MAPT) and FTDP-17 (PGRN
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2020 Question Book
2020 QUESTION BOOK 13TH EDITION WHO WE ARE Welcome to the thirteenth edition of the Ninja’s Guide to PRITE! Loma Linda University Medical Center is located in sunny Southern California. about 60 miles east of Los Angeles. A part of the Adventist Health System, we provide patient care in one of the largest non-profit health systems in the nation. Loma Linda's mission is to excel in medical education, global healthcare, and community outreach, all under a central tenant: "To Make Man Whole." At the Loma Linda Department of Psychiatry, our residents are trained in many diverse patient care settings. As an official World Health Organization Collaboration Center, our department funds resident electives in Global Mental Health at locations around the world. Additionally, our residents can participate in national and international disaster relief on the LLU Behavioral Health Trauma Team. We were proud to welcome our first group of Child and Adolescent Psychiatry fellows in the Summer of 2019 and work collaboratively with 3 other residency programs within the region. Our residency didactic education is constantly evolving based upon resident feedback, and our residents have the opportunity to aid in course development. More than anything, our residency fosters an environment where residents and faculty treat each other like family. Our faculty are dedicated to resident education and professional development. We believe in "taking 'No' off the table", encouraging innovative change, and passionately supporting our residents to achieve anything they set their minds to. For over a decade our residents have volunteered their time to create The Ninja's Guide to PRITE at our Annual Ninja PRITE Workshop. -

Theory of Mind Deficit in the Behavioral Variant of Frontotemporal Dementia and in Amyotrophic Lateral Sclerosis: Why Does It Matter?
Open Access Journal of Neurology & Neurosurgery Editorial Open Access J Neurol Neurosurg Volume 1 Issue 1 - December 2015 Copyright © All rights are reserved by Marco Cavallo Theory of Mind deficit in the behavioral variant of frontotemporal dementia and in amyotrophic lateral sclerosis: Why does it matter? Marco Cavallo1,2* 1eCampus University, Novedrate (Como), Italy 2Mental Health Department - Azienda Sanitaria Locale Torino 3, Italy Submission: November 15, 2015; Published: December 02, 2015 *Corresponding author: Marco Cavallo, Neuropsychologist, Researcher at the faculty of Psychology of the eCampus University of Novedrate, Italy, Tel no: +39.3478306430; Email: Editorial stories that explicitly referred to social situations. Our results underlined the needs for further research to gain a deeper Theory of Mind (hereinafter referred to as ToM) is the ability understanding on the possible link between patient’s behavioral to explain and predict other people’s behavior by attributing problems and their limited understanding of social situations. independent mental states to them. It allows us to recognize that mental states such as beliefs, intentions, and desires play a key role in driving and monitoring human behavior. Impairment in associated with ALS, a neurodegenerative disease that from We also aimed at clarifying the nature of the ToM deficits ToM ability can be highly disabling. ToM had been extensively cognitive and neuroimaging points of view appears to share studied in neuropsychiatric conditions such as autism and some relevant -

Pathologic Thr175 Tau Phosphorylation in CTE and CTE with ALS
Published Ahead of Print on January 3, 2018 as 10.1212/WNL.0000000000004899 ARTICLE OPEN ACCESS Pathologic Thr175 tau phosphorylation in CTE and CTE with ALS Alexander J. Moszczynski, PhD, Wendy Strong, BSc, Kathy Xu, MSc, Ann McKee, MD, Arthur Brown, PhD, Correspondence and Michael J. Strong, MD Dr. M.J. Strong [email protected] Neurology® 2018;90:e1-8. doi:10.1212/WNL.0000000000004899 Abstract Objective To investigate whether chronic traumatic encephalopathy (CTE) and CTE with amyotrophic lateral sclerosis (CTE-ALS) exhibit features previously observed in other tauopathies of pathologic phosphorylation of microtubule-associated protein tau at Thr175 (pThr175 tau) and Thr231 (pThr231 tau), and glycogen synthase kinase–3β (GSK3β) activation, and whether these pathologic features are a consequence of traumatic brain injury (TBI). Methods Tau isoform expression was assayed by western blot in 6 stage III CTE cases. We also used immunohistochemistry to analyze 5 cases each of CTE, CTE-ALS, and 5 controls for ex- pression of activated GSK3β, pThr175 tau, pThr231 tau, and oligomerized tau within spinal cord tissue and hippocampus. Using a rat model of moderate TBI, we assessed tau pathology and phospho-GSK3β expression at 3 months postinjury. Results CTE and CTE-ALS are characterized by the presence of all 6 tau isoforms in both soluble and insoluble tau isolates. Activated GSK3β, pThr175 tau, pThr231 tau, and oligomerized tau protein expression was observed in hippocampal neurons and spinal motor neurons. We observed tau neuronal pathology (fibrillar inclusions and axonal damage) and increased levels of pThr175 tau and activated GSK3β in moderate TBI rats. Conclusions Pathologic phosphorylation of tau at Thr175 and Thr231 and activation of GSK3β are features of the tauopathy of CTE and CTE-ALS. -

