Arthropod Envenomations: Immunologic and Toxicologic Considerations Cyrus Rangan, MD, FAAP, ACMT
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Western Black Widow Spider
Arachnida Western Black Widow Spider Class Order Family Species Arachnida Araneae Theridiidae Latrodectus hesperus Range Reproduction Special Adaptations The genus is worldwide. Growth: gradual, molts several times. Venom: Although never Western Texas, Okla- Egg: produced in bunches of 40 or more, wrapped in silk and sus- aggressive, the females homa and Kansas north pended from the web, can hatch within a week of being laid. occasionally bite hu- to Canada and west to the Immature: pure white after hatching and slowly gaining color with each mans but only in self defense (males do not Pacific Coaststates molt. Adult: may live for several years. The female can store sperm for many bite humans). They months. It is a fallacy that the female always eats the male after can cause a serious but Habitat mating. rarely fatal result. The venom is neurotoxic and Found in tropical, temper- Physical Characteristics is reported to be 15 times ate and arid zones in a as poisonous as that of the rattlesnake. Symptoms multitude of habitats. Mouthparts: chelicerate, fangs are perpendicular to body line. Duct from a include a painful tight- poison gland opens from the base of each fang. The mouth and ening of the abdomenal jaws are on the underside of the head. Niche wall muscles, increased Legs: 8 long, narow legs. blood pressure and body Eyes: 8 eyes. Usually found in temperature, nausea, lo- Egg: their eggs are layed in clusters and covered with silk to undisturbed places like calized edema, asphyxia form an egg sac. wood piles, outhouses, and convulsions. Medical Immature: white at first , gaining color with each molt. -

Spider Bites
Infectious Disease Epidemiology Section Office of Public Health, Louisiana Dept of Health & Hospitals 800-256-2748 (24 hr number) www.infectiousdisease.dhh.louisiana.gov SPIDER BITES Revised 6/13/2007 Epidemiology There are over 3,000 species of spiders native to the United States. Due to fragility or inadequate length of fangs, only a limited number of species are capable of inflicting noticeable wounds on human beings, although several small species of spiders are able to bite humans, but with little or no demonstrable effect. The final determination of etiology of 80% of suspected spider bites in the U.S. is, in fact, an alternate diagnosis. Therefore the perceived risk of spider bites far exceeds actual risk. Tick bites, chemical burns, lesions from poison ivy or oak, cutaneous anthrax, diabetic ulcer, erythema migrans from Lyme disease, erythema from Rocky Mountain Spotted Fever, sporotrichosis, Staphylococcus infections, Stephens Johnson syndrome, syphilitic chancre, thromboembolic effects of Leishmaniasis, toxic epidermal necrolyis, shingles, early chicken pox lesions, bites from other arthropods and idiopathic dermal necrosis have all been misdiagnosed as spider bites. Almost all bites from spiders are inflicted by the spider in self defense, when a human inadvertently upsets or invades the spider’s space. Of spiders in the United States capable of biting, only a few are considered dangerous to human beings. Bites from the following species of spiders can result in serious sequelae: Louisiana Office of Public Health – Infectious Disease Epidemiology Section Page 1 of 14 The Brown Recluse: Loxosceles reclusa Photo Courtesy of the Texas Department of State Health Services The most common species associated with medically important spider bites: • Physical characteristics o Length: Approximately 1 inch o Appearance: A violin shaped mark can be visualized on the dorsum (top). -

ALLERGIC REACTIONS/ANAPHYLAXIS Connie J
