Integrated Monitoring System Annual Report Cheshire and Merseyside 2016/17
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

North West Region Cheshire and North Wales
NATIONS, REGIONS & GROUPS NORTH WEST REGION LONDON REGION CHESHIRE AND NORTH WALES GROUPS HEATHROW GROUP Borderlands (Wrexham to Bidston) rail line Crossrail becomes Elizabeth Line full house greeted speaker John Goldsmith, Community A Relations Manager for Crossrail. Some 43km of new tunnelling is now complete under central London, and 65 million tonnes of material have been excavated. Building work on the whole line is now 87% complete. The first trains of the new Elizabeth Line are now in service between Liverpool Street and Shenfield where a new platform has been built for them, and the roof garden at the seven-storey Canary Wharf station has been open for some time. The 70 trains, built in Derby by Bombardier, are some 10–15% lighter than those now in use and will be in nine-car sets, 200m long, seating 450 passengers, with an estimated total capacity including standing passengers of 1,500 at peak times, most of The Borderlands line runs from Wrexham Central Station to Bidston Station whom are expected to be short-journey passengers. Seats will be sideways, forward facing and backward facing, giving plenty of his event was held in the strategic location of Chester, circulating space. The early trains now in service between T close to the border between England and Wales. The Liverpool Street and Shenfield are only seven cars long, because location chosen was apt, as the Borderlands line is a key the main line platforms at Liverpool Street will not accept nine-car strategic passenger route between North Wales and Merseyside. trains, but this is an interim measure until the lower level new John Allcock, Chairman, Wrexham–Bidston Rail Users’ Association station is operative. -

Pharmacy Name
Think Pharmacy Scheme Pharmacies - December 2019 Pharmacy Name Asda Pharmacy – Birkenhead – 222 Grange Rd, Birkenhead CH41 6EB Asda Pharmacy – Liscard – Seaview Road, Wallasey CH45 4NZ Asda Pharmacy – Upton – Woodchurch Road, Upton, CH49 5PD Asda Pharmacy – Bromborough – Welton Road, Croft Business Park, CH62 3QP Birkenhead Pharmacy – 31 Laird Street, Birkenhead CH41 8DB Blackheath Pharmacy – 113 Reeds Lane, Leasowe, CH46 1QT Boots – Birkenhead – 215 Grange Road, Birkenhead, Merseyside, CH41 2PH Boots – Bromborough Retail Park – Welton Road, Croft Retail Park, Bromborough, CH62 3PN Boots – Manor Health Centre – Manor Health Centre, Liscard Village,Wallasey, CH45 4JG Boots – Higher Bebington – 118 Teehey Lane, Bebington, Wirral CH63 8QT Boots – West Kirby – 11-13 The Crescent, West Kirby, CH48 4HL Boots – Rock Ferry – 206 Bedford Road, Birkenhead CH42 2AT Boots – Noctorum Upton Road – 395 Upton Road, Birkenhead CH43 9SE Boots – Bromborough The Precinct – 3-5 The Rake Precinct, Bromborough, CH62 7AD Boots – Moreton – 254 Hoylake Road, Moreton, CH46 6AF Boots – Greasby – 148 Greasby Road, Greasby, CH49 3NQ Boots – Upton – 23 Arrowe Park Road, Wirral, CH49 0UB Boots – Bidston – 30 Hoylake Road, Birkenhead CH41 7BX Boots – Arrowe Park – 156 Common Field Rd, Woodchurch, Wirral CH49 7LP Boots – Thingwall – 509 Pensby Road, Wirral, CH61 7UQ Boots – Prenton Woodchurch Road – 379 Woodchurch Rd, Birkenhead CH42 8PE Boots – Heswall – 218-220, Telegraph Road, Heswall, CH60 0AL Boots – Prenton Holmlands Drive – 8-10 Holmlands Dr, Birkenhead CH43 0TX -

