A Phase 2A Study to Evaluate the Kappa Opioid Receptor As a Target
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(12) Patent Application Publication (10) Pub. No.: US 2004/0224020 A1 Schoenhard (43) Pub
US 2004O224020A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2004/0224020 A1 Schoenhard (43) Pub. Date: Nov. 11, 2004 (54) ORAL DOSAGE FORMS WITH (22) Filed: Dec. 18, 2003 THERAPEUTICALLY ACTIVE AGENTS IN CONTROLLED RELEASE CORES AND Related U.S. Application Data IMMEDIATE RELEASE GELATIN CAPSULE COATS (60) Provisional application No. 60/434,839, filed on Dec. 18, 2002. (76) Inventor: Grant L. Schoenhard, San Carlos, CA (US) Publication Classification Correspondence Address: (51) Int. Cl. ................................................... A61K 9/24 Janet M. McNicholas (52) U.S. Cl. .............................................................. 424/471 McAndrews, Held & Malloy, Ltd. 34th Floor (57) ABSTRACT 500 W. Madison Street Chicago, IL 60661 (US) The present invention relates to oral dosage form with active agents in controlled release cores and in immediate release (21) Appl. No.: 10/742,672 gelatin capsule coats. Patent Application Publication Nov. 11, 2004 Sheet 1 of 3 US 2004/0224020 A1 r N 2.S Hr s Patent Application Publication Nov. 11, 2004 Sheet 2 of 3 US 2004/0224020 A1 r CN -8 e N va N . t Cd NOLLYRILNONOO Patent Application Publication Nov. 11, 2004 Sheet 3 of 3 US 2004/0224020 A1 US 2004/0224020 A1 Nov. 11, 2004 ORAL DOSAGE FORMS WITH released formulations, a long t is particularly disadvan THERAPEUTICALLY ACTIVE AGENTS IN tageous to patients Seeking urgent treatment and to maintain CONTROLLED RELEASE CORES AND MEC levels. A second difference in the pharmacokinetic IMMEDIATE RELEASE GELATIN CAPSULE profiles of controlled release in comparison to immediate COATS release drug formulations is that the duration of Sustained plasma levels is longer in the controlled release formula CROSS REFERENCED APPLICATIONS tions. -

INVESTIGATION of NATURAL PRODUCT SCAFFOLDS for the DEVELOPMENT of OPIOID RECEPTOR LIGANDS by Katherine M
INVESTIGATION OF NATURAL PRODUCT SCAFFOLDS FOR THE DEVELOPMENT OF OPIOID RECEPTOR LIGANDS By Katherine M. Prevatt-Smith Submitted to the graduate degree program in Medicinal Chemistry and the Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Philosophy. _________________________________ Chairperson: Dr. Thomas E. Prisinzano _________________________________ Dr. Brian S. J. Blagg _________________________________ Dr. Michael F. Rafferty _________________________________ Dr. Paul R. Hanson _________________________________ Dr. Susan M. Lunte Date Defended: July 18, 2012 The Dissertation Committee for Katherine M. Prevatt-Smith certifies that this is the approved version of the following dissertation: INVESTIGATION OF NATURAL PRODUCT SCAFFOLDS FOR THE DEVELOPMENT OF OPIOID RECEPTOR LIGANDS _________________________________ Chairperson: Dr. Thomas E. Prisinzano Date approved: July 18, 2012 ii ABSTRACT Kappa opioid (KOP) receptors have been suggested as an alternative target to the mu opioid (MOP) receptor for the treatment of pain because KOP activation is associated with fewer negative side-effects (respiratory depression, constipation, tolerance, and dependence). The KOP receptor has also been implicated in several abuse-related effects in the central nervous system (CNS). KOP ligands have been investigated as pharmacotherapies for drug abuse; KOP agonists have been shown to modulate dopamine concentrations in the CNS as well as attenuate the self-administration of cocaine in a variety of species, and KOP antagonists have potential in the treatment of relapse. One drawback of current opioid ligand investigation is that many compounds are based on the morphine scaffold and thus have similar properties, both positive and negative, to the parent molecule. Thus there is increasing need to discover new chemical scaffolds with opioid receptor activity. -