Northwest Community EMS System Paramedic Education Program ALLERGIC REACTIONS/ANAPHYLAXIS Connie J. Mattera, M.S., R.N., EMT-P Reading assignments Text-Vol.1 pp. 235, 1272-1276 SOP: Allergic Reactions/ Anaphylactic Shock Assumed knowledge: Drugs: Epinephrine 1:1,000, 1:10,000; albuterol, ipratropium, dopamine, glucagon KNOWLEDGE OBJECTIVES Upon reading the assigned text assignments and completion of the class and homework questions, each participant will independently do the following with at least an 80% degree of accuracy and no critical errors: 1. Define allergic reaction. 2. Describe the incidence, morbidity and mortality of allergic reactions and anaphylaxis. 3. Identify risk factors that predispose a patient to anaphylaxis. 4. Explain the physiology of the immune system following exposure to an allergen including activation of histamine receptors and the formation of antibodies. 5. Discuss the pathophysiology of allergic reactions and anaphylaxis. 6. Describe the common modes by which allergens enter the body. 7. Compare and contrast natural and acquired and active vs. passive immunity. 8. Identify antigens most frequently associated with anaphylaxis. 9. Differentiate the clinical presentation and severity of risk for a mild, moderate and severe allergic reaction with an emphasis on recognizing an anaphylactic reaction. 10. Integrate the pathophysiologic principles of anaphylaxis with treatment priorities. 11. Sequence care per SOP for patients with mild, moderate and severe allergic reactions. CJM: S14 NWC EMSS Paramedic Education Program ALLERGIC REACTIONS/ANAPHYLAXIS Connie J. Mattera, M.S., R.N., EMT-P I. Immune system A. Principal body system involved in allergic reactions. Others include the cutaneous, cardiovascular, respiratory, nervous, and gastrointestinal systems. -
Approach and Management of Spider Bites for the Primary Care Physician
Osteopathic Family Physician (2011) 3, 149-153 Approach and management of spider bites for the primary care physician John Ashurst, DO,a Joe Sexton, MD,a Matt Cook, DOb From the Departments of aEmergency Medicine and bToxicology, Lehigh Valley Health Network, Allentown, PA. KEYWORDS: Summary The class Arachnida of the phylum Arthropoda comprises an estimated 100,000 species Spider bite; worldwide. However, only a handful of these species can cause clinical effects in humans because many Black widow; are unable to penetrate the skin, whereas others only inject prey-specific venom. The bite from a widow Brown recluse spider will produce local symptoms that include muscle spasm and systemic symptoms that resemble acute abdomen. The bite from a brown recluse locally will resemble a target lesion but will develop into an ulcerative, necrotic lesion over time. Spider bites can be prevented by several simple measures including home cleanliness and wearing the proper attire while working outdoors. Although most spider bites cause only local tissue swelling, early species identification coupled with species-specific man- agement may decrease the rate of morbidity associated with bites. © 2011 Elsevier Inc. All rights reserved. More than 100,000 species of spiders are found world- homes and yards in the southwestern United States, and wide. Persons seeking medical attention as a result of spider related species occur in the temperate climate zones across bites is estimated at 50,000 patients per year.1,2 Although the globe.2,5 The second, Lactrodectus, or the common almost all species of spiders possess some level of venom, widow spider, are found in both temperate and tropical 2 the majority are considered harmless to humans. -
Instruction Sheet: Bee Sting, Local Reaction
University of North Carolina Wilmington Abrons Student Health Center INSTRUCTION SHEET: BEE STING, LOCAL REACTION The Student Health Provider has diagnosed a mild allergic reaction to a bee/wasp sting. Fortunately, most bee stings are not serious and cause only temporary swelling, redness, and pain at the sting site. Rarely, a whole-body allergic reaction occurs; shock can result. The stinger, if still in the wound, should be removed; if the stinger is left in place, bee toxin continues to enter the body, increasing the reaction. A stinger should be removed with a piece of paper or credit card, using a sideways scraping motion. A pair of tweezers can also be used to remove the stinger, but try not to squeeze the stinger, or more toxin can be pushed inside the wound. Realize that swelling may increase at first, even with treatment. Measures can be taken, however, to minimize the reaction to bee stings. MEASURES YOU SHOULD TAKE TO HELP TREAT YOUR BEE STING: 1. Rest and elevate the affected body part. Rest and elevation help reduce swelling and pain. 2. Apply cold packs to the area off-and-on for the first 24 hours after injury. Cold helps ease discomfort, and minimizes additional swelling. Do not apply ice directly to the area, causing discomfort. Rather, aim for coolness, yet comfort, applying a layer or two of cloth between the cold pack and affected area. 3. Take over-the-counter antihistamines: In the morning, take a non-sedating antihistamine such as loratadine, 10 mg daily. At night, take diphenhydramine (Benadryl), 25 mg, 1 or 2 every 6 hours for itching and swelling. -

