A Large Mutational Study in Pachyonychia Congenita Neil J
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PGD: a Celebration of 20 Years
PGD: A Celebration of 20 years: What is Reality and What is Not? Roma June 30, 2010 Mark Hughes, M.D., Ph.D . Professor of Genetics, Internal Medicine, Pathology Director, Genesis Genetics Institute Director, State of Michigan Genomic Technology Center Reality – (Three obvious ones) PGD • Has led to the birth of thousands of healthy children to very desperate, genetically at-risk couples. • Remains at the very limit of medical diagnostic testing • The technology continues to improve - – but it is not reality to think PGD will ever have a 0% false positive or false negative rate Reality: We still do not know What is best to biopsy, and when? Polar Body Blastomere Trophoectoderm Variation in Biopsy Skill Clinic Biopsies +HCG / ET 1 314 17% 2 427 26% 3 181 12% 4 712 31% Reality: We all are controversial • PGD has raised international controversy – How is it bioethically different from Prenatal Testing? – Who should control the use of these technologies? – Should there be government PGD testing standards? • What is the difference between a Disease and a Trait - and who decides? PGD Disorders (A, B, C) • ACHONDROPLASIA (FGFR) • BARTH DILIATED CARDIOMYOPATHY • ACTIN-NEMALIN MYOPATHY (ACTA) • BETA THALASSEMIA (HBB) • ADRENOLEUKODYSTROPHY (ABCD) • BLOOM SYNDROME • AGAMMAGLOBULINEMIA-BRUTON (TYKNS) • BREAST CANCER (BRCA1 & 2) • ALAGILLE SYNDROME (JAG) • CACH-ATAXIA (EIFB) • ALDOLASE A, FRUCTOSE-BISPHOSPHATE • CADASIL (NOTCH) • ALPHA THALASSEMIA (HBA) • CANAVAN DISEASE (ASPA) • ALPHA-ANTITRYPSIN (AAT) • CARNITINE-ACYLCARN TRANSLOCASE • ALPORT SYNDROME -
Associated Palmoplantar Keratoderma
DR ABIGAIL ZIEMAN (Orcid ID : 0000-0001-8236-207X) Article type : Review Article Pathophysiology of pachyonychia congenita-associated palmoplantar keratoderma: New insight into skin epithelial homeostasis and avenues for treatment Authors: A. G. Zieman1 and P. A. Coulombe1,2 # Affiliations: 1Department of Cell and Developmental Biology, University of Michigan Medical School, Ann Arbor, MI 48109, USA; 2Department of Dermatology, University of Michigan Medical School, Ann Arbor, MI 48109, USA #Corresponding author: Pierre A. Coulombe, PhD, 3071 Biomedical Sciences Research Building, 109 Zina Pitcher Place, Ann Arbor, MI 48109, USA. Tel: 734-615-7509. Email: [email protected]. Funding Sources: These studies were supported by grant AR044232 issued to P.A.C. from the National Institute of Arthritis, Musculoskeletal and Skin Disease (NIAMS). A.G.Z. received support from grant T32 CA009110 from the National Cancer Institute. Author Manuscript This is the author manuscript accepted for publication and has undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/BJD.18033 This article is protected by copyright. All rights reserved Conflict of interest disclosures: None declared. Bulleted statements: What’s already known about this topic? Pachyonychia congenita is a rare genodermatosis caused by mutations in KRT6A, KRT6B, KRT6C, KRT16, KRT17, which are normally expressed in skin appendages and induced following injury. Individuals with PC present with multiple clinical symptoms that usually include thickened and dystrophic nails, palmoplantar keratoderma (PPK), glandular cysts, and oral leukokeratosis. -

