Mental Health Branch Cultural Competence Plan June 2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Appendix A: Project Partners
Humboldt County Coastal Trail Implementation Strategy Technical Appendix JANUARY 2011 Prepared for: State of California Coastal Conservancy Project team: Natural Resources Services Division of Redwood Community Action Agency Alta Planning + Design Planwest Partners Streamline Planning Consultants Humboldt County Coastal Trail Implementation Strategy TECHNICAL APPENDICES Thank you to the community members and agency staff who provided input during public meetings and advisory team workshops throughout the planning process. Your participation and contributions are key to this and future efforts to bring the CCT to fruition. Peter Jarausch Project Manager State of California Coastal Conservancy [email protected] This plan was made possible through Proposition 40 funding Photo credits: Kids on bicycles, N. Wynne; Trail horses, U. Driscoll; Eureka boardwalk, J. Kalt All other photos by project team Appendix A: Project Partners Primary Partners ................................................................................................................................................................... 2 Federal Agencies .............................................................................................................................................................. 2 Bureau of Land Management (BLM) ....................................................................................................................... 2 U.S. Fish and Wildlife Service (USFWS) ................................................................................................................ -

Characterizing Tribal Cultural Landscapes, Volume II: Tribal Case
OCS Study BOEM 2017-001 Characterizing Tribal Cultural Landscapes Volume II: Tribal Case Studies US Department of the Interior Bureau of Ocean Energy Management Pacific OCS Region This page intentionally left blank. OCS Study BOEM 2017-001 Characterizing Tribal Cultural Landscapes Volume II: Tribal Case Studies David Ball Rosie Clayburn Roberta Cordero Briece Edwards Valerie Grussing Janine Ledford Robert McConnell Rebekah Monette Robert Steelquist Eirik Thorsgard Jon Townsend Prepared under BOEM-NOAA Interagency Agreement M12PG00035 by National Oceanic and Atmospheric Administration Office of National Marine Sanctuaries 1305 East-West Highway, SSMC4 Silver Spring, MD 20910 Makah Tribe Confederated Tribes of Grand Ronde Community of Oregon Yurok Tribe National Marine Sanctuary Foundation US Department of Commerce National Oceanic and Atmospheric Administration Office of National Marine Sanctuaries US Department of the Interior Bureau of Ocean Energy Management Pacific OCS Region December 31, 2017 This page intentionally left blank. DISCLAIMER This study was funded, in part, by the US Department of the Interior, Bureau of Ocean Energy Management (BOEM), Pacific Outer Continental Shelf (OCS) Region, Camarillo, CA, through Interagency Agreement Number M12PG00035 with the US Department of Commerce, National Oceanic and Atmospheric Administration (NOAA). This report has been technically reviewed by BOEM and it has been approved for publication. The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the opinions or policies of the US Government, nor does mention of trade names or commercial products constitute endorsement or recommendation for use. REPORT AVAILABILITY This report can be downloaded from the Bureau of Ocean Energy Management’s Recently Completed Environmental Studies – Pacific webpage at https://www.boem.gov/Pacific-Completed-Studies/. -

Listening Patterns – 2 About the Study Creating the Format Groups
SSRRGG PPuubblliicc RRaaddiioo PPrrooffiillee TThhee PPuubblliicc RRaaddiioo FFoorrmmaatt SSttuuddyy LLiisstteenniinngg PPaatttteerrnnss AA SSiixx--YYeeaarr AAnnaallyyssiiss ooff PPeerrffoorrmmaannccee aanndd CChhaannggee BByy SSttaattiioonn FFoorrmmaatt By Thomas J. Thomas and Theresa R. Clifford December 2005 STATION RESOURCE GROUP 6935 Laurel Avenue Takoma Park, MD 20912 301.270.2617 www.srg.org TThhee PPuubblliicc RRaaddiioo FFoorrmmaatt SSttuuddyy:: LLiisstteenniinngg PPaatttteerrnnss Each week the 393 public radio organizations supported by the Corporation for Public Broadcasting reach some 27 million listeners. Most analyses of public radio listening examine the performance of individual stations within this large mix, the contributions of specific national programs, or aggregate numbers for the system as a whole. This report takes a different approach. Through an extensive, multi-year study of 228 stations that generate about 80% of public radio’s audience, we review patterns of listening to groups of stations categorized by the formats that they present. We find that stations that pursue different format strategies – news, classical, jazz, AAA, and the principal combinations of these – have experienced significantly different patterns of audience growth in recent years and important differences in key audience behaviors such as loyalty and time spent listening. This quantitative study complements qualitative research that the Station Resource Group, in partnership with Public Radio Program Directors, and others have pursued on the values and benefits listeners perceive in different formats and format combinations. Key findings of The Public Radio Format Study include: • In a time of relentless news cycles and a near abandonment of news by many commercial stations, public radio’s news and information stations have seen a 55% increase in their average audience from Spring 1999 to Fall 2004. -

