Studies of Salvinorin-Based Antagonists to Elucidate Pertinent Interactions for Kappa Opioid Receptor Antagonism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

INVESTIGATION of NATURAL PRODUCT SCAFFOLDS for the DEVELOPMENT of OPIOID RECEPTOR LIGANDS by Katherine M
INVESTIGATION OF NATURAL PRODUCT SCAFFOLDS FOR THE DEVELOPMENT OF OPIOID RECEPTOR LIGANDS By Katherine M. Prevatt-Smith Submitted to the graduate degree program in Medicinal Chemistry and the Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Philosophy. _________________________________ Chairperson: Dr. Thomas E. Prisinzano _________________________________ Dr. Brian S. J. Blagg _________________________________ Dr. Michael F. Rafferty _________________________________ Dr. Paul R. Hanson _________________________________ Dr. Susan M. Lunte Date Defended: July 18, 2012 The Dissertation Committee for Katherine M. Prevatt-Smith certifies that this is the approved version of the following dissertation: INVESTIGATION OF NATURAL PRODUCT SCAFFOLDS FOR THE DEVELOPMENT OF OPIOID RECEPTOR LIGANDS _________________________________ Chairperson: Dr. Thomas E. Prisinzano Date approved: July 18, 2012 ii ABSTRACT Kappa opioid (KOP) receptors have been suggested as an alternative target to the mu opioid (MOP) receptor for the treatment of pain because KOP activation is associated with fewer negative side-effects (respiratory depression, constipation, tolerance, and dependence). The KOP receptor has also been implicated in several abuse-related effects in the central nervous system (CNS). KOP ligands have been investigated as pharmacotherapies for drug abuse; KOP agonists have been shown to modulate dopamine concentrations in the CNS as well as attenuate the self-administration of cocaine in a variety of species, and KOP antagonists have potential in the treatment of relapse. One drawback of current opioid ligand investigation is that many compounds are based on the morphine scaffold and thus have similar properties, both positive and negative, to the parent molecule. Thus there is increasing need to discover new chemical scaffolds with opioid receptor activity. -

Biased Signaling by Endogenous Opioid Peptides
Biased signaling by endogenous opioid peptides Ivone Gomesa, Salvador Sierrab,1, Lindsay Lueptowc,1, Achla Guptaa,1, Shawn Goutyd, Elyssa B. Margolise, Brian M. Coxd, and Lakshmi A. Devia,2 aDepartment of Pharmacological Sciences, Icahn School of Medicine at Mount Sinai, New York, NY 10029; bDepartment of Physiology & Biophysics, Virginia Commonwealth University, Richmond, VA 23298; cSemel Institute for Neuroscience and Human Behavior, University of California, Los Angeles, CA 90095; dDepartment of Pharmacology & Molecular Therapeutics, Uniformed Services University, Bethesda MD 20814; and eDepartment of Neurology, UCSF Weill Institute for Neurosciences, University of California, San Francisco, CA 94143 Edited by Susan G. Amara, National Institutes of Health, Bethesda, MD, and approved April 14, 2020 (received for review January 20, 2020) Opioids, such as morphine and fentanyl, are widely used for the possibility that endogenous opioid peptides could vary in this treatment of severe pain; however, prolonged treatment with manner as well (13). these drugs leads to the development of tolerance and can lead to For opioid receptors, studies showed that mice lacking opioid use disorder. The “Opioid Epidemic” has generated a drive β-arrestin2 exhibited enhanced and prolonged morphine-mediated for a deeper understanding of the fundamental signaling mecha- antinociception, and a reduction in side-effects, such as devel- nisms of opioid receptors. It is generally thought that the three opment of tolerance and acute constipation (15, 16). This led to types of opioid receptors (μ, δ, κ) are activated by endogenous studies examining whether μOR agonists exhibit biased signaling peptides derived from three different precursors: Proopiomelano- (17–20), and to the identification of agonists that preferentially cortin, proenkephalin, and prodynorphin. -
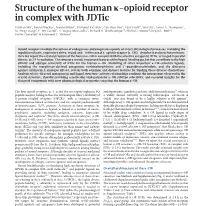
Structure of the Human Κ-Opioid Receptor in Complex with Jdtic
ARTICLE doi:10.1038/nature10939 Structure of the human k-opioid receptor in complex with JDTic Huixian Wu1, Daniel Wacker1, Mauro Mileni1, Vsevolod Katritch1, Gye Won Han1, Eyal Vardy2, Wei Liu1, Aaron A. Thompson1, Xi-Ping Huang2, F. Ivy Carroll3, S. Wayne Mascarella3, Richard B. Westkaemper4, Philip D. Mosier4, Bryan L. Roth2, Vadim Cherezov1 & Raymond C. Stevens1 Opioid receptors mediate the actions of endogenous and exogenous opioids on many physiological processes, including the regulation of pain, respiratory drive, mood, and—in the case of k-opioid receptor (k-OR)—dysphoria and psychotomimesis. Here we report the crystal structure of the human k-OR in complex with the selective antagonist JDTic, arranged in parallel dimers, at 2.9 A˚ resolution. The structure reveals important features of the ligand-binding pocket that contribute to the high affinity and subtype selectivity of JDTic for the human k-OR. Modelling of other important k-OR-selective ligands, including the morphinan-derived antagonists norbinaltorphimine and 59-guanidinonaltrindole, and the diterpene agonist salvinorin A analogue RB-64, reveals both common and distinct features for binding these diverse chemotypes. Analysis of site-directed mutagenesis and ligand structure–activity relationships confirms the interactions observed in the crystal structure, thereby providing a molecular explanation for k-OR subtype selectivity, and essential insights for the design of compounds with new pharmacological properties targeting the human k-OR. The four opioid receptors, m, d, k and the nociceptin/orphanin FQ antidepressants, anxiolytics and anti-addiction medications14, whereas peptide receptor, belong to the class A (rhodopsin-like) c subfamily of a widely abused, naturally occurring hallucinogen—salvinorin A G-protein-coupled receptors (GPCRs)1 with a common seven- (SalA)—was also found to be a highly selective k-OR agonist15. -