Social Behaviour Vs. Psychiatric Features Of
Psychiatria Danubina, 2010; Vol. 22, No. 2, pp 179–182 Case report © Medicinska naklada - Zagreb, Croatia SOCIAL BEHAVIOUR VS. PSYCHIATRIC FEATURES OF FRONTOTEMPORAL DEMENTIA Clinical report of two cases Rajka Marija Liščić1 & Aleš Kogoj2 1Institute for Medical Research and Occupational Health, Zagreb, Croatia 2Department of Geriatric Psychiatry, University Psychiatric Hospital, Ljubljana, Slovenia received: 6.10.2009; revised: 12.1.2010; accepted: 9.2.2010 SUMMARY Behavioural disturbances are prominent in frontotemporal dementia (FTD), a focal, non-Alzheimer type of dementia. Although most patients with FTD present with socially inappropriate behaviour, compulsive-like acts, poor insight and disinhibition, the presence of psychiatric features including delusions, hallucinations, and paranoia can lead to a misclassification of FTD as psychiatric disorder. In the absence of cognitive deficits non-experts fail to recognize these social changes as dementia symptoms. We report two individuals who met current clinical criteria for behavioural or frontal variant FTD (bv-FTD), with the aim of distinguishing between psychotic symptoms and the often bizarre personality and behaviour change found in FTD. Also we review the literature on the noncognitive neuropsyhiatric manifestation of this disorder. Clinical findings presented, and a literature review, indicate that psychotic symptoms are rare in FTD. Better awareness of behavioural symptoms in clinical practice is necessary in order to avoid misdiagnosis of FTD as psychiatric disorder. Key words: bv-frontotemporal dementia - behavioural disturbances - psychotic symptoms * * * * * INTRODUCTION and paranoia) must be distinguished from the often bizarre personality and behaviour changes of FTD. The With baby boomers now reaching late middle age, overlap between FTD and psychotic symptoms exists degenerative diseases are becoming an increasingly and therefore may lead to misleading diagnoses. -

Immune Effector Mechanisms and Designer Vaccines Stewart Sell Wadsworth Center, New York State Department of Health, Empire State Plaza, Albany, NY, USA
EXPERT REVIEW OF VACCINES https://doi.org/10.1080/14760584.2019.1674144 REVIEW How vaccines work: immune effector mechanisms and designer vaccines Stewart Sell Wadsworth Center, New York State Department of Health, Empire State Plaza, Albany, NY, USA ABSTRACT ARTICLE HISTORY Introduction: Three major advances have led to increase in length and quality of human life: Received 6 June 2019 increased food production, improved sanitation and induction of specific adaptive immune Accepted 25 September 2019 responses to infectious agents (vaccination). Which has had the most impact is subject to debate. KEYWORDS The number and variety of infections agents and the mechanisms that they have evolved to allow Vaccines; immune effector them to colonize humans remained mysterious and confusing until the last 50 years. Since then mechanisms; toxin science has developed complex and largely successful ways to immunize against many of these neutralization; receptor infections. blockade; anaphylactic Areas covered: Six specific immune defense mechanisms have been identified. neutralization, cytolytic, reactions; antibody- immune complex, anaphylactic, T-cytotoxicity, and delayed hypersensitivity. The role of each of these mediated cytolysis; immune immune effector mechanisms in immune responses induced by vaccination against specific infectious complex reactions; T-cell- mediated cytotoxicity; agents is the subject of this review. delayed hypersensitivity Expertopinion: In the past development of specific vaccines for infections agents was largely by trial and error. With an understanding of the natural history of an infection and the effective immune response to it, one can select the method of vaccination that will elicit the appropriate immune effector mechanisms (designer vaccines). These may act to prevent infection (prevention) or eliminate an established on ongoing infection (therapeutic). -