March 23-26, 2011 in San Luis Obispo
29th Annual Salmonid Restoration Conference Holding the Line on Species Decline March 23-26, 2011 in San Luis Obispo 2011 Conference Co-sponsors Alnus Ecological, Balance Hydrologics, Inc., California Department of Fish and Game, California Department of Water Resources, Cachuma Conservation Release Board, Cal Trout – North Coast, California Conservation Corps, CalTrans, Cardno Entrix, Casitas Municipal Water District, cbec, inc., Central Coast Salmon Enhancement, City of San Luis Obispo, City of Santa Barbara – Creeks Project, CONTECH, Fred Euphrat, McBain and Trush, Michael Love and Associates, Morro Bay National Estuary Program, NOAA Fisheries, Northern California Council of Federation of Fly-Fishers, Northwest Hydraulic Consultants, Pacifi c Coast Fish, Wildlife and Wetlands Restoration Association, Pacifi c States Marine Fisheries Commission, Pacifi c Watershed Associates, Pacifi c Gas & Electric Company, Philip Williams and Associates, Inc., Prunuske Chatham, Inc., Restoration Design Group, San Lorenzo Valley Water District, Solano County Water Agency, Sonoma County Water Agency, Stillwater Sciences, The Bay Institute, The Nature Conservancy, Trees Foundation, Trout Unlimited, U.S. Fish and Wildlife Service – CA/NV Fisheries, Winzler and Kelly Restoring Salmonids—Holding the Line on Species Decline SRF is pleased to be returning to San Luis Obispo for the 29th annual Salmonid Restoration Conference. Since last holding the conference in SLO in 2003, we’ve been to Davis, Fortuna, Santa Barbara, Santa Rosa, Lodi, Santa Cruz, and Redding. At each location, we focus on the issues in the local watersheds while including topics of wide ranging interest among the fi sheries restoration community. Each locale gives us an opportunity to consider a theme appropriate for the state of salmon fi sheries and the location of the conference. -