The Effects of Morphine, Naloxone, and Оє Opioid Manipulation On
Neuroscience 287 (2015) 32–42 THE EFFECTS OF MORPHINE, NALOXONE, AND j OPIOID MANIPULATION ON ENDOCRINE FUNCTIONING AND SOCIAL BEHAVIOR IN MONOGAMOUS TITI MONKEYS (CALLICEBUS CUPREUS) B. J. RAGEN, a,b* N. MANINGER, b S. P. MENDOZA b AND Key words: titi monkey, mu opioid, pair-bonding, cortisol, K. L. BALES a,b monogamy, kappa opioid. a Psychology Department, University of California-Davis, One Shields Avenue, Davis, CA 95616, USA b California National Primate Research Center, One Shields INTRODUCTION Avenue, Davis, CA 95616, USA Socially monogamous species form long-term associations between two adults. In some species, Abstract—The l opioid receptor (MOR) and j opioid recep- these relationships have been shown to be classic tor (KOR) have been implicated in pair-bond formation and attachment bonds (Hazan and Shaver, 1987) and result maintenance in socially monogamous species. Utilizing in pair-mates spending considerable time in physical con- monogamous titi monkeys (Callicebus cupreus), the present tact with one another, providing social buffering, and study examined the potential role opioids play in modulat- exhibiting substantial behavioral and physiological agita- ing the response to separation, a potent challenge to the tion upon involuntary separation (Mason and Mendoza, pair-bond. In Experiment 1, paired male titi monkeys were separated from their pair-mate for 30-min and then received 1998). Due to the rarity of monogamy in mammals saline, naloxone (1.0 mg/kg), morphine (0.25 mg/kg), or the (Kleiman, 1977) there is a paucity of data on the neurobio- KOR agonist, U50,488 (0.01, 0.03, or 0.1 mg/kg) in a coun- logical underpinnings of adult attachment. -