Investigation of Anti-Iglon5-Induced Neurodegenerative Changes in Human Neurons
bioRxiv preprint doi: https://doi.org/10.1101/2020.08.27.269795; this version posted August 28, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Manuscript BioRxiv Investigation of anti-IgLON5-induced neurodegenerative changes in human neurons Mattias Gamre1,2, Matias Ryding1,2, Mette Scheller Nissen1,2,3, Anna Christine Nilsson4, Morten Meyer1,2,5, Morten Blaabjerg1,2,3,5 1Neurobiological Research, Institute of Molecular Medicine, University of Southern Denmark, Odense, Denmark. 2Department of Neurology, Odense University Hospital, Odense, Odense, Denmark 3Department of Clinical Research, Odense University Hospital, Odense, Denmark 4Department of Clinical Immunology, Odense University Hospital, Odense, Denmark 5BRIDGE – Brain Research Inter-Disciplinary Guided Excellence, Department of Clinical Research, University of Southern Denmark, Odense, Denmark Number of pages: 12 Number of figures: 4 Keywords: IgLON5, Autoimmune encephalitis, neurodegeneration, inflammation, Tau Corresponding author Professor Morten Blaabjerg, MD, PhD Department of Neurology Odense University Hospital J.B. Winsløws Vej 4 5000 Odense C Denmark Phone: (+45) 6541 2457 E-mail: [email protected] Page 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.08.27.269795; this version posted August 28, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. -

Psychotic Symptoms in Frontotemporal Dementia: a Diagnostic Dilemma?
International Psychogeriatrics (2015), 27:4, 531–539 C International Psychogeriatric Association 2014. This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/3.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited. doi:10.1017/S1041610214002580 Psychotic symptoms in frontotemporal dementia: a diagnostic dilemma? ........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................... Maria Landqvist Waldö,1 Lars Gustafson,1 Ulla Passant1 and Elisabet Englund2 1Section of Geriatric Psychiatry, Department of Clinical Sciences, Lund University, Klinikgatan 22, Lund SE-221 85, Sweden 2Section of Oncology and Pathology, Department of Clinical Sciences, Lund University, Lund, SE-221 85, Sweden ABSTRACT Background: Frontotemporal dementia (FTD) constitutes a spectrum of neurodegenerative disorders associated with degeneration of, predominantly, -

Schizophrenia and Frontotemporal Dementia: Shared Causation?
International Review of Psychiatry, April 2013; 25(2): 168–177 Schizophrenia and frontotemporal dementia: Shared causation? MICHA Ł HARCIAREK 1 , DOLORES MALASPINA2 , TAO SUN3 & ELKHONON GOLDBERG4 1 Division of Clinical Psychology and Neuropsychology, Institute of Psychology, University of Gdansk, Poland, 2 Department of Psychiatry, New York University School of Medicine, New York, USA, 3 Department of Cell and Developmental Biology, Cornell University Weill Medical College, New York, USA, 4 Department of Neurology, New York University School of Medicine, New York, USA Abstract The relationship between specifi c genes and particular diseases in neuropsychiatry is unclear, and newer studies focus on shared domains of neurobiological and cognitive pathology across different disorders. This paper reviews the evidence for an association between schizophrenia and frontotemporal dementia, including symptom similarity, familial co-morbidity, and neuroanatomical changes. Genetic as well as epigenetic fi ndings from both schizophrenia and frontotemporal demen- tia are also discussed. As a result, we introduce the hypothesis of a shared susceptibility for certain subgroups of schizo- phrenia and frontotemporal dementia. This common causation may involve the same gene(s) at different stages of life: early in schizophrenia and late in frontotemporal dementia. Additionally, we provide a rationale for future research that should emphasize both genetic and cognitive parallels between certain forms of schizophrenia and frontotemporal dementia in a synergistic, coordinated way, placing both in the context of aberrant lateralization patterns. Introduction of what constitutes a ‘ disorder ’ in neuropsychiatry, The relationship between specifi c genes and particu- and invited the revision of, and departure from, tra- lar diseases in neuropsychiatry remains unclear, and ditional diagnostic taxonomies. -