WES Gene Package Multiple Congenital Anomalie.Xlsx
Whole Exome Sequencing Gene package Multiple congenital anomalie, version 5, 1‐2‐2018 Technical information DNA was enriched using Agilent SureSelect Clinical Research Exome V2 capture and paired‐end sequenced on the Illumina platform (outsourced). The aim is to obtain 8.1 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA‐MEM algorithm (reference: http://bio‐bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x A4GALT [Blood group, P1Pk system, P(2) phenotype], 111400 607922 101 100 100 99 [Blood group, P1Pk system, p phenotype], 111400 NOR polyagglutination syndrome, 111400 AAAS Achalasia‐addisonianism‐alacrimia syndrome, 231550 605378 73 100 100 100 AAGAB Keratoderma, palmoplantar, -

1 Introduction 1
1 Introduction 1 Part I The Mechanisms of Cutaneous Mosaicism 2 Mosaicism as a Biological Concept 5 2.1 Historical Beginnings 5 2.2 Mosaicism in Plants 6 2.3 Mosaicism in Animals 7 2.4 Mosaicism in Human Skin 9 2.5 Mosaicism Versus Chimerism 10 References 11 3 Two Major Categories of Mosaicism 13 3.1 Genomic Mosaicism 13 3.1.1 Genomic Mosaicism of Autosomes 13 3.1.2 Genomic X-Chromosome Mosaicism in Male Patients 24 3.1.3 Superimposed Segmental Manifestation of Polygenic Skin Disorders 24 3.2 Epigenetic Mosaicism 26 3.2.1 Epigenetic Mosaicism of Autosomal Genes 26 3.2.2 Epigenetic Mosaicism of X Chromosomes 27 References 31 4 Relationship Between Hypomorphic Alleles and Mosaicism of Lethal Mutations 39 References 41 Part II The Patterns of Cutaneous Mosaicism 5 Six Archetypical Patterns 45 5.1 Lines of Blaschko 45 5.1.1 Lines of Blaschko, Narrow Bands 52 5.1.2 Lines of Blaschko, Broad Bands 52 5.1.3 Analogy of Blaschko's Lines in Other Organs. ... 53 5.1.4 Blaschko's Lines in Animals 54 5.1.5 Analogy of Blaschko's Lines in the Murine Brain. 54 http://d-nb.info/1034513591 X 5.2 Checkerboard Pattern 56 5.3 Phylloid Pattern 57 5.4 Large Patches Without Midline Separation 57 5.5 Lateralization Pattern 57 5.6 Sash-Like Pattern 58 References 59 6 Less Well Defined or So Far Unclassifiable Patterns 63 6.1 The Pallister-Killian Pattern 63 6.2 The Mesotropic Facial Pattern 64 References 65 Part III Mosaic Skin Disorders 7 Nevi 69 7.1 The Theory of Lethal Genes Surviving by Mosaicism 70 7.2 Pigmentary Nevi 70 7.2.1 Melanocytic Nevi 70 7.2.2 Other Nevi Reflecting Pigmentary Mosaicism. -

Hereditary Palmoplantar Keratoderma "Clinical and Genetic Differential Diagnosis"
doi: 10.1111/1346-8138.13219 Journal of Dermatology 2016; 43: 264–274 REVIEW ARTICLE Hereditary palmoplantar keratoderma “clinical and genetic differential diagnosis” Tomo SAKIYAMA, Akiharu KUBO Department of Dermatology, Keio University School of Medicine, Tokyo, Japan ABSTRACT Hereditary palmoplantar keratoderma (PPK) is a heterogeneous group of disorders characterized by hyperkerato- sis of the palm and the sole skin. Hereditary PPK are divided into four groups – diffuse, focal, striate and punctate PPK – according to the clinical patterns of the hyperkeratotic lesions. Each group includes simple PPK, without associated features, and PPK with associated features, such as involvement of nails, teeth and other organs. PPK have been classified by a clinically based descriptive system. In recent years, many causative genes of PPK have been identified, which has confirmed and/or rearranged the traditional classifications. It is now important to diag- nose PPK by a combination of the traditional morphological classification and genetic testing. In this review, we focus on PPK without associated features and introduce their morphological features, genetic backgrounds and new findings from the last decade. Key words: diffuse, focal, punctate, striate, transgrediens. INTRODUCTION psoriasis vulgaris confined to the palmoplantar area (Fig. 1b) are comparatively common and are sometimes difficult to Palmoplantar keratoderma (PPK) is a heritable or acquired dis- distinguish from hereditary PPK. A skin biopsy is essential in order characterized by abnormal hyperkeratotic thickening of diagnosing these cases. Lack of a family history is not neces- the palm and sole skin. In a narrow sense, PPK implies heredi- sarily evidence of an acquired PPK, because autosomal reces- tary PPK, the phenotype of which usually appears at an early sive PPK can appear sporadically from parent carriers and age. -