1 TITLE PAGE Buprenorphine and Opioid Antagonism, Tolerance
JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 JPET FastThis Forward.article has not Published been copyedited on and November formatted. The 4, final 2010 version as DOI:10.1124/jpet.110.173823may differ from this version. JPET #173823 TITLE PAGE Buprenorphine and opioid antagonism, tolerance, and naltrexone-precipitated withdrawal Carol A. Paronis and Jack Bergman Downloaded from jpet.aspetjournals.org Preclinical Pharmacology Laboratory (C.A.P, J.B.) McLean Hospital/Harvard Medical School Belmont, MA at ASPET Journals on September 26, 2021 Department of Pharmaceutical Sciences (C.A.P.) Northeastern University Boston, MA 1 Copyright 2010 by the American Society for Pharmacology and Experimental Therapeutics. JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 This article has not been copyedited and formatted. The final version may differ from this version. JPET #173823 RUNNING TITLE PAGE Running Title: Buprenorphine antagonism, tolerance, and dependence Corresponding author: Carol A. Paronis, PhD Department of Pharmaceutical Sciences Northeastern University Downloaded from 211 Mugar Life Sciences Building Boston, MA 02115 jpet.aspetjournals.org Tel. (617) 373-3212 Fax. (617) 373-8886 Email: [email protected] at ASPET Journals on September 26, 2021 Number of: Pages - 20 Tables - 3 Figures - 5 References - 38 Number of words in: Abstract - 284 Introduction - 683 Discussion - 1258 2 JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 This article has not been copyedited and formatted. The final version may differ from this version. JPET #173823 ABSTRACT The dual antagonist effects of the mixed-action μ-opioid partial agonist/κ-opioid antagonist buprenorphine have not been previously compared in behavioral studies, and it is unknown whether they are comparably modified by chronic exposure. -

In Silico Results of Κ-Opioid Receptor Antagonists As Ligands for The
bioRxiv preprint doi: https://doi.org/10.1101/432468; this version posted October 3, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. In silico results of k-Opioid receptor antagonists as ligands for the second bromodomain of the Pleckstrin Homology Domain Interacting Protein Lemmer R. P. EL ASSAL ([email protected]) 25/08/2018 Abstract Pleckstrin Homology Domain Interacting Protein (PHIP) is a member of the BRWD1-3 Family (Bromodomain and WD repeat-containing proteins). PHIP (BRWD2, WDR11) contains a WD40 repeat (methyl-lysine binder) and 2 bromodomains (acetyl-lysine binder). It was discovered through interactions with the pleckstrin homology domain of Insulin Receptor Signalling (IRS) proteins and has been shown to mediate transcriptional responses in pancreatic islet cells and postnatal growth. An initial hit for the second bromodomain of PHIP (PHIP(2)) was discovered in 2012, with consecutive research yielding a candidate with a binding anity of 68mM. PHIP(2) is an atypical category III bromodomain with a threonine (THR1396) where an asparagine residue would usually be. In the standard case, this pocket holds four water molecules, but in the case of PHIP(2), there is room for one extra water molecule - also known as PHIP water, able to mediate interaction between THR1396 and the typical water network at the back of the binding pocket. We present rst ever results of two k-Opioid receptor (KOR) antagonists with distinct pharmacophores having an estimated binding anity in the nM to mM range, as well as higher binding anities for every currently discovered PHIP(2) ligand towards KOR. -

Potential of Buprenorphine/Naltrexone in Treating Polydrug Addiction and Co-Occurring Psychiatric Disorders
nature publishing group DEVELOPMENT Potential of Buprenorphine/Naltrexone in Treating Polydrug Addiction and Co-occurring Psychiatric Disorders DJ McCann1 In recent years, we have seen regulatory approval being therefore, any potential cocaine addiction pharmacotherapy given for several new pharmacotherapies in the treatment under serious consideration for regulatory filing requires evalu- of drug addiction disorders. Within the United States, the ation in subjects with comorbid cocaine/alcohol dependence. most noteworthy development has been the approval of Correspondingly, alcohol dependence was not an exclusion cri- buprenorphine in the treatment of opioid dependence, and terion when the National Institute on Drug Abuse conducted its availability for prescribing in an office-based setting a recent 210-subject, multi-site, placebo-controlled study of has resulted in thousands of additional patients going into modafinil for the treatment of cocaine dependence. A post-hoc treatment. Although approved medications for the treatment longitudinal analysis of the resulting data revealed a significant of cocaine and methamphetamine dependence are still effect of modafinil in decreasing cocaine use in subjects who lacking, the National Institute on Drug Abuse has devoted were not dependent on alcohol but this effect was lacking in substantial effort toward meeting these clinical needs.1 Recent alcohol-dependent subjects; in fact, compared to placebo, studies of modafinil for the treatment of cocaine dependence there was a nonsignificant trend toward increased cocaine use have been especially encouraging. Looking to the future, the with modafinil treatment in alcohol-dependent patients (A.M. looming challenge is polydrug addiction, a situation that is Elkashef; presented at the 69th Annual Scientific Meeting of often complicated by co-occurring psychiatric disorders. -