Prioritization of Health Services
PRIORITIZATION OF HEALTH SERVICES A Report to the Governor and the 74th Oregon Legislative Assembly Oregon Health Services Commission Office for Oregon Health Policy and Research Department of Administrative Services 2007 TABLE OF CONTENTS List of Figures . iii Health Services Commission and Staff . .v Acknowledgments . .vii Executive Summary . ix CHAPTER ONE: A HISTORY OF HEALTH SERVICES PRIORITIZATION UNDER THE OREGON HEALTH PLAN Enabling Legislatiion . 3 Early Prioritization Efforts . 3 Gaining Waiver Approval . 5 Impact . 6 CHAPTER TWO: PRIORITIZATION OF HEALTH SERVICES FOR 2008-09 Charge to the Health Services Commission . .. 25 Biennial Review of the Prioritized List . 26 A New Prioritization Methodology . 26 Public Input . 36 Next Steps . 36 Interim Modifications to the Prioritized List . 37 Technical Changes . 38 Advancements in Medical Technology . .42 CHAPTER THREE: CLARIFICATIONS TO THE PRIORITIZED LIST OF HEALTH SERVICES Practice Guidelines . 47 Age-Related Macular Degeneration (AMD) . 47 Chronic Anal Fissure . 48 Comfort Care . 48 Complicated Hernias . 49 Diagnostic Services Not Appearing on the Prioritized List . 49 Non-Prenatal Genetic Testing . 49 Tuberculosis Blood Test . 51 Early Childhood Mental Health . 52 Adjustment Reactions In Early Childhood . 52 Attention Deficit and Hyperactivity Disorders in Early Childhood . 53 Disruptive Behavior Disorders In Early Childhood . 54 Mental Health Problems In Early Childhood Related To Neglect Or Abuse . 54 Mood Disorders in Early Childhood . 55 Erythropoietin . 55 Mastocytosis . 56 Obesity . 56 Bariatric Surgery . 56 Non-Surgical Management of Obesity . 58 PET Scans . 58 Prenatal Screening for Down Syndrome . 59 Prophylactic Breast Removal . 59 Psoriasis . 59 Reabilitative Therapies . 60 i TABLE OF CONTENTS (Cont’d) CHAPTER THREE: CLARIFICATIONS TO THE PRIORITIZED LIST OF HEALTH SERVICES (CONT’D) Practice Guidelines (Cont’d) Sinus Surgery . -

110 Mapas De Distribución De Arañas De Importancia
MAPAS DE DISTRIBUCIÓN DE ARAÑAS DE IMPORTANCIA MÉDICA DEL GÉNERO Latrodectus (ARANEAE: THERIDIIDAE) PARA NORTEAMÉRICA. Rodrigo Monjaraz-Ruedas. Colección Nacional de Arácnidos (CNAN), Departamento de Zoología, Instituto de Biología, Universidad Nacional Autónoma de México. Apartado Postal 70-153, C.P. 04510, Ciudad Universitaria, Distrito Federal, México. E-mail: [email protected]. RESUMEN. Las especies de arañas pertenecientes al género Latrodectus Walckenaer, 1805 son consideradas de importancia médica, debido a la toxicidad de su veneno, el cual representa un riesgo de salud para el ser humano. Se realizó una búsqueda exhaustiva de las localidades en literatura especializada y de material depositado en la Colección Nacional de Arácnidos (CNAN) del Instituto de Biología, UNAM, en la cual han sido registradas las especies con mayor número de registros para Norteamérica: Latrodectus mactans (Fabricius, 1775), Latrodectus variolus Walckenaer, 1837 y Latrodectus geometricus C. L. Koch, 1841. Las localidades fueron georeferenciadas con la ayuda de GEOlocate y Google Earth, mientras que los mapas de registros para las tres especies se elaboraron con el programa gvSIG. Con la elaboración de estos mapas, se pretende incrementar el conocimiento sobre la distribución de las especies con mayores registros en Norteamérica del género Latrodectus, dicha información podrá ser utilizada por el sector médico de los países norteamericanos. Palabras clave: Latrodectus, distribución, importancia médica, Norteamérica. ABSTRACT. The spiders of the genus Latrodectus Walcknaer, 1805 are considered of medical importance, because the toxicity of their venom represents an important health risk to humans. We performed an exhaustive search of the literature and locations of material deposited in Colección Nacional de Arácnidos (CNAN) of the Instituto de Biología, UNAM, for the species that have the highest number of records for North America: Latrodectus mactans (Fabricius, 1775), Latrodectus variolus Walckenaer, 1837 and Latrodectus geometricus C. -
Integrating Climate Change Vulnerability Assessments Into Adaptation Planning