County Profile
FY 2020-21 PROPOSED BUDGET SECTION B:PROFILE GOVERNANCE Assessor County Counsel Auditor-Controller Human Resources Board of Supervisors Measure Z Clerk-Recorder Other Funds County Admin. Office Treasurer-Tax Collector Population County Comparison Education Infrastructure Employment DEMOGRAPHICS Geography Located on the far North Coast of California, 200 miles north of San Francisco and about 50 miles south of the southern Oregon border, Humboldt County is situated along the Pacific coast in Northern California’s rugged Coastal (Mountain) Ranges, bordered on the north SCENERY by Del Norte County, on the east by Siskiyou and Trinity counties, on the south by Mendocino County and on the west by the Pacific Ocean. The climate is ideal for growth The county encompasses 2.3 million acres, 80 percent of which is of the world’s tallest tree - the forestlands, protected redwoods and recreational areas. A densely coastal redwood. Though these forested, mountainous, rural county with about 110 miles of coastline, trees are found from southern more than any other county in the state, Humboldt contains over forty Oregon to the Big Sur area of percent of all remaining old growth Coast Redwood forests, the vast California, Humboldt County majority of which is protected or strictly conserved within dozens of contains the most impressive national, state, and local forests and parks, totaling approximately collection of Sequoia 680,000 acres (over 1,000 square miles). Humboldt’s highest point is sempervirens. The county is Salmon Mountain at 6,962 feet. Its lowest point is located in Samoa at home to Redwood National 20 feet. Humboldt Bay, California’s second largest natural bay, is the and State Parks, Humboldt only deep water port between San Francisco and Coos Bay, Oregon, Redwoods State Park (The and is located on the coast at the midpoint of the county. -
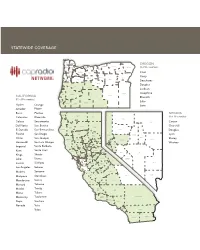
Statewide Coverage
STATEWIDE COVERAGE CLATSOP COLUMBIA OREGON MORROW UMATILLA TILLAMOOK HOOD WALLOWA WASHINGTON MULTNOMAH RIVER (9 of 36 counties) GILLIAM SHERMAN UNION YAMHILL CLACKAMAS WASCO Coos POLK MARION WHEELER Curry JEFFERSON BAKER LINCOLN LINN BENTON GRANT Deschutes CROOK Douglas LANE DESCHUTES Jackson MALHEUR Josephine COOS DOUGLAS HARNEY CALIFORNIA LAKE Klamath (51 of 58 counties) CURRY Lake KLAMATH JOSEPHINE JACKSON Alpine Orange Lane Amador Placer Butte Plumas NEVADA DEL NORTE SISKIYOU Calaveras Riverside MODOC (6 of 16 counties) HUMBOLDT Colusa Sacramento ELKO Carson Del Norte San Benito SHASTA LASSEN Churchill TRINITY El Dorado San Bernardino HUMBOLDT PERSHING Douglas TEHAMA Fresno San Diego WASHOE LANDER Lyon PLUMAS EUREKA Glenn San Joaquin MENDOCINO WHITE PINE Storey GLENN BUTTE SIERRA CHURCHILL STOREY Humboldt San Luis Obispo Washoe NEVADA ORMSBY LYON COLUSA SUTTER YUBA PLACER Imperial Santa Barbara LAKE DOUGLAS Santa Cruz YOLO EL DORADO Kern SONOMA NAPA ALPINE MINERAL NYE SACRAMENTO Kings Shasta AMADOR SOLANO CALAVERAS MARIN TUOLUMNE SAN ESMERALDA Lake Sierra CONTRA JOAQUIN COSTA MONO LINCOLN Lassen Siskiyou ALAMEDA STANISLAUS MARIPOSA SAN MATEO SANTA CLARA Los Angeles Solano MERCED SANTA CRUZ MADERA Madera Sonoma FRESNO SAN CLARK Mariposa Stanislaus BENITO INYO Mendocino Sutter TULARE MONTEREY KINGS Merced Tehama Trinity SAN Modoc LUIS KERN OBISPO Mono Tulare SANTA SAN BERNARDINO Monterey Tuolumne BARBARA VENTURA Napa Ventura LOS ANGELES Nevada Yolo ORANGE Yuba RIVERSIDE IMPERIAL SAN DIEGO CAPRADIO NETWORK: AFFILIATE STATIONS JEFFERSON PUBLIC STATION CITY FREQUENCY STATION CITY FREQUENCY FREQUENCY RADIO - TRANSLATORS KXJZ-FM Sacramento 90.9 KPBS-FM San Diego 89.5 Big Bend, CA 91.3 KXPR-FM Sacramento 88.9 KQVO Calexico 97.7 Brookings, OR 101.7 KXSR-FM Groveland 91.7 KPCC-FM Pasadena 89.3 Burney, CA 90.9 Stockton KUOP-FM 91.3 KUOR-FM Inland Empire 89.1 Callahan/Ft. -

Ryan Eric Emenaker ______1236 Chester Ct
Ryan Eric Emenaker _______________________________ 1236 Chester Ct. Arcata CA 95521 (707) 499-0368, [email protected] Education: M.A. Government, Summa Cum Laude , The Johns Hopkins University 2013 M.A. Social Science, Humboldt State University 2005 Future Faculty Preparation Certificate , Humboldt State University 2003 B.A. Political Science with minor in Sociology, Humboldt State University 2001 Teaching: College of the Redwoods- Professor 2009-Present Serving as Area Coordinator and Lead Faculty for Political Science Department. • POLSC 1: Political Controversies • POLSC 10: US Government & Politics • POLSC 12: State & Local Politics • POLSC 30: Campaigns & Elections • POLSC 13: Environmental Politics & Policy College of the Redwoods- Associate Faculty 2006- 2009 Humboldt State University- Guest Lecturer 2006- 2008 • SOC 494: Corporatization of Culture Prescott College- Adjunct Faculty 2004 • PSCI 400: Challenging Corporate Rule Humboldt State University Extended Education- Guest Lecturer 2003- 2004 • PSCI x371: Corporations vs. Democracy • HIST x371: Corporations & Democracy in American History College of the Redwoods- Student Teaching Intern 2003 • ENVS 10: Environmental Ethics Humboldt State University- Teaching Assistant & Discussion Leader 2001- 2003 • PSCI 220: Introduction to Political Theory • PSCI 371: Political Theory Discussion • HIST 111: American History since 1877 Awards & Honors: - The Dr. Eugene Portugal Award for Outstanding Faculty Research, College of the Redwoods 2014 - Best Master’s Thesis in the Area -