TABLE 1 Studies of Antagonist Activity in Constitutively Active
TABLE 1 Studies of antagonist activity in constitutively active receptors systems shown to demonstrate inverse agonism for at least one ligand Targets are natural Gs and constitutively active mutants (CAM) of GPCRs. Of 380 antagonists, 85% of the ligands demonstrate inverse agonism. Receptor Neutral Antagonist Inverse Agonist Reference Human β2-adrenergic Dichloroisoproterenol, pindolol, labetolol, timolol, Chidiac et al., 1996; Azzi et alprenolol, propranolol, ICI 118,551, cyanopindolol al., 2001 Turkey erythrocyte β-adrenergic Propranolol, pindolol Gotze et al., 1994 Human β2-adrenergic (CAM) Propranolol Betaxolol, ICI 118,551, sotalol, timolol Samama et al., 1994; Stevens and Milligan, 1998 Human/guinea pig β1-adrenergic Atenolol, propranolol Mewes et al., 1993 Human β1-adrenergic Carvedilol CGP20712A, metoprolol, bisoprolol Engelhardt et al., 2001 Rat α2D-adrenergic Rauwolscine, yohimbine, WB 4101, idazoxan, Tian et al., 1994 phentolamine, Human α2A-adrenergic Napthazoline, Rauwolscine, idazoxan, altipamezole, levomedetomidine, Jansson et al., 1998; Pauwels MPV-2088 (–)RX811059, RX 831003 et al., 2002 Human α2C-adrenergic RX821002, yohimbine Cayla et al., 1999 Human α2D-adrenergic Prazosin McCune et al., 2000 Rat α2-adrenoceptor MK912 RX821002 Murrin et al., 2000 Porcine α2A adrenoceptor (CAM- Idazoxan Rauwolscine, yohimbine, RX821002, MK912, Wade et al., 2001 T373K) phentolamine Human α2A-adrenoceptor (CAM) Dexefaroxan, (+)RX811059, (–)RX811059, RS15385, yohimbine, Pauwels et al., 2000 atipamezole fluparoxan, WB 4101 Hamster α1B-adrenergic -

A,-, and P-Opioid Receptor Agonists on Excitatory Transmission in Lamina II Neurons of Adult Rat Spinal Cord
The Journal of Neuroscience, August 1994, 74(E): 4965-4971 Inhibitory Actions of S,-, a,-, and p-Opioid Receptor Agonists on Excitatory Transmission in Lamina II Neurons of Adult Rat Spinal Cord Steven R. Glaum,’ Richard J. Miller,’ and Donna L. Hammond* Departments of lPharmacoloaical and Phvsioloqical Sciences and ‘Anesthesia and Critical Care, The University of Chicago, Chicago, Illinois 60637 . This study examined the electrophysiological consequences tor in rat spinal cord and indicate that activation of either of selective activation of 6,-, 6,-, or r-opioid receptors using 6,- or Qopioid receptors inhibits excitatory, glutamatergic whole-cell recordings made from visually identified lamina afferent transmission in the spinal cord. This effect may me- II neurons in thin transverse slices of young adult rat lumbar diate the ability of 6, or 6, receptor agonists to produce an- spinal cord. Excitatory postsynaptic currents (EPSCs) or po- tinociception when administered intrathecally in the rat. tentials (EPSPs) were evoked electrically at the ipsilateral [Key words: DPDPE, deltorphin, spinal cord slice, EPSP, dorsal root entry zone after blocking inhibitory inputs with 6-opioid receptor, DAMGO, naltriben, 7-benzylidene- bicuculline and strychnine, and NMDA receptors with o-2- naltrexone (BNTX), naloxone] amino+phosphonopentanoic acid. Bath application of the p receptor agonist [D-Ala2, KMePhe4, Gly5-ollenkephalin (DAMGO) or the 6, receptor agonist [D-Pen2, o-PerF]en- The dorsal horn of the spinal cord is an important site for the kephalin (DPDPE) produced a log-linear, concentration-de- production of antinociception by K- and 6-opioid receptor ag- pendent reduction in the amplitude of the evoked EPSP/ onists (Yaksh, 1993). -