492 Bus Time Schedule & Line Route
492 bus time schedule & line map 492 Birkenhead - Birkenhead View In Website Mode The 492 bus line Birkenhead - Birkenhead has one route. For regular weekdays, their operation hours are: (1) Birkenhead: 7:12 AM - 9:10 PM Use the Moovit App to ƒnd the closest 492 bus station near you and ƒnd out when is the next 492 bus arriving. Direction: Birkenhead 492 bus Time Schedule 55 stops Birkenhead Route Timetable: VIEW LINE SCHEDULE Sunday 9:27 AM - 5:10 PM Monday 7:12 AM - 9:10 PM Grange Road, Birkenhead Oliver Lane, Birkenhead Tuesday 7:12 AM - 9:10 PM Birkenhead Bus Station, Birkenhead Wednesday 7:12 AM - 9:10 PM 2a Princes Pavement, Birkenhead Thursday 7:12 AM - 9:10 PM Catherine Street, Birkenhead Friday 7:12 AM - 9:10 PM Cook Street, Birkenhead Saturday 8:55 AM - 9:10 PM Clayton Place, Birkenhead Oak Bank, Birkenhead Cartmel Close, Birkenhead 492 bus Info Woodchurch Road, Oxton Direction: Birkenhead Princess Terrace, Birkenhead Stops: 55 Trip Duration: 53 min Lynn Bank, Oxton Line Summary: Grange Road, Birkenhead, Lynnbank, Birkenhead Birkenhead Bus Station, Birkenhead, Catherine Street, Birkenhead, Cook Street, Birkenhead, Oak Columbia Road, Oxton Bank, Birkenhead, Woodchurch Road, Oxton, Lynn Bank, Oxton, Columbia Road, Oxton, Arnside Road, Arnside Road, Oxton Oxton, Beresford Road, Oxton, Kingsmead Road, Oxton, Shrewsbury Close, Oxton, Tollemache Road, Beresford Road, Oxton Claughton, Upton Road, Claughton, Bidston Avenue, Shrewsbury Road, Birkenhead Birkenhead Park, Plumer Drive, Birkenhead, Dundonald Street, Birkenhead, Arkle Road, -

Birkenhead Bidston/Moreton
BIDSTON/MORETON "HEALTHY HIGHWAY/KEY-WORKERS CORRIDOR" - FENDER LANE. Existing layout provides 2 lanes of vehicular traffic in each direction, with overall carriageway width per 2 lanes approx. 7.6m. NCR Proposal is to provide one lane for vehicular traffic and one lane "Healthy Highway" in each direction. Each approx. 3.8m wide comprising of a 2.3m WALLASEY 56 wide cycle lane separated from traffic by a 1.2m wide hatched mandatory road marking and wand/orca light segregation infrastructure. In terms of Key Workers, both Moreton and Bidston/Birkenhead have several care homes, doctors, health centres, chemists, sheltered accomodation, BIDSTON CYCLE LINK assisted living facilities, schools and a specialist college. With most "journeys" being short distance the proposal provides a viable alternative to those needing to get from A to B that either do not have access to car, are avoiding public transport as per government guidelines, or have always wanted to NCR walk/cycle this route but have never been able to do so. 56 In terms of local economy & employers, in the immediate vicinity of the link at the Moreton end is an ALDI supermarket, Tesco Express, and a hub of JCT 1 shops/supermarkets found at Moreton Cross. Beyond Moreton directly lies Leasowe, Meols, Hoylake, West Kirby, Upton and Arrowe Park. At the RETAIL Bidston end lies a Tesco Superstore, Jct 1 Retail Park (containing ALDI, M&S, B&Q, Halfords, Home Bargains etc) and the long hub of shops found BIDSTON TRAIN STATION PARK along Bidston and Birkenhead North. Beyond Bidston lies Birkenhead North and Birkenhead Town Centre. -