Differentiating Delirium, Dementia, and Depression Elderly Patients Are at High Risk of Mood and Cognitive Impairments Such As Depression, Delirium and Dementia
February 2021 www.nursingcenter.com Differentiating Delirium, Dementia, and Depression Elderly patients are at high risk of mood and cognitive impairments such as depression, delirium and dementia. Delirium is an acute, transient and reversible cause of brain dysfunction, usually triggered by one or more precipitating factors, including infection, medications, pain and dehydration. Dementia is usually subtle in its onset and may not be recognized until it has affected one or more cognitive domains. Depression is characterized by low mood, loss of interest or pleasure in most activities, sleep disturbance, anxiety, and social withdrawal. Delirium, dementia, and depression have overlapping characteristics, and patients may experience more than one of these conditions at the same time. It is essential to differentiate between these conditions, particularly if delirium is present, because this is an acute medical emergency that requires rapid assessment and management. Nurses in both outpatient and hospital settings can have a significant role in the identification, assessment and management of patients with dementia, delirium and depression. Dementia Signs and Symptoms Dementia is the most common disorder of cognition, and is characterized by a decline in one or more of these cognitive domains (Larson, 2019): • Memory (remote memories versus recent memories) • Language (word retrieval, comprehension) • Learning new skills (following linear instructions, with ability to repeat skills) • Executive function (ability to shop, do laundry, write a check) • Complex attention (completing multi-step tasks) • Social cognition (remembering family connections, names) • Perceptual-motor skills (dressing, bathing) The decline in function must not be attributable to other organic disease, must not be due to an episode of delirium, and must be severe enough to interfere with independence or daily functioning. -