Zebrafish Behavioral Profiling Links Drugs to Biological Targets and Rest/Wake Regulation
www.sciencemag.org/cgi/content/full/327/5963/348/DC1 Supporting Online Material for Zebrafish Behavioral Profiling Links Drugs to Biological Targets and Rest/Wake Regulation Jason Rihel,* David A. Prober, Anthony Arvanites, Kelvin Lam, Steven Zimmerman, Sumin Jang, Stephen J. Haggarty, David Kokel, Lee L. Rubin, Randall T. Peterson, Alexander F. Schier* *To whom correspondence should be addressed. E-mail: [email protected] (A.F.S.); [email protected] (J.R.) Published 15 January 2010, Science 327, 348 (2010) DOI: 10.1126/science.1183090 This PDF file includes: Materials and Methods SOM Text Figs. S1 to S18 Table S1 References Supporting Online Material Table of Contents Materials and Methods, pages 2-4 Supplemental Text 1-7, pages 5-10 Text 1. Psychotropic Drug Discovery, page 5 Text 2. Dose, pages 5-6 Text 3. Therapeutic Classes of Drugs Induce Correlated Behaviors, page 6 Text 4. Polypharmacology, pages 6-7 Text 5. Pharmacological Conservation, pages 7-9 Text 6. Non-overlapping Regulation of Rest/Wake States, page 9 Text 7. High Throughput Behavioral Screening in Practice, page 10 Supplemental Figure Legends, pages 11-14 Figure S1. Expanded hierarchical clustering analysis, pages 15-18 Figure S2. Hierarchical and k-means clustering yield similar cluster architectures, page 19 Figure S3. Expanded k-means clustergram, pages 20-23 Figure S4. Behavioral fingerprints are stable across a range of doses, page 24 Figure S5. Compounds that share biological targets have highly correlated behavioral fingerprints, page 25 Figure S6. Examples of compounds that share biological targets and/or structural similarity that give similar behavioral profiles, page 26 Figure S7. -

In Vivoactivation of a Mutantμ-Opioid Receptor by Naltrexone Produces A
The Journal of Neuroscience, March 23, 2005 • 25(12):3229–3233 • 3229 Brief Communication In Vivo Activation of a Mutant -Opioid Receptor by Naltrexone Produces a Potent Analgesic Effect But No Tolerance: Role of -Receptor Activation and ␦-Receptor Blockade in Morphine Tolerance Sabita Roy, Xiaohong Guo, Jennifer Kelschenbach, Yuxiu Liu, and Horace H. Loh Department of Pharmacology, University of Minnesota, Minneapolis, Minnesota 55455 Opioid analgesics are the standard therapeutic agents for the treatment of pain, but their prolonged use is limited because of the development of tolerance and dependence. Recently, we reported the development of a -opioid receptor knock-in (KI) mouse in which the -opioid receptor was replaced by a mutant receptor (S196A) using a homologous recombination gene-targeting strategy. In these animals, the opioid antagonist naltrexone elicited antinociceptive effects similar to those of partial agonists acting in wild-type (WT) mice; however, development of tolerance and physical dependence were greatly reduced. In this study, we test the hypothesis that the failure of naltrexone to produce tolerance in these KI mice is attributable to its simultaneous inhibition of ␦-opioid receptors and activation of -opioid receptors. Simultaneous implantation of a morphine pellet and continuous infusion of the ␦-opioid receptor antagonist naltrindole prevented tolerance development to morphine in both WT and KI animals. Moreover, administration of SNC-80 [(ϩ)-4-[(␣R)-␣-((2S,5R)-4-allyl-2,5-dimethyl-1-piperazinyl)-3-methoxybenzyl]-N,N-diethylbenzamide], a ␦ agonist, in the naltrexone- pelleted KI animals resulted in a dose-dependent induction in tolerance development to both morphine- and naltrexone-induced anal- gesia. We conclude that although simultaneous activation of both - and ␦-opioid receptors results in tolerance development, -opioid receptor activation in conjunction with ␦-opioid receptor blockade significantly attenuates the development of tolerance. -