U.S.D.A. Forest Service
KRIS edition Lower-Middle Klamath Watershed Analysis United States Department of Agriculture Six Rivers National Forest Forest Service Orleans Ranger District Pacific Version 1.0 Southwest Region R5-MB-011 March 2003 Early Forest Service fire patrol plane. The first plane to land in Orleans, California circa 1920. This page intentionally left blank. Lower-Middle Klamath Watershed Analysis Version 1.0 U.S. Department of Agriculture Forest Service Pacific Southwest Region Six Rivers National Forest Orleans Ranger District Located within Humboldt County, Klamath Province, CA March 2003 Cover Photo: This photo was taken during a 4th of July celebration in the town of Orleans at the heart of the Lower-Middle Klamath Analysis area. In showing a group of Karuk elders and other townspeople posed in front of what was then the most modern piece of fire fighting equipment, it depicts several features related to the historical or reference condition of the Lower-Middle Klamath area. Within the photo are individuals who likely knew the time before Europeans arrived in Orleans and who witnessed the start of the modern fire suppression era. For Additional Information Contact: Six Rivers National Forest 1330 Bayshore Way Eureka, CA 95501 707-442-1721 Text (TTY) 707-442-1721 Voice http://www.r5.fs.fed.us/sixrivers The U.S. Department of Agriculture (USDA) prohibits discrimination in all its programs and activities on the basis of race, color, national origin, sex, religion, age, disability, political beliefs, sexual orientation, or marital or family status. (Not all prohibited bases apply to all programs.) Persons with disabilities who require alternative means for communication of program information (“Braille, large print, audiotape, etc.) should contact USDA’s TARGET Center at 202-720-2600 (Voice and TDD). -

Cooperative Program Tape Networks in Noncommercial EDRS
DOCUMENT RESUME ED 115 254 IR 002 798 AUTHOR Nordgren, Peter D. TITLE Cooperative Program Tape Networks in Noncommercial Radio. PUB DATE Dec 75 NOTE 94p. EDRS PRICE MF-$0.76 HC-$4.43 Plus Postage DESCRIPTORS *Cooperative Programs; *Educational Radio; Higher Education; *Programing (Broadcast); *Questionnaires; Shared Services; Statistical Data; Tables (Data) IDENTIFIERS Cooperative Program Tape Networks ABSTRACT Over 200 noncommercial radio stations responded to a survey to gather data on the characteristics of member stations and to sample the opinion of nonmembers toward a cooperative network concept. A second survey of 18 networks sought to gather indepth information on network operation. Results showed that 22.2 percent of the stations surveyed were participating in program cooperatives, and over 79 percent felt that network participation would be beneficial. It was concluded that the cooperative program tape network should continue in order to fulfill specialized programing needs. A copy of the two questionnaires, the letter of transmittal, and the mailing list is appended. A list of the networks that participated in the study, 12 statistical tables, and a 20-item bibliography are included. (Author/DS) lb *********************************************************************** * Documents acquired by ERIC include many informal unpublished * * materials not available from other sources. ERIC makes every effort * * to obtain the best copy available. Nevertheless, items of marginal * * reproducibility are often encountered and this affects the quality * *of the microfiche and hardcopy reproductions ERIC makes available * *via the ERIC Document ReproductionService (EDRS). EDRS is not * *responsible for the quality of theoriginal document. Reproductions* *supplied by EDRS are the best thatcan be made from the original. -