Ectodermal Dysplasia (Generic Term)
Ectodermal Dysplasia (generic term) Authors: Doctor Kathleen Mortier1, Professor Georges Wackens1 Creation date: September 2004 Scientific Editor: Professor Antonella Tosti 1Department of stomatology and maxillofacial surgery, AZ VUB Brussels, Belgium [email protected] Definition Clinical classification of Ectodermal dysplasias References Definition Ectodermal dysplasias (EDs) are a heterogeneous group of disorders characterized by developmental dystrophies of ectodermal structures, such as hypohidrosis, hypotrichosis, onychodysplasia and hypodontia or anodontia. About 160 clinically and genetically distinct hereditery ectodermal dysplasias have been cataloged. In the early seventies there existed no definition and no classification. Freire-Maia and Pinheiro tried to put some order in the field of ectodermal dysplasias. Firstly, the group should be defined before an attempt was made to list its conditions. Secondly, the group was so large that it was necessary to split it into several subgroups. So they decided that an ED should present any two of the signs that affected the four structures widely mentioned by the authors who studied the classic EDs – hair, teeth, nails and sweat glands – with or without any other sign (see blow). The system is arbitrary without biological relevance to the pathogenesis and genetics of the specific disorder. However, classification based on clinical signs and symptoms is all that has been available until recently, since the pathogenesis and molecular genetics of the disorder are largely unknown. Clinical classification of Ectodermal dysplasias (Pinheiro and Freire-Maia, 1994) Unknown cause Conditions AD AR XL ? AD? AR? XL? Subgroup 1-2-3-4 1. Christ-Siemens-Touraine (CST) syndrome (MIM 305100; XR BDE 0333; POS 3208; FMP 1) 2. -

Nova Scotia Atlee Perinatal Database Coding Manual 15 Edition (Version
Nova Scotia Atlee Perinatal Database Coding Manual 15th Edition (Version 15.0.0) April 2011 TABLE OF CONTENTS LISTINGS OF HOSPITALS 11 ADMISSION INFORMATION 16 DELIVERED ADMISSION 26 Routine Information – Delivered Admission 26 Routine Information – Labour 57 Routine Information – Infant 77 UNDELIVERED ADMISSION 94 Routine information – undelivered 94 POSTPARTUM ADMISSIONS 104 Routine Information – Postpartum Admission 104 NEONATAL ADMISSIONS 112 Routine Information – Neonatal Admissions 112 ADULT RCP CODES 124 INFANT RCP CODES 143 INDEX OF MATERNAL DISEASES AND PROCEDURES 179 INDEX OF NEONATAL DISEASES AND PROCEDURES 195 1 INDEX FOR ADMISSION INFORMATION Admission date .............................................................................................................................. 17 Admission time .............................................................................................................................. 17 Admission process status ............................................................................................................... 25 Admission type .............................................................................................................................. 17 A/S/D number ................................................................................................................................ 18 Birth date ....................................................................................................................................... 18 Care provider attending ................................................................................................................ -