Therapeutic Potential of Kappa Opioids in Pain and Addiction”
KappaCon 2021 The 6th Conference on the “Therapeutic Potential of Kappa Opioids in Pain and Addiction” Program Committee....................................................1 Sponsors.....................................................................1 Kappa Code of Conduct..............................................2 Instructions for connecting to Zoom............................3 Instructions for connecting to gather.town...................3 Instructions for connecting to Slack.............................4 gather.town map..........................................................5 Session Schedule.......................................................6 Featured Sessions......................................................9 gather.town Poster Layout.........................................11 Poster Presentation List.............................................12 Oral Abstracts............................................................14 Poster Abstracts.........................................................48 Job Opportunities.......................................................74 Registration Contact List............................................76 Program Committee • Elyssa B. Margolis (UCSF), Program Chair • Ream Al-Hasani (Washington University) • Irwin Lucki (Uniformed Services University) • Nicolas Massaly (Washington University) • Abigail Polter (George Washington University) • Hugo Tejeda (NIMH-IRP) KappaCon Secretary: Charles Chavkin (University of Washington) Sponsors We are grateful for the generous support of these -

NIDA Drug Supply Program Catalog, 25Th Edition
RESEARCH RESOURCES DRUG SUPPLY PROGRAM CATALOG 25TH EDITION MAY 2016 CHEMISTRY AND PHARMACEUTICS BRANCH DIVISION OF THERAPEUTICS AND MEDICAL CONSEQUENCES NATIONAL INSTITUTE ON DRUG ABUSE NATIONAL INSTITUTES OF HEALTH DEPARTMENT OF HEALTH AND HUMAN SERVICES 6001 EXECUTIVE BOULEVARD ROCKVILLE, MARYLAND 20852 160524 On the cover: CPK rendering of nalfurafine. TABLE OF CONTENTS A. Introduction ................................................................................................1 B. NIDA Drug Supply Program (DSP) Ordering Guidelines ..........................3 C. Drug Request Checklist .............................................................................8 D. Sample DEA Order Form 222 ....................................................................9 E. Supply & Analysis of Standard Solutions of Δ9-THC ..............................10 F. Alternate Sources for Peptides ...............................................................11 G. Instructions for Analytical Services .........................................................12 H. X-Ray Diffraction Analysis of Compounds .............................................13 I. Nicotine Research Cigarettes Drug Supply Program .............................16 J. Ordering Guidelines for Nicotine Research Cigarettes (NRCs)..............18 K. Ordering Guidelines for Marijuana and Marijuana Cigarettes ................21 L. Important Addresses, Telephone & Fax Numbers ..................................24 M. Available Drugs, Compounds, and Dosage Forms ..............................25 -

A Phase 2A Study to Evaluate the Kappa Opioid Receptor As a Target
Study Title: A Phase 2a Study to Evaluate the Kappa Opioid Receptor As a Target for the Treatment of Mood and Anxiety Spectrum Disorders by Evaluation of Whether CERC-501 Engages Key Neural Circuitry Related to the Hedonic Response Version Date: October 06, 2016 NCT02218736 FAST-MAS KOR Phase 2a Study Protocol Version 6.0 Task Order #: HHSN27100004 Version Date 10/06/16 Contract #: HHSN271201200006I CLINICAL STUDY PROTOCOL Study Title: A Phase 2a Study to Evaluate the Kappa Opioid Receptor As a Target for the Treatment of Mood and Anxiety Spectrum Disorders by Evaluation of Whether CERC-501 Engages Key Neural Circuitry Related to the Hedonic Response Abbreviated Title: FAST-MAS KOR Phase 2a Protocol Version: 6.0 Version Date: October 06, 2016 Contract Title: New Experimental Medicine Studies: Fast-Fail Trials in Mood and Anxiety Spectrum Disorders (FAST-MAS) Contract #: HHSN271201200006I Contractor: Duke University Contract PI: Andrew D. Krystal, M.D., M.S. Professor, Department of Psychiatry and Behavioral Sciences Duke University Medical Center Box 3309 Durham, NC 27710 Task Order #: HHSN27100004 Overall Study PI: Andrew D. Krystal, M.D., M.S. Supported by: National Institute of Mental Health (NIMH) Confidential: This document and its contents are the property of the Duke Clinical Research Institute. The information contained herein is confidential and is to be used only in connection with matters authorized by Duke Clinical Research Institute. No portion of this document is to be disclosed to others without prior written permission of Duke Clinical Research Institute. Page 1 of 75 FAST-MAS KOR Phase 2a Study Protocol Version 6.0 Task Order #: HHSN27100004 Version Date 10/06/16 Contract #: HHSN271201200006I Abbreviated Study Title: FAST-MAS KOR Phase 2a Contract #: HHSN271201200006I Task Order #: HHSN27100004 Coordinating Center [CC]: Duke Clinical Research Institute (DCRI) Data center [DCC]: Duke Clinical Research Institute (DCRI) Phase of Study: Phase 2a Target enrollment: 90 Patients FDA Approval(s) IND No Yes Drug: CERC-501 IND #: 121225 held by Dr. -