Integrating climate change vulnerability assessments into adaptation planning A case study using the NatureServe Climate Change Vulnerability Index to inform conservation planning for species in Florida A Report Prepared for the Florida Fish and Wildlife Conservation Commission Natalie Dubois, Astrid Caldas, Judy Boshoven & Aimee Delach Defenders of Wildlife is a national, nonprofit, membership organization dedicated to the protection of all native wild animals and plants in their natural communities. Jamie Rappaport Clark, President Donald Barry, Executive Vice President This report was made possible with the generous support of the Doris Duke Charitable Foundation, the Kresge Foundation and the Educational Foundation of America AUTHORS Natalie Dubois Astrid Caldas Judy Boshoven Aimee Delach With additional input from Amielle DeWan and Kathleen Theoharides PRODUCTION Claire Colegrove © 2011 Defenders of Wildlife, 1130 17th St NW, Washington D.C. 20036 http:/www.defenders.org Disclaimer: This document represents the work and views of the authors and does not necessarily imply endorsement by the Florida Fish and Wildlife Conservation Commission. Suggested citation: Dubois, N., A. Caldas, J. Boshoven, and A. Delach. 2011. Integrating Climate Change Vulnerability Assessments into Adaptation Planning: A Case Study Using the NatureServe Climate Change Vulnerability Index to Inform Conservation Planning for Species in Florida [Final Report]. Defenders of Wildlife, Washington D.C. CONTENTS Executive Summary ................................................................................... -
Apple-Cider Vinegar Dab the Vinegar Onto Each Bite with a Paper Towel
STRUCK OR BITTEN OR INJURED BY…. BY THE NUMBERS…… 2010 2011 • #3 IN WC CLAIMS • #5 IN WC CLAIMS FOR FOR MAINTENANCE MAINTENANCE • 3 WC CLAIMS FOR • 1 CLAIM THUS 2010 FAR FOR 2011 • $2,456 INCURRED • $550 INCURRED AVOIDING A BEE STING • STAND STILL, MOST TIMES THEY AREN’T ATTACKING, THEY’RE JUST CURIOUS ABOUT YOUR SMELL & WHY YOUR NEAR THEIR HOME • FAST MOVEMENTS MAKE YOU THE AGGRESSOR • IF A BEE HAS BEEN AROUND FOR MORE THAN A MINUTE YOUR IN ITS TERRITORY. LEAVE THE AREA. JOG IN A STRAIGHT LINE FOR A FEW SECONDS TO GAIN DISTANCE. BEES GIVE UP THE CHASE IF YOU’RE TOO FAR AWAY. • DON’T ZIG ZAG, THE BEE CAN FOLLOW YOUR SCENT & ZIGZAGGING MAKES FOR A LOT OF RUNNING BUT NOT A LOT OF DISTANCE. AVOIDING A BEE STING • A CIRCLING BEE ISN’T MAD, ITS SCENT GLANDS MAY BE AGITATED BY A GROOMING PRODUCT, ITS SIMPLY SEEKING THE SOURCE • A BEE DOESN’T KNOW WHAT YOUR ROLLED UP NEWSPAPER IS. ALL YOUR DOING IS MAKING IT MAD AT CLOSE RANGE. • BAD MOVE… BEES ARE HAPPY TO FOLLOW YOUR SCENT TO THE WATER & STING YOUR FACE WHEN YOU RESURFACE. “PRIMARY STINGERS” • HORNET- SLEEK, USUALLY NESTS IN TREES, CAN STING MULTIPLE TIMES • WASP-SLEEK, AERIAL OR BURIED NEST, CAN STING MULTIPLE TIMES • YELLOW JACKET-DISTINCTIVE BLACK & YELLOW-BANDED WASP, AERIAL OR BURIED NEST, CAN STING MULTIPLE TIMES “PRIMARY STINGERS” • BUMBLEBEE- BIG, FUZZY, SLOW FLYER; BURIED NEST, CAN STING MULTIPLE TIMES • HONEYBEE- RELATIVELY SMALL, NESTS IN TREES & WOOD, STINGS ONCE. Consider Dust Mites • They're invisible to the naked eye, but not to your health – Found in most every home or business – Live in the fine layer of dust that continually settles on any surface – Are nearly impossible to see – Astoundingly, up to 500 dust mites can be found in a single gram of particulate dust. -
Widow Spider Parasitoids Philolema Latrodecti
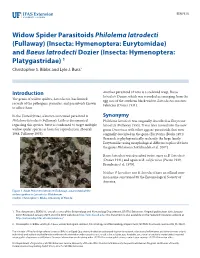
EENY515 Widow Spider Parasitoids Philolema latrodecti (Fullaway) (Insecta: Hymenoptera: Eurytomidae) and Baeus latrodecti Dozier (Insecta: Hymenoptera: Platygastridae) 1 Christopher S. Bibbs and Lyle J. Buss2 Introduction Another parasitoid of note is a scelionid wasp, Baeus latrodecti Dozier, which was recorded as emerging from the The genus of widow spiders, Latrodectus, has limited egg sacs of the southern black widow, Latrodectus mactans records of the pathogens, parasites, and parasitoids known Fabricius (Dozier 1931). to affect them. In the United States, a known associated parasitoid is Synonymy Philolema latrodecti (Fullaway). Little is documented Philolema latrodecti was originally described as Eurytoma regarding this species, but it is confirmed to target multiple latrodecti (Fullaway 1953). It was later moved into the new widow spider species as hosts for reproduction (Boucek genus Desantisca with other egg sac parasitoids that were 1988, Fullaway 1953). originally described in the genus Eurytoma (Burks 1971). Research