Neuroenhancement in Healthy Adults, Part I: Pharmaceutical
l Rese ca arc ni h li & C f B o i o l e Journal of a t h n Fond et al., J Clinic Res Bioeth 2015, 6:2 r i c u s o J DOI: 10.4172/2155-9627.1000213 ISSN: 2155-9627 Clinical Research & Bioethics Review Article Open Access Neuroenhancement in Healthy Adults, Part I: Pharmaceutical Cognitive Enhancement: A Systematic Review Fond G1,2*, Micoulaud-Franchi JA3, Macgregor A2, Richieri R3,4, Miot S5,6, Lopez R2, Abbar M7, Lancon C3 and Repantis D8 1Université Paris Est-Créteil, Psychiatry and Addiction Pole University Hospitals Henri Mondor, Inserm U955, Eq 15 Psychiatric Genetics, DHU Pe-psy, FondaMental Foundation, Scientific Cooperation Foundation Mental Health, National Network of Schizophrenia Expert Centers, F-94000, France 2Inserm 1061, University Psychiatry Service, University of Montpellier 1, CHU Montpellier F-34000, France 3POLE Academic Psychiatry, CHU Sainte-Marguerite, F-13274 Marseille, Cedex 09, France 4 Public Health Laboratory, Faculty of Medicine, EA 3279, F-13385 Marseille, Cedex 05, France 5Inserm U1061, Idiopathic Hypersomnia Narcolepsy National Reference Centre, Unit of sleep disorders, University of Montpellier 1, CHU Montpellier F-34000, Paris, France 6Inserm U952, CNRS UMR 7224, Pierre and Marie Curie University, F-75000, Paris, France 7CHU Carémeau, University of Nîmes, Nîmes, F-31000, France 8Department of Psychiatry, Charité-Universitätsmedizin Berlin, Campus Benjamin Franklin, Eschenallee 3, 14050 Berlin, Germany *Corresponding author: Dr. Guillaume Fond, Pole de Psychiatrie, Hôpital A. Chenevier, 40 rue de Mesly, Créteil F-94010, France, Tel: (33)178682372; Fax: (33)178682381; E-mail: [email protected] Received date: January 06, 2015, Accepted date: February 23, 2015, Published date: February 28, 2015 Copyright: © 2015 Fond G, et al. -

Biased Signaling by Endogenous Opioid Peptides
Biased signaling by endogenous opioid peptides Ivone Gomesa, Salvador Sierrab,1, Lindsay Lueptowc,1, Achla Guptaa,1, Shawn Goutyd, Elyssa B. Margolise, Brian M. Coxd, and Lakshmi A. Devia,2 aDepartment of Pharmacological Sciences, Icahn School of Medicine at Mount Sinai, New York, NY 10029; bDepartment of Physiology & Biophysics, Virginia Commonwealth University, Richmond, VA 23298; cSemel Institute for Neuroscience and Human Behavior, University of California, Los Angeles, CA 90095; dDepartment of Pharmacology & Molecular Therapeutics, Uniformed Services University, Bethesda MD 20814; and eDepartment of Neurology, UCSF Weill Institute for Neurosciences, University of California, San Francisco, CA 94143 Edited by Susan G. Amara, National Institutes of Health, Bethesda, MD, and approved April 14, 2020 (received for review January 20, 2020) Opioids, such as morphine and fentanyl, are widely used for the possibility that endogenous opioid peptides could vary in this treatment of severe pain; however, prolonged treatment with manner as well (13). these drugs leads to the development of tolerance and can lead to For opioid receptors, studies showed that mice lacking opioid use disorder. The “Opioid Epidemic” has generated a drive β-arrestin2 exhibited enhanced and prolonged morphine-mediated for a deeper understanding of the fundamental signaling mecha- antinociception, and a reduction in side-effects, such as devel- nisms of opioid receptors. It is generally thought that the three opment of tolerance and acute constipation (15, 16). This led to types of opioid receptors (μ, δ, κ) are activated by endogenous studies examining whether μOR agonists exhibit biased signaling peptides derived from three different precursors: Proopiomelano- (17–20), and to the identification of agonists that preferentially cortin, proenkephalin, and prodynorphin. -