Psychoactive Natural Products: Overview of Recent Developments
12 Ann Ist Super Sanità 2014 | Vol. 50, No. 1: 12-27 DOI: 10.4415/ANN_14_01_04 Psychoactive natural products: overview of recent developments István Ujváry REVIEWS iKem BT, Budapest, Hungary AND Abstract Natural psychoactive substances have fascinated the curious mind of shamans, artists, Key words ARTICLES scholars and laymen since antiquity. During the twentieth century, the chemical com- • ethnopharmacology position of the most important psychoactive drugs, that is opium, cannabis, coca and • mode of action “magic mushrooms”, has been fully elucidated. The mode of action of the principal in- • natural products gredients has also been deciphered at the molecular level. In the past two decades, the • psychopharmacology RIGINAL use of herbal drugs, such as kava, kratom and Salvia divinorum, began to spread beyond • toxicology O their traditional geographical and cultural boundaries. The aim of the present paper is to briefly summarize recent findings on the psychopharmacology of the most prominent psychoactive natural products. Current knowledge on a few lesser-known drugs, includ- ing bufotenine, glaucine, kava, betel, pituri, lettuce opium and kanna is also reviewed. In addition, selected cases of alleged natural (or semi-natural) products are also mentioned. O, mickle is the powerful grace that lies In herbs, plants, stones, and their true qualities William Shakespeare (Romeo and Juliet) INTRODUCTION Historical background of psychoactive natural During the past 200 years, there has been major pro- products research gress in our understanding of the composition and ef- The biochemical machinery of an organism generates fects of many psychoactive natural products, particular- many structurally related chemicals (Nature’s “combinato- ly those that have therapeutic uses. -

Dr. Chartoff's NIH Biosketch
OMB No. 0925-0001 and 0925-0002 (Rev. 10/15 Approved Through 10/31/2018) BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors. Follow this format for each person. DO NOT EXCEED FIVE PAGES. NAME: CHARTOFF, ELENA eRA COMMONS USER NAME (credential, e.g., agency login):ECHARTOFF POSITION TITLE: Assistant Professor EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable. Add/delete rows as necessary.) DEGREE Completion Date INSTITUTION AND LOCATION FIELD OF STUDY (if applicable) MM/YYYY Carnegie Mellon University, Pittsburgh, PA B.S. 06/1992 Biology University of Washington, Seattle, WA Ph.D. 05/2001 Neurobiology & Behavior Harvard Medical School, Belmont, MA Postdoctoral 08/2004 Behavioral Genetics fellow A. Personal Statement My research focuses on the neurobiological underpinnings of reward function and motivated behavior in the context of psychiatric disorders such as bipolar disorder, depression, and drug addiction. A major biological question in my laboratory is how neural circuits act under normal circumstances to regulate mood and how these circuits can be disrupted to produce mood disorders. In this context, we are investigating the role of kappa opioid receptor systems and AMPA glutamate receptors in limbic brain regions such as the nucleus accumbens, amygdala, and prefrontal cortex in reward function. To accomplish this, we are using pharmacological and molecular genetic approaches to selectively enhance or disrupt kappa opioid or AMPA receptor-related signaling pathways within these limbic circuits in order to determine causal relationships between these systems and affective states.