considerations 5 5 Review of Batch I of Revitalisation Scheme z Batch I of the Revitalisation Scheme was launched in February 2008. -

Cb(1)816/08-09(04)
立法會 Legislative Council LC Paper No. CB(1)816/08-09(04) Ref: CB1/PL/DEV Panel on Development Meeting on 24 February 2009 Background brief on Revitalizing Historic Buildings Through Partnership Scheme Purpose This paper provides background information on the Revitalizing Historic Buildings Through Partnership Scheme (Revitalization Scheme), and a summary of the concerns and views expressed by Members when the subject was discussed at the relevant committees of the Legislative Council. Background 2. In his 2007-2008 Policy Address, the Chief Executive announced that Government would seek to revitalize Government-owned historic buildings by introducing a new scheme which would allow non-governmental organizations to apply for adaptive re-use of these buildings. On 11 October 2007, the Development Bureau issued a Legislative Council Brief on Heritage Conservation Policy [File Ref : DEVB(CR)(W) 1-55/68/01] which set out, inter alia, the general framework of the scheme, titled as "Revitalising Historic Buildings Through Partnership Scheme". Modus operandi of the Revitalization Scheme First batch historic buildings 3. The following seven buildings1 are the first batch of historic buildings included in the Revitalization Scheme -- 1 Details of these buildings are provided in Annex 1 to LC Paper No. CB(2)637/07-08(03). - 2 - - Old Tai Po Police Station; - Lui Seng Chun; - Lai Chi Kok Hospital; - North Kowloon Magistracy; - Old Tai O Police Station; - Fong Yuen Study Hall; and - Mei Ho House. Eligibility of applicants 4. The Administration has adopted the social enterprise (SE) approach whereby non-profit-making non-governmental organizations (NGOs) were invited to submit proposals on a competitive basis to revitalize the historic buildings and the proposed usage should take the form of a SE. -
Paper on Provision of Obstetric Services in the Tseung
立法會 Legislative Council LC Paper No. CB(2)486/12-13(05) Ref : CB2/PL/HS Panel on Health Services Background brief prepared by the Legislative Council Secretariat for the meeting on 21 January 2013 Provision of obstetric services in the Tseung Kwan O Hospital Purpose This paper summarizes the concerns of the members of the Panel on Health Services ("the Panel") on the provision of obstetric services in the Tseung Kwan O Hospital ("TKOH"). Background 2. The Kowloon East Cluster serves the population of Kwun Tong, Tseung Kwan O ("TKO") and Sai Kung districts which have an estimated population of 980 000. There are three hospitals in the cluster, namely, United Christian Hospital ("UCH"), TKOH and Haven of Hope Hospital. With the rapid increase of population in TKO and Sai Kung, the existing facilities in TKOH are inadequate in terms of space and capacity to meet the future service requirements and service demand in the Kowloon East Cluster. In July 2008, the Finance Committee approved a sum of $1,945 million in money-of-the-day prices for a major renovation and expansion project at TKOH. The TKOH expansion project includes, among others, the establishment of obstetric wards, Neonatal Intensive Care Unit ("NICU") as well as Special Care Baby Unit to provide the necessary facilities for the development of obstetric and neonatal services in TKOH. The whole project is targeted for completion by late 2013-2014. - 2 - 3. HA has also planned to commission the obstetric and NICU services in TKOH in phases, from enhancement of antenatal and postnatal services, delivery of low risk pregnancies to the provision of a full scale service. -

New Acute Hospital at Kai Tak Development Area
Task Force on Kai Tak Harbourfront Development For discussion on 23 May 2018 TFKT/06/2018 New Acute Hospital at Kai Tak Development Area PURPOSE This paper seeks Members’ views on the preliminary design concept of the New Acute Hospital (NAH) at Kai Tak Development Area (KTDA) by the Hospital Authority (HA), ahead of the upcoming procurement of the Foundation Works. Further development of the overall design will be carried out during the next Work Stage and presented to the Task Force on Kai Tak Harbourfront Development expected in 2019. BACKGROUND 2. To meet the long-term demand for healthcare services and facilities in Kowloon arising from the growing and ageing population, the Government has reserved sites in KTDA for hospital development. The Kai Tak Development is a major project covering the ex-airport site, together with adjoining districts of Kowloon City, Wong Tai Sin and Kwun Tong. The KTDA will have a mix of housing, community, business, tourism and infrastructural uses. With the Government’s plan to strive for increasing the development intensity in Kai Tak Development, the population of KTDA is to be increased to about 134 000 upon completion of the planned developments in KTDA. 3. There are currently eight hospitals or institutions in the Kowloon Central Cluster (KCC), namely Queen Elizabeth Hospital, Kowloon Hospital, Hong Kong Buddhist Hospital, Hong Kong Eye Hospital, Kwong Wah Hospital, Wong Tai Sin Hospital, Our Lady of Maryknoll Hospital and Hong Kong Red Cross Blood Transfusion Service Headquarters. HA formulated the Clinical Services Plan (CSP) for KCC in 2016 providing an overarching clinical strategy to align and inform the future services developments in KCC. -

Administration's Paper on Progress Report on Heritage Conservation
LC Paper No. CB(1)456/18-19(05) For discussion on 22 January 2019 Legislative Council Panel on Development Progress Report on Heritage Conservation Initiatives Purpose This paper updates Members on the progress of the heritage conservation initiatives since our last report to the Panel in October 2017. Heritage Conservation Policy Policy statement 2. As promulgated in 2007, the Government seeks “to protect, conserve and revitalise as appropriate historical and heritage sites and buildings through relevant and sustainable approaches for the benefit and enjoyment of present and future generations. In implementing this policy, due regard should be given to development needs in the public interest, respect for private property rights, budgetary considerations, cross-sector collaboration and active engagement of stakeholders and the general public.” Statutory monument declaration system 3. In accordance with section 3 of the Antiquities and Monuments Ordinance (Cap. 53) (the “Ordinance”), the Antiquities Authority (i.e. the Secretary for Development) may, after consultation with the Antiquities Advisory Board (“AAB”) and with the approval of the Chief Executive, by notice in the Gazette, declare any place, building, site or structure, which the Authority considers to be of public interest by reason of its historical, archaeological or palaeontological significance, to be a monument. Monuments are subject to statutory protection provided 1 under the Ordinance. Pursuant to section 6 of the Ordinance, the protection includes prohibition of any excavation, carrying on building or other works on the monument, and any action to demolish, remove, obstruct, deface or interfere with the monument unless a permit is granted by the Antiquities Authority.