Table I. Genodermatoses with Known Gene Defects 92 Pulkkinen
92 Pulkkinen, Ringpfeil, and Uitto JAM ACAD DERMATOL JULY 2002 Table I. Genodermatoses with known gene defects Reference Disease Mutated gene* Affected protein/function No.† Epidermal fragility disorders DEB COL7A1 Type VII collagen 6 Junctional EB LAMA3, LAMB3, ␣3, 3, and ␥2 chains of laminin 5, 6 LAMC2, COL17A1 type XVII collagen EB with pyloric atresia ITGA6, ITGB4 ␣64 Integrin 6 EB with muscular dystrophy PLEC1 Plectin 6 EB simplex KRT5, KRT14 Keratins 5 and 14 46 Ectodermal dysplasia with skin fragility PKP1 Plakophilin 1 47 Hailey-Hailey disease ATP2C1 ATP-dependent calcium transporter 13 Keratinization disorders Epidermolytic hyperkeratosis KRT1, KRT10 Keratins 1 and 10 46 Ichthyosis hystrix KRT1 Keratin 1 48 Epidermolytic PPK KRT9 Keratin 9 46 Nonepidermolytic PPK KRT1, KRT16 Keratins 1 and 16 46 Ichthyosis bullosa of Siemens KRT2e Keratin 2e 46 Pachyonychia congenita, types 1 and 2 KRT6a, KRT6b, KRT16, Keratins 6a, 6b, 16, and 17 46 KRT17 White sponge naevus KRT4, KRT13 Keratins 4 and 13 46 X-linked recessive ichthyosis STS Steroid sulfatase 49 Lamellar ichthyosis TGM1 Transglutaminase 1 50 Mutilating keratoderma with ichthyosis LOR Loricrin 10 Vohwinkel’s syndrome GJB2 Connexin 26 12 PPK with deafness GJB2 Connexin 26 12 Erythrokeratodermia variabilis GJB3, GJB4 Connexins 31 and 30.3 12 Darier disease ATP2A2 ATP-dependent calcium 14 transporter Striate PPK DSP, DSG1 Desmoplakin, desmoglein 1 51, 52 Conradi-Hu¨nermann-Happle syndrome EBP Delta 8-delta 7 sterol isomerase 53 (emopamil binding protein) Mal de Meleda ARS SLURP-1 -

Atlas of DISEASES of the NAIL
An Atlas of DISEASES OF THE NAIL THE ENCYCLOPEDIA OF VISUAL MEDICINE SERIES An Atlas of DISEASES OF THE NAIL Phoebe Rich, MD Oregon Health Sciences University Portland, Oregon, USA Richard K.Scher, MD College of Physicians and Surgeons Columbia University, New York, USA The Parthenon Publishing Group International Publishers in Medicine, Science & Technology A CRC PRESS COMPANY BOCA RATON LONDON NEW YORK WASHINGTON, D.C. Published in the USA by The Parthenon Publishing Group Inc. 345 Park Avenue South, 10th Floor New York NY 10010 USA This edition published in the Taylor & Francis e-Library, 2005. To purchase your own copy of this or any of Taylor & Francis or Routledge’s collection of thousands of eBooks please go to www.eBookstore.tandf.co.uk. Published in the UK and Europe by The Parthenon Publishing Group 23–25 Blades Court Deodar Road London SW15 2NU UK Copyright © 2003 The Parthenon Publishing Group Library of Congress Cataloging-in-Publication Data Rich, Phoebe An atlas of diseases of the nail/Phoebe Rich, R.K.Scher p.; cm.—(The encyclopedia of visual medicine series) Includes bibliographical references and index. ISBN 1-85070-595-X 1. Nails (Anatomy)—Diseases—Atlases. I. Title: Diseases of the nail. II. Rich, Phoebe III. Title. IV. Series. [DNLM: 1. Nail Diseases—diagnosis—Atlases. 2. Nail Diseases—therapy—Atlases. WR 17 S326a 2002] RL165.S35 2002 616.5′47—dc21 2002025346 British Library Cataloguing in Publication Data Rich, Phoebe— An atlas of diseases of the nail 1. Nails (Anatomy)—Diseases I. Title II. Scher, Richard K., 1929– 616.5′47 ISBN 0-203-49069-X Master e-book ISBN ISBN 0-203-59671-4 (Adobe eReader Format) ISBN 1-85070-595-X (Print Edition) First published in 2003 This edition published in the Taylor & Francis e-Library, 2005. -