WALK 1 Bidston Hill & River Fender
Information WALK 1 Bidston Hill & River Fender WALK 2 The Wonders of Birkenhead This Walk and Cycle leaflet for Wirral covers the north eastern quarter and is one of a series of A circular walk starting at the Tam O’Shanter 2a Turn left onto Noctorum Lane. Follow this grows in the shallow sandy soils. Follow the main path Birkenhead has some fascinating historical traffic lights and turn left into Ivy Street, following 7 From the Transport Museum retrace your steps four leaflets each consisting of three walks and Urban Farm, this route takes you across Wirral unsurfaced lane to the junction with Budworth Road. along this natural Sandstone Pavement. The Windmill attractions and if you haven’t yet discovered the Birkenhead Priory sign on your right. Birkenhead back to Pacific Road where there is the Pacific Road one cycle route. Cross with care as there is a blind bend to the right. should now be coming into view. Priory is at the end of Priory Street on the left. This Arts Centre and on towards the river to view the Ladies Golf Course, along the River Fender and Continue along Noctorum Lane past Mere Bank on the them you may be pleasantly surprised. This walk former Benedictine monastery has an exhibition and the is Mersey Tunnel Ventilation Tower. The architect who 8 Continue to the iron footbridge above the deep rocky I have recently updated all 12 walks based on back to the heights of Bidston Hill with views of right. Continue straight ahead. The track swings right visits ten of them. -
Get the PDF Route Pack
Directions Climb the steps up to the footbridge at Bidston train station and bear left. Descend the steps and continue down the footpath angling off to the right. Cross the bridge over the water. Turn right and head onto the signposted cycle path, marked by a big black sign with a tag on it. Cross the road by walking under the bridge, taking note of the graffiti on the left where the path turns into stones and gravel. Continue along the path. You will see a turn off to the left, but walk straight on. When you have been walking for about 10 minutes, with the train tracks to your right and marsh and vegetation to your left, the path will take a left. Bear right at the signpost to Bidston Moss, towards the big road bridges. Here you might like to take a detour by walking off the path to the left in order to look at the street art on some of the concrete bridge uprights. If you walk up towards the railway line in between the two road bridges, you will discover some large and interesting artworks. After exploring the artwork go back to the path and up the ramp towards the footbridge. Be aware that a lot of cyclists use this route, so keep an eye out. There is a left turn on the footbridge, but keep going straight across onto Bidston Moss. You should see a sign post on the right hand side welcoming you to the Moss. Follow the footpath downhill around to the left which will lead you on to a tarmac path. -
ODS Codeparent Service Public Name Postal Address Postal Code
BOXING DAY NEW YEAR'S XMAS DAY 26/12/2020 (in leiu) DAY ODS CodeParent Service Public Name Postal Address Postal Code Phone Public 25/12/2020 28/12/2020 01/01/2021 FV704 Eastern Cheshire Well Pharmacy 4 Park Lane, Poynton SK12 1RE 01625 872214 14.00 - 16.00 FG757 Eastern Cheshire WELL Pharmacy - Fountain Square - Disley 11 Fountain Square, Disley, Cheshire, SK12 2AB 01663 762048 14:00-16:00 FH709 Eastern Cheshire Andrews Pharmacy - Kennedy Avenue - Macclesfield71 Kennedy Avenue, Macclesfield SK10 3DE 01625 618481 10:00-12:00 09:00-12:30 FHM07 Eastern Cheshire Lloyds Pharmacy - West Street - Congleton 41A West Street, , Congleton, , CheshireCW12 1JN 01260 275523 12:00-14:00 09:00-13:00 FPF22 Eastern Cheshire Boots Pharmacy - King Street - Knutsford 64 King Street, Knutsford, , WA16 6DT 01565 633114 14:00-16:00 08:30-17:30 10:30-16:30 FTH54 Eastern Cheshire WELL Pharmacy - Bollin House - Macclesfield Bollin House, Sunderland Street, MacclesfieldSK11 6JL 01625 422927 12:00-14:00 FYA25 Eastern Cheshire Cedrics Chemist - Festival Hall - Alderley Edge FESTIVAL HALL, TALBOT ROAD , ALDERLEYSK9 EDGE 7HR 01625 583145 10:00-12:00 09:00-14:00 FA539 Eastern Cheshire Boots Pharmacy - Bridge Street - Congleton 14-16 Bridge Street, Congleton, Cheshire,CW12 1AY 01260 273153 09:00-17:30 FAY71 Eastern Cheshire Peak Pharmacy - Weston Square - Macclesfield5-6 Weston Square, Macclesfield SK11 8SS 01625 423465 09:00-13:00 FC072 Eastern Cheshire WELL Pharmacy - Wilmslow Road - Handforth 110 Wilmslow Road, Handforth SK9 3ES 01625 523945 09:00-13:00 FCN20 Eastern -