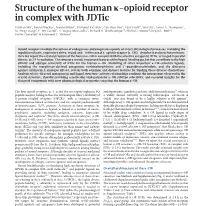
Structure of the Human Κ-Opioid Receptor in Complex with Jdtic
ARTICLE doi:10.1038/nature10939 Structure of the human k-opioid receptor in complex with JDTic Huixian Wu1, Daniel Wacker1, Mauro Mileni1, Vsevolod Katritch1, Gye Won Han1, Eyal Vardy2, Wei Liu1, Aaron A. Thompson1, Xi-Ping Huang2, F. Ivy Carroll3, S. Wayne Mascarella3, Richard B. Westkaemper4, Philip D. Mosier4, Bryan L. Roth2, Vadim Cherezov1 & Raymond C. Stevens1 Opioid receptors mediate the actions of endogenous and exogenous opioids on many physiological processes, including the regulation of pain, respiratory drive, mood, and—in the case of k-opioid receptor (k-OR)—dysphoria and psychotomimesis. Here we report the crystal structure of the human k-OR in complex with the selective antagonist JDTic, arranged in parallel dimers, at 2.9 A˚ resolution. The structure reveals important features of the ligand-binding pocket that contribute to the high affinity and subtype selectivity of JDTic for the human k-OR. Modelling of other important k-OR-selective ligands, including the morphinan-derived antagonists norbinaltorphimine and 59-guanidinonaltrindole, and the diterpene agonist salvinorin A analogue RB-64, reveals both common and distinct features for binding these diverse chemotypes. Analysis of site-directed mutagenesis and ligand structure–activity relationships confirms the interactions observed in the crystal structure, thereby providing a molecular explanation for k-OR subtype selectivity, and essential insights for the design of compounds with new pharmacological properties targeting the human k-OR. The four opioid receptors, m, d, k and the nociceptin/orphanin FQ antidepressants, anxiolytics and anti-addiction medications14, whereas peptide receptor, belong to the class A (rhodopsin-like) c subfamily of a widely abused, naturally occurring hallucinogen—salvinorin A G-protein-coupled receptors (GPCRs)1 with a common seven- (SalA)—was also found to be a highly selective k-OR agonist15. -
Pramipexole V2.1 Last Reviewed: 22/04/2021 Review Date: 22/04/2024
Pramipexole V2.1 Last reviewed: 22/04/2021 Review date: 22/04/2024 Pramipexole Traffic light classification- Amber 2 Information sheet for Primary Care Prescribers CLINICAL INFORMATION Key points/interactions Nausea is a common early side effect but usually responds to domperidone (10mg tds, or lowest effective dose – see MHRA advice) Ropinirole MR is first line dopamine agonist. Pramipexole MR should be reserved for patients in whom this is not suitable- see formulary. Dopamine agonists may cause compulsive/addictive behaviours such as gambling, compulsive shopping and hyper sexuality. Patients rarely recognise such changes as side effects and rarely report them unless specifically asked. Licensed Indications Treatment of idiopathic Parkinson's disease. Pramipexole may be used alone (without levodopa) or in combination with levodopa throughout the disease, through to late stages when the effect of levodopa wears off or becomes inconsistent and fluctuations of the therapeutic effect occur (end of dose or “on-off” fluctuations). Therapeutic Summary As per the licensed indication. NICE recommendations for the use of Pramipexole in Parkinson’s disease are: Consider a choice of dopamine agonists, levodopa or monoamine oxidase B (MAO-B) inhibitors for people in the early stages of Parkinson's disease whose motor symptoms do not impact their quality of life. Do not offer ergot-derived dopamine agonists as first-line treatment for Parkinson's disease. Offer a choice of dopamine agonists, MAO-B inhibitors or catechol-O-methyltransferase (COMT) -