NGS Oncology)
UNIVERSITY OF MINNESOTA PHYSICIANS OUTREACH LABS Submit this form along with the appropriate Molecular requisition (Molecular Diagnostics or MOLECULAR DIAGNOSTICS (612) 273-8445 DATE: TIME COLLECTED: PCU/CLINIC: Molecular NGS Oncology). AM PM PATIENT IDENTIFICATION DIAGNOSIS (Dx) / DIAGNOSIS CODES (ICD-9) - OUTPATIENTS ONLY SPECIMEN TYPE: o Blood (1) (2) (3) (4) PLEASE COLLECT 5-10CC IN ACD-A OR EDTA TUBE ORDERING PHYSICIAN NAME AND PHONE NUMBER: Tests can be ordered as a full panel, or by individual gene(s). Please contact the genetic counselor with any questions at 612-624-8948 or by pager at 612-899-3291. _______________________________________________ Test Ordered- EPIC: Next generation sequencing(Next Gen) Sunquest: NGS Ectodermal dysplasia epidermolysis bullosa simplex with Acne inversa muscular dystrophy Full panel PLEC Full panel EDA Epidermolytic hyperkeratosis NCSTN EDARADD Full panel PSENEN MSX1 KRT1 PSEN1 KRT85 KRT10 Acrodermatitis enteropathica PVRL4 Erythroderma, congenital, with NFKBIA palmoplantar keratoderma, SLC39A4 IKBKG hypotrichosis, and hyper IgE Amyloidosis, primary localized Ectodermal dysplasia/skin fragility DSG1 cutaneous, 1 syndrome Erythrokeratodermia variabilis with PKP1 erythema gyratum repens Full panel Ectrodactyly, ectodermal dysplasia, GJB4 OSMR and cleft lip/palate syndrome 3 Familial benign pemphigus IL31RA TP63 ATP2C1 Atrichia with papular lesions Focal facial dermal dysplasia 3 Focal dermal hypoplasia TWIST2 HR PORCN Epidermodysplasia verruciformis Autosomal recessive hypohidrotic Glomuvenous malformations -

Acro-Osteolysis: a Complication of Jadassohn–Lewandowsky Syndrome
15 March 2005 Use of Articles in the Pachyonychia Congenita Bibliography The articles in the PC Bibliography may be restricted by copyright laws. These have been made available to you by PC Project for the exclusive use in teaching, scholar- ship or research regarding Pachyonychia Congenita. To the best of our understanding, in supplying this material to you we have followed the guidelines of Sec 107 regarding fair use of copyright materials. That section reads as follows: Sec. 107. - Limitations on exclusive rights: Fair use Notwithstanding the provisions of sections 106 and 106A, the fair use of a copyrighted work, including such use by reproduction in copies or phonorecords or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use the factors to be considered shall include - (1) the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; (2) the nature of the copyrighted work; (3) the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and (4) the effect of the use upon the potential market for or value of the copyrighted work. The fact that a work is unpublished shall not itself bar a finding of fair use if such finding is made upon consideration of all the above factors. -
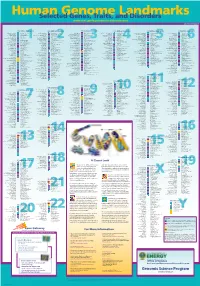
Genomeposter2009.Pdf
Fold HumanSelected Genome Genes, Traits, and Landmarks Disorders www.ornl.gov/hgmis/posters/chromosome genomics.energy.