to phylogenetically reclassify the large family Eurytomidae using morphological differences placed it into the genus Philolema (Lotfalizadeh et al. 2007). Baeus latrodecti was described twice, once as B. latrodecti (Dozier 1931) and again as B. californicus (Pierce 1939, Krombein et al. 1979). Neither P. latrodecti nor B. latrodecti have an official com- mon name sanctioned by the Entomological Society of America. Figure 1. Adult Philolema latrodecti (Fullaway), a parasitoid of the widow spiders in Latrodectus Walckenaer. Credits: Christopher S. Bibbs, University of Florida 1. This document is EENY515, one of a series of the Entomology and Nematology Department, UF/IFAS Extension. Original publication date January 2012. Reviewed January 2019. Visit the EDIS website at http://edis.ifas.ufl.edu. -

Population Dynamics of the Red Widow Spider (Araneae: Theridiidae)
Carrel: Red Widow Spider Populations 385 POPULATION DYNAMICS OF THE RED WIDOW SPIDER (ARANEAE: THERIDIIDAE) JAMES E. CARREL Division of Biological Sciences, 105 Tucker Hall, University of Missouri-Columbia, Columbia, MO 65211-7400 ABSTRACT Populations of the red widow spider, Latrodectus bishopi, in native Florida scrub at the Arch- bold Biological Station were monitored annually on ten ~0.5 ha transects in late winter from 1987 to 2000. Of 398 L. bishopi detected in the study, all but three had their silken retreats built in palmetto leaves. L. bishopi at rest in retreats in saw palmetto (Serenoa repens) were higher above the ground (~0.5 m) than spiders in scrub palmetto (Sabal etonia) (~0.3 m). From a peak of 31 spiders/ha in 1989, the average L. bishopi density declined exponentially to only 0.3 spiders/ha in 1997, after which L. bishopi densities began to recover. Burning of scrubby transects in spring or summer appeared to have no affect on subsequent L. bishopi populations. There were no significant correlations between L. bishopi population density and local temperature or precipitation data. These results suggest that undescribed biotic factors may regulate populations of the red widow spider in a density-dependent fashion. Key Words: Latrodectus, Florida scrub, ecology, populations, dynamics, fire RESUMEN En diez transectos de ~0.5 ha, determinamos cada invierno de 1987-2000 las poblaciones de la araña Latrodectus bishopi en matorral nativo de Florida en la Estación Biológica Arch- bold. De las 398 L. bishopi que encontramos, todos menos tres habían construido sus retiros sedosus entre las ojas de palmitos. -
Bees, Part 1: Characteristics, Reactions, and Management
CLOSE ENCOUNTERS WITH THE ENVIRONMENT What’s Eating You? Bees, Part 1: Characteristics, Reactions, and Management MAJ Felisa S. Lewis, MC, USA; Laurie J. Smith, MD Bee stings are common in the United States. Classification and Characteristics of Bees We review the characteristics of bumblebees, Insects in the order Hymenoptera, meaning “mem- honeybees, and Africanized honeybees; the types brane wings,” have 2 sets of front and hind wings and pathophysiology of sting reactions; and the that are connected by a series of little hooks called medical management and prevention of bee hamuli. A constriction in the abdomen distinguishes stings. In part 2 of this series, we will discuss these insects from similar-looking insects, such as the use of venom immunotherapy, the diagnosis flies.5 The order is large and includes not only bees of systemic mastocytosis that initially presents as (family Apidae) but also wasps and hornets (family anaphylaxis, and the efficacy of immunotherapy Vespidae) and ants (family Formicidae).2,6 Although in patients with mastocytosis. there are many types of bees, only bumblebees (genus Cutis. 2007;79:439-444. Bombus) and honeybees (including the Africanized honeybee, genus Apis) are considered of medical importance and will be the only ones addressed in this s members of the order Hymenoptera, bees article. The female aculeate (Aculeata, a suborder of deliver a venom-producing sting with which Hymenoptera, referring to the stinging capabilities A many people have had personal experience. of these insects) can inject its venom from a gland With 0.5% to 3.0% of the US population consid- or sac (singularly or in pairs) through an ovipositor ered allergic to venomous stings,1,2 and an average (a long tapered structure on the posterior portion of of 48 reported deaths annually in the United States their body)(Figure 1).