6 Merseyside
6 Merseyside 6.1 Administrative set-up Merseyside takes its name from the River Mersey and is a metropolitan county in North West England. Merseyside came into existence as a metropolitan county in 1974, after the passage of the Local Government Act 1972, and the county consists of five metropolitan boroughs adjoining the Mersey Estuary, including the City of Liverpool. Merseyside encompasses about 645 km2 (249 sq miles) and has a population of around 1,350,100 (Office of National Statistics). Number of Males Females Total Area Merseyside people per (thousands) (thousands) (thousands) (hectares) hectare Knowsley 71.7 79.1 150.8 8629.3 17.48 Liverpool 212.7 222.8 435.5 11159.08 39.03 Sefton 131.3 144.9 276.2 15455.66 17.87 St Helens 86.5 91 177.5 13589.08 13.06 Wirral 147.7 162.4 310.1 15704.9 19.75 Total 649.9 700.2 1350.1 64538.02 107.19 Table 3 Demographics of Merseyside (sourced various from ONS www.statistics.gov.uk) Merseyside County Council was abolished in 1986, and so its districts (the metropolitan boroughs) are now essentially unitary authorities. However, the metropolitan county continues to exist in law and as a geographic frame of reference. Merseyside is divided into two parts by the Mersey Estuary: the Metropolitan Borough of Wirral is located to the west of the estuary on the Wirral Peninsula; the rest of the county is located on the eastern side of the estuary. The eastern boroughs of Merseyside border Lancashire to the north and Greater Manchester to the east, and both parts of Merseyside, west and east of the estuary, border Cheshire to the south. -

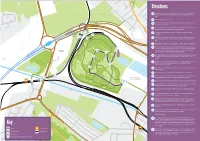
Bidston Moss Bidston, North Wirral, Merseyside Regeneration Benefi Ts the Objectives and Outomes of the Bidston Moss Project Are to
Site context plan Bidston Moss Bidston, North Wirral, Merseyside Regeneration benefi ts The objectives and outomes of the Bidston Moss Project are to : • Transform 68 hectares of previously developed brownfi eld land to community woodland • Provide image improvements for the City Region of Liverpool through woodland creation around Junction 1, M53 and along a main rail route to the city, supporting strategic investments for Capital of Culture 2008 • Delivers a beacon site within the Mersey Waterfront Regional Park • Create a zone of infl uence around the project area that will make it a more competitive choice for indigenous and inward business investment • Improves 3 Super Output Areas (SOA) in Inner Wirral that are within the top 5% of the national Index of Multiple Deprivation (IMD) • Contribute to Merseyside’s Biodiversity Action Plan targets • Improve and create safe access routes to local businesses, schools and residential areas • Create a sub-regional cycling facility that contributes to the National Cycle Route Network Project location Strategic investment Site biography Site: Bidston Moss Where: Bidston, North Wirral Size: 68 hectares The Bidston Moss Project is The former Cross Lane Tip Local Nature Reserve (WMBC) to work in partnership with located in Birkenhead, overlooking (WMBC) Land located in between the River Groundwork Wirral who has junction 1 of the M53 and close The former Cross Lane Tip was Birket, the M53 and the A554, been a key delivery partner in the to the entrance of the Mersey a domestic refuse tip for WMBC was previously used as a borrow restoration of the former landfi ll Tunnel. -

THE LONDON GAZETTE, NOVEMBER 24, 1899. 7845 Contained in the Schedule to the Electric Lighting- the Following Are the Streets and Places Clauses Act, 1899
THE LONDON GAZETTE, NOVEMBER 24, 1899. 7845 contained in the Schedule to the Electric Lighting- The following are the streets and places Clauses Act, 1899. within which the Undertakers propose to lay And notice is hereby given, that the draft of lectric linos within a specified time, viz:— the Order will be deposited at the offices of the The road, called Eleanor-road, between Bid- Board of Trade on or before the 21st. day of ston Hall Farm-yard and Upton-road. December next, and printed copies of the draft The public highway, known as Upton-road, at Order, when deposited, and of the Order, when the point where that road intersects Vyner- made, may be obtained (at the price of one road. shilling for each copy) at the offices of the The road called Vyner-road (leading from Clerk to the Council, 9, Welsh-row, Nantwich, Uptou-road), from a point opposite Eleanor- and at the office of the undermentioned Solicitor road to Bidston-road. and Parliamentary Agents respectively. The Bidston-road fram the termination of And notice is hereby further given, that a Vyner-road to the junction of Bidston-road map showing the boundaries of the proposed and Upton-road. area of supply, and the streets in which it is pro- The road leading from Vyner-road, passing in prosed that electric lines shall be laid down with- front of the house known as " Chenotrie," in a specified time, and a copy of this advertise- to and terminating at or near to Noctorum- ment, as published in the London Gazette, will farm at the junction of the Noctorum Cross- be deposited on or before the 30th day of roads. -