An Autopsy Case of Progressive Supranuclear Palsy with Incidental
Letters Discussion | This pilot study successfully explored the effect size 3. Korte J-M, Kaila T, Saari KM. Systemic bioavailability and cardiopulmonary of timolol eyedrops on migraine headaches. Several partici- effects of 0.5% timolol eyedrops. Graefes Arch Clin Exp Ophthalmol. 2002;240 (6):430-435. pants responded extremely well to the timolol. Further re- 4. Migliazzo CV, Hagan JC III. Beta blocker eyedrops for treatment of acute search is needed to determine what patient factors might pre- migraine. Mo Med. 2014;111(4):283-288. dict responsiveness to timolol. 5. Chiam PJT. Topical beta-blocker treatment for migraine. Int Ophthalmol. 2012; 32(1):85-88. Limitations. Study limitations include a small sample size, a 6. Headache Classification Committee of the International Headache Society. lack of investigator masking, and an imperfect placebo, as The international classification of headache disorders, 3rd edition (beta artificial tears tend to cause less of a burning sensation than version). https://www.ichd-3.org/wp-content/uploads/2016/08/International -Headache-Classification-III-ICHD-III-2013-Beta-1.pdf. Accessed June 1, 2016. timolol. With a half-life of 4 hours, timolol ophthalmic is unlikely to have had an association with repeated head- aches or beyond the 3-day washout period. Four 50-μL drops of timolol, 0.5%, represent 1 mg of timolol, which An Autopsy Case of Progressive Supranuclear compares with an oral prophylactic dosage of 10 to 30 mg of Palsy With Incidental ATXN2 Expansion timolol daily. Future research should aim for a target enroll- A case of multiple system atrophy with predominant parkin- ment of more than 86 participants and explore optimal dos- sonism (MSA-P) with ATXN2 (OMIM 601517) expansion was ing regimens. -
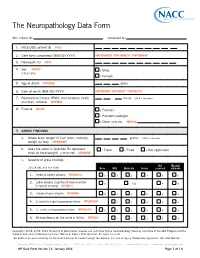
The Neuropathology Data Form
The Neuropathology Data Form ADC subject ID: Completed by: 1. MDS/UDS patient ID PTID 2. Date form completed (MM/DD/ YYYY) NPFORMMO / NPFORMDY / NPFORMYR 3. Neuropath ID NPID 4. Sex NPSEX 1 Male (CHECK ONE) 2 Female 5. Age at death NPDAGE years 6. Date of death (MM/ DD/ YYYY) NPDODMO / NPDODDY / NPDODYR 7. Postmortem interval (PMI): time between death . hours (99.9 = unknown) and brain removal NPPMIH 8. Fixative NPFIX 1 Formalin 2 Paraformaldehyde 7 Other (SPECIFY): NPFIXX 9. GROSS FINDINGS a. Whole brain weight (if half brain, multiply grams (9999 = unknown) weight by two) NPWBRWT b. Does the value in Question 9a represent 1 Fresh 2 Fixed 8 Not applicable fresh or fixed weight? (CHECK ONE) NPWBRF c. Severity of gross findings Not Missing/ (CHECK ONE BOX PER ROW) None Mild Moderate Severe assessed unknown 1. Cerebral cortex atrophy NPGRCCA 0 1 2 3 8 9 Lobar atrophy (significant frontal and/or 2. 0 1 Yes 8 9 temporal atrophy) NPGRLA 3. Hippocampus atrophy NPGRHA 0 1 2 3 8 9 4. Substantia nigra hypopigmentation NPGRSNH 1 2 3 8 9 5. L. ceruleus hypopigmentation NPGRLCH 0 1 2 3 8 9 6. Atherosclerosis (of the circle of Willis) NPAVAS 1 2 3 8 9 Copyright© 2006, 2008, 2014 University of Washington. Created and published by the Neuropathology Steering ommittee of the ADC Program and the National Alzheimer’s Coordinating Center (Walter A. Kukull, PhD, Director). All rights reserved. This publication was funded by the National Institutes of Health through the National Institute on Aging (Cooperative Agreement U01 AG016976). -

Qt8nt665v8.Pdf
UC Berkeley Berkeley Scientific Journal Title Acquired Savantism: The Genesis of Accidental Genius Permalink https://escholarship.org/uc/item/8nt665v8 Journal Berkeley Scientific Journal, 14(2) ISSN 1097-0967 Author Gururangan, Kapil Publication Date 2011 DOI 10.5070/BS3142011708 Undergraduate eScholarship.org Powered by the California Digital Library University of California ACQUIRED SAVANTISM: THE GENESIS OF ACCIDENTAL GENIUS Kapil Gururangan The autistic model for savantism stems from At age ten, Orlando Serrell was struck on the the high incidence of autism in the savant population. left side of his head with a baseball; he is able to clearly Nearly half of all savants display some condition that remember the weather and details about his personal can be classified as an autism spectrum disorder, leading activities for every day since that accident (Hughes 2010, scientists to presume that some facet of autism may 149). Some elderly patients battling the debilitation of also predispose the human mind to the formation of dementia have discovered newfound abilities in music, these amazing abilities (Treffert 2009, 2). This model is art, and language (Miller 2008, 8). A former molecular based on the principle of weak central coherence theory, biologist loses her ability to speak but becomes amazingly talented in painting that fuses music, vision, and feeling onto a canvas titled Unraveling Bolero (8). These examples all have one thing in common: the individuals acquire BSJ impressive abilities following damage to the central nervous system, predominantly in the left hemisphere of the brain. Savant syndrome is the presence of extreme talent in the wake of profound disabilities and while this normally presents in early development, scientists have observed a fascinating mechanism for the occurrence of savant syndrome after an accident (Hughes 2010, 149).