Yurok and the Klamath River
Yurok and the Klamath River: Yurok Historical Context and Data for Assessing Current Conditions and the Effects of the proposed Klamath Restoration Project on Yurok Tribal Trust Assets and Yurok Resources of Cultural and Religious Significance Report Prepared for the Department of the Interior Bureau of Indian Affairs For Use in the Secretarial Determination Overview Report and NEPA/CEQA Analysis Under Grant # 81333AG053 from US Fish and Wildlife Service Prepared by: Dr. Kathleen Sloan Yurok Tribe Environmental Program February 2011 TABLE OF CONTENTS I. Introduction: Purpose of Report 3 II. Yurok Tribe: Overview of Yurok History 7 III. Yurok Traditional Knowledge and the Klamath River 25 IV. Yurok Resources of Cultural and Religious Significance 43 V. Yurok Fishing Sites and Fishing Rights 47 VI. Yurok Beneficial Uses of the Klamath River and Tributaries 56 VII. Environmental Justice 70 VIII. Tribal Trust and Potentially Impacted Trust Assets 110 IX. Conclusions and Recommendations 120 X. References Cited 125 XI. Attachments 130 A. 1851 Treaty with the Poh-lik-lah B. 1973 USC 412 US 481 Mattz v. Arnett C. 1993 DOI Solicitors Opinion: Fishing Rights of the Yurok and Hoopa Valley Tribes D. 2006 DOI Cooperative Agreement: Cooperative Management of Tribal and Federal Lands and Resources in the Klamath River Basin in California 2 I. Introduction: Purpose of Report This report has been prepared under contract with the US Fish and Wildlife Service for the purpose of providing information to the Department of the Interior (DOI), the Secretary of the Interior, the Bureau of Indian Affairs (BIA) and all federal agencies involved in the Secretarial Determination and compliance with the National Environmental Policy Act (NEPA) and California Environmental Policy Act (CEQA) currently underway for the purposes of evaluating the proposed action of removing four Klamath River dams and implementing provisions set forth in the Klamath Basin Restoration Agreement (KBRA) and the Klamath Hydroelectric Settlement Agreement (KHSA). -

Regional Pedestrian Plan 2008
HUMBOLDT COUNTY REGIONAL PEDESTRIAN PLAN PREPARED BY: Alta Planning + Design Redwood Community Action Agency SHN Consultant Engineers PREPARED FOR: Humboldt County Association of Governments June 2008 TABLE OF CONTENTS I. INTRODUCTION......................................................................................................................................................1-1 1.1. Project Setting..................................................................................................................................................1-1 1.2. Overview of the Study Area..........................................................................................................................1-1 1.3. Plan Contents ..................................................................................................................................................1-2 II. PURPOSE OF THE PLAN.............................................................................................................................2-1 2.1. Need for Pedestrian Facilities in Humboldt County.................................................................................2-1 2.2. Previous Pedestrian Plans..............................................................................................................................2-1 2.3. Goals and Objectives......................................................................................................................................2-1 III. STUDY PROCESS................................................................................................................................................3-1 -

Public Law 100-580 102 Stat. 2924 Date Enacted: October 31, 1988
http://sorrel.humboldt.edu/~nasp/hoopa.html Public Law 100-580 102 Stat. 2924 Date Enacted: October 31, 1988 SYNOPSIS: An Act, To partition certain reservation lands between the Hoopa Valley Tribe and the Yurok Indians, to clarify the use of tribal timber proceeds, and for other purposes. Be it enacted by the Senate and House of Representatives of the United States of America in Congress assembled, Section 1. Short Title and Definitiions (a) Short Title--This Act may be cited as the "Hoopa-Yurok Settlement Act". (b) Definitions--For the purposes of this Act, the term-- (1) "Escrow funds" means the moneys derived from the joint reservation which are held in trust by the Secretary in the accounts entitled-- (A) "Proceeds of Labor- Hoopa Valley Indians-California 70 percent Fund, account number J52-561-7197"; (B) "Proceeds of Labor-Hoopa Valley Indians-California 30 percent Fund, account number J52-561-7236"; (C) "Proceeds of Klamath River Reservation, California, account number J52-562-7056"; (D) "Proceeds of Labor-Yurok Indians of Lower Klamath River, California, account number J52-562-7153"; (E) "Proceeds of Labor-Yurok Indians of Upper Klamath River, California, account number J52-562-7154"; (F) "Proceeds of Labor- Hoopa Reservation for Hoopa Valley and Yurok Tribes, account number J52-575-7256"; and (G) "Klamath River Fisheries, account number 5628000001"; (2) "Hoopa Indian blood" means that degree of ancestry derived from an Indian of the Hunstang, Hupa, Miskut, Redwood, Saiaz, Sermalton, Tish-Tang-Atan, South Fork, or Grouse Creek