NHS England Cheshire and Merseyside: Lots and Locations
NHS England Cheshire and Merseyside: Lots and locations Local Proposed Lot names Related wards Related post codes Authority / Location of (including but not provider exclusively) Cheshire Cheshire East (East) Alderley Edge, Bollington, Chelford, Congleton, CW4, CW12, SK9, SK10, East Disley, Handforth, Holmes Chapel, Knutsford, SK11, SK12, WA16 Macclesfield, Mobberley, Poynton, Prestbury, Wilmslow Cheshire East (South) Alsagar, Audlem, Crewe, Middlewich, Nantwich, CW1, CW2, CW5, CW10, Sandbach, Scholar Green, Wrenbury CW11, ST7 Cheshire Cheshire West & Barnton, Lostock Gralam, Northwich, Sandiway, CW7, CW8, CW9 West and Chester (East) Weaverham, Winsford Chester Cheshire West & Chester, Farndon, Malpas, Tarvin, Tattenhall, CH1, CH2, CH3, CH4, (includes Chester (West) Kelsall, Bunbury, Tarporley, Frodsham, Helsby, CW6, SY14, WA6 Vale Royal) Ellesmere Port, Neston, Great Sutton, Little Sutton, Neston, Elton, Willaston Halton Halton Hough Green, Runcorn, Widnes WA7,WA8 Knowsley - Halewood, Huyton, Kirkby, Stockbridge Village, L14, L25, L26, L28, L32, Whiston L33, L34, L35, L36 Liverpool Liverpool North Aintree, Warbreck, Fazakerley, Croxteth, L4, L5, L9, L10, L11, L13 Clubmoor, Norris Green, Kirkdale, Anfield, (Clubmoor) Everton, Walton Liverpool South Riverside, Toxteth, Prince’s Park, Greenbank, L1 (Riverside), L8,L12 Church, Woolton, St Michaels', Mossley Hill, (Greenbank),L17, L18, Aigburth, Cressington, Allerton, Hunts Cross, L19, L24, L25 Speke, Garston, Gatacre Liverpool East Central, Dovecot, Kensington, Fairfield, Tuebrook, L1 (Central), -

Palliative Care Medicines Supply – Primary Care
Palliative Care Medicines Supply – Primary Care COVID-19 Suspected or Confirmed The COVID-19 pandemic has changed the way patients are reviewed in primary care and will increase demand for palliative care medicines as more patients are palliated in their usual place of residence, be it care home or own home. It is noted that demise from COVID-19 in the frail and elderly has been sadly very rapid and the need for palliation in this scenario is for short time periods. This document describes the various clinical streams through which patients may be managed. The main aim of this document is to facilitate the timely access to medicine for patients (NHSE recommendation is <1hour from prescription to delivery1) and to preserve stock / reduce wastage as these medicines are likely to be subject to supply shortages. Amendments may be made to the appendices within this document without a full review of this document. Relevant parties will be notified of any updates. 1.0 Discharge from Hospice or Acute Trust to Usual Place of Residence • Ward based prescriber (medical and non-medical) to generate prescription in accordance with usual process by ward based prescribers Electronic signature acceptable for St John’s Hospice or WUTH for supply (wet ink requirement relaxed during COVID-19 period by CDAO-WUTH). • Ward based prescriber or pharmacist to generate PMAC (patient medicines administration chart). This is a direct transcription of the discharge prescription. • Ward to document on TTH which community-based team will be taking over care in the community on discharge and contact details e.g.