The Effects of Morphine, Naloxone, and Оє Opioid Manipulation On
Neuroscience 287 (2015) 32–42 THE EFFECTS OF MORPHINE, NALOXONE, AND j OPIOID MANIPULATION ON ENDOCRINE FUNCTIONING AND SOCIAL BEHAVIOR IN MONOGAMOUS TITI MONKEYS (CALLICEBUS CUPREUS) B. J. RAGEN, a,b* N. MANINGER, b S. P. MENDOZA b AND Key words: titi monkey, mu opioid, pair-bonding, cortisol, K. L. BALES a,b monogamy, kappa opioid. a Psychology Department, University of California-Davis, One Shields Avenue, Davis, CA 95616, USA b California National Primate Research Center, One Shields INTRODUCTION Avenue, Davis, CA 95616, USA Socially monogamous species form long-term associations between two adults. In some species, Abstract—The l opioid receptor (MOR) and j opioid recep- these relationships have been shown to be classic tor (KOR) have been implicated in pair-bond formation and attachment bonds (Hazan and Shaver, 1987) and result maintenance in socially monogamous species. Utilizing in pair-mates spending considerable time in physical con- monogamous titi monkeys (Callicebus cupreus), the present tact with one another, providing social buffering, and study examined the potential role opioids play in modulat- exhibiting substantial behavioral and physiological agita- ing the response to separation, a potent challenge to the tion upon involuntary separation (Mason and Mendoza, pair-bond. In Experiment 1, paired male titi monkeys were separated from their pair-mate for 30-min and then received 1998). Due to the rarity of monogamy in mammals saline, naloxone (1.0 mg/kg), morphine (0.25 mg/kg), or the (Kleiman, 1977) there is a paucity of data on the neurobio- KOR agonist, U50,488 (0.01, 0.03, or 0.1 mg/kg) in a coun- logical underpinnings of adult attachment. -

1 TITLE PAGE Buprenorphine and Opioid Antagonism, Tolerance
JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 JPET FastThis Forward.article has not Published been copyedited on and November formatted. The 4, final 2010 version as DOI:10.1124/jpet.110.173823may differ from this version. JPET #173823 TITLE PAGE Buprenorphine and opioid antagonism, tolerance, and naltrexone-precipitated withdrawal Carol A. Paronis and Jack Bergman Downloaded from jpet.aspetjournals.org Preclinical Pharmacology Laboratory (C.A.P, J.B.) McLean Hospital/Harvard Medical School Belmont, MA at ASPET Journals on September 26, 2021 Department of Pharmaceutical Sciences (C.A.P.) Northeastern University Boston, MA 1 Copyright 2010 by the American Society for Pharmacology and Experimental Therapeutics. JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 This article has not been copyedited and formatted. The final version may differ from this version. JPET #173823 RUNNING TITLE PAGE Running Title: Buprenorphine antagonism, tolerance, and dependence Corresponding author: Carol A. Paronis, PhD Department of Pharmaceutical Sciences Northeastern University Downloaded from 211 Mugar Life Sciences Building Boston, MA 02115 jpet.aspetjournals.org Tel. (617) 373-3212 Fax. (617) 373-8886 Email: [email protected] at ASPET Journals on September 26, 2021 Number of: Pages - 20 Tables - 3 Figures - 5 References - 38 Number of words in: Abstract - 284 Introduction - 683 Discussion - 1258 2 JPET Fast Forward. Published on November 4, 2010 as DOI: 10.1124/jpet.110.173823 This article has not been copyedited and formatted. The final version may differ from this version. JPET #173823 ABSTRACT The dual antagonist effects of the mixed-action μ-opioid partial agonist/κ-opioid antagonist buprenorphine have not been previously compared in behavioral studies, and it is unknown whether they are comparably modified by chronic exposure.