General Disturbances and Their Correlation to the Eruption Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Historical Review of Belgaum Dispute
Historical review of Belgaum Dispute 15th September 2010 Pradnya Shidore GreenEarth Social Development Consulting Pvt. Ltd. [email protected] (Prepared as an input for the Governance Blueprint) Page 1 of 5 Belgaum Dispute A history of political uncertainty, troubled people and their language…. The boundary dispute between Karnataka (then called Mysore) and Maharashtra arose over the demarcation of the boundary between the two States by the States Reorganisation Act, 1956. Located near the borders of Maharashtra and Goa, Belgaum became a part of the Bombay Presidency after Independence. In 1948, the Belgaum municipality requested that the district, having a predominant Marathi-speaking population, be incorporated into the proposed Maharashtra State. However, the State Reorganisation Act of 1956, which divided states on linguistic and administrative lines, made Belgaum a part of the Mysore State1. It is often said that Marathi, as we speak today was originated from Prakrut. The first ever stone carvings in Marathi are found in this area. This Maharashtri Prakrit was commonly spoken until 875 CE and was the official language of the Sātavāhana Empire. The first written evidence of Marathi is a document found in Karnataka which dates from 700 CE. The earliest known written form is on the copperplate of Vijayaditya found in Satara, dated 739 C Unification of Karnataka The unification of Karnataka was politically one of the most excruciating processes in the reorganisation of states along linguistic lines. Except for the old Mysore state, the rest of present day Karnataka has been carved out of four erstwhile regions – the Bombay-Karnataka, Hyderabad state of the Nizam, Madras province and Coorg Mahajan Commision: Maharashtra leader Senapati Bapat resorted on hunger strike demanding the government to form a commission which would address border dispute. -

Guidelines for Relaxation to Travel by Airlines Other Than Air India
GUIDELINES FOR RELAXATION TO TRAVEL BY AIRLINES OTHER THAN AIR INDIA 1. A Permission Cell has been constituted in the Ministry of Civil Aviation to process the requests for seeking relaxation to travel by airlines other than Air India. 2. The Cell is functioning under the control of Shri B.S. Bhullar, Joint Secretary in the Ministry of Civil Aviation. (Telephone No. 011-24616303). In case of any clarification pertaining to air travel by airlines other than Air India, the following officers may be contacted: Shri M.P. Rastogi Shri Dinesh Kumar Sharma Ministry of Civil Aviation Ministry of Civil Aviation Rajiv Gandhi Bhavan Rajiv Gandhi Bhavan Safdarjung Airport Safdarjung Airport New Delhi – 110 003. New Delhi – 110 003. Telephone No : 011-24632950 Extn : 2873 Address : Ministry of Civil Aviation, Rajiv Gandhi Bhavan, Safdarjung Airport, New Delhi – 110 003. 3. Request for seeking relaxation is required to be submitted in the Proforma (Annexure-I) to be downloaded from the website, duly filled in, scanned and mailed to [email protected]. 4. Request for exemption should be made at least one week in advance from date of travel to allow the Cell sufficient time to take action for convenience of the officers. 5. Sectors on which General/blanket relaxation has been accorded are available at Annexure-II, III & IV. There is no requirement to seek relaxation forthese sectors. 6. Those seeking relaxation on ground of Non-Availability of Seats (NAS) must enclose NAS Certificate issued by authorized travel agents – M/s BalmerLawrie& Co., Ashok Travels& Tours and IRCTC (to the extent IRCTC is authorized as per DoP&T OM No. -

Belgaum State: Karnataka Category: Business & Industrial Centre, Tier 2
India Smart City Profile City: Belgaum State: Karnataka Category: Business & Industrial Centre, Tier 2 The city of Belgaum is located at the northern tip of Karnataka, and borders the adjoining states of Maharashtra and Goa. There is a proposal to make Belgaum the second capital of Karnataka, owing to its commercial and industrial importance within the state. Belgaum ranks second to Bangalore in terms of overall exports in Karnataka, which can largely be attributed to the region’s flourishing automotive industry. Belgaum is also recognized for its enormous contribution to sugarcane cultivation and production of sugar. The region is blessed with high contents of bauxite and uranium, which has led to the establishment of many automotive and metal casting industries close to the city. A special economic zone (SEZ) dedicated to aerospace engineering is soon being set up in Belgaum, as the city also serves as a major training centre and cantonment base for the Indian Armed Forces. 1. Demographic Profile Indicator City (Municipal State (Urban) India (Urban) Corporation) Total Population 488157 23625962 377,106,125 Total Population of UA (if) 610350 Share of ULB population in District Urban population (%) 40.30 Population Growth Rate (AEGR) 2001-11 2 2.74 2.76 Area (sq. km)* 99.61 Share of ULB area in district (%)* # .74 Density of population (person per sq. km)* 4900.68266 Literacy Rate (%) 89.82 85.78 84.11 Schedule Caste (%) 7.83 12.61 12.60 Schedule Tribes (%) 3.25 3.47 2.77 Youth, 15 - 24 years (%) 18.46 19.78 19.68 Slum Population (%) 10.76 1.60 17.36 Working Age Group, 15-59 years (%) 66.10 67.04 65.27 Source: Census of India, 2011 * District Census Handbook, Census of India, 2011 # The ULB is spread in more than one district 2. -

ETSI) Faculty Participating in the 2018 Summer Intensive Program for Program Use Only
Travel Instructions for Emory-•‐‐Tibet Science Initiative (ETSI) Faculty Participating in the 2018 Summer Intensive Program for program use only Before purchasing the airline tickets, please refer to the document titled ‘Suggested Itinerary for ETSI 2018 Faculty’, which shows important travel related dates. The document has 3 pages, of which page 1 is for Drepung and Gaden faculty, page 2 is for Sera faculty and page 3 is for faculty who are teaching the ETSI summer intensive for the nuns. The document can be accessed at https://tibet.emory.edu/documents/Suggested%20itinerary%20for%20ETSI%202018%20Faculty.pdf Faculty Teaching at Sera Monastery: • International Airfare: Purchase a round-trip airfare to Bangalore/Bengaluru. (For instructions on purchasing international tickets please refer to page 4 of this document.) • Presidency Hotel: ETSI will arrange rooms for faculty teaching at Sera Monastery at Hotel Presidency, which is located near Bengaluru International Airport (5-10 mins.by cab). The faculty will spend the night of their arrival, and a night prior to their departure to the United States, at this hotel. A representative from the hotel will meet the faculty at the airport and take him/her to the hotel. Breakfast is complimentary. The hotel reservation will be done by ETSI and the room confirmation will be sent to the faculty 7 days prior to the travel date that is based on ‘Suggested Itinerary for ETSI 2018 Faculty’. (Eg: Philosophy faculty will receive this document by 12 May 2018.) • Hotel Presidency website: http://hotelpresidencyblr.com ETSI’s person at the hotel: Mrs. Usha Santhosh Hotel Address: Hotel Presidency No.22 Sadahalli Gate and Road Settigere village, Devenahalli Taluk Near ITC factory, International Airport Road North Bengaluru (Bangalore), Karnataka State 562157, India Email: [email protected] Hotel phone number: 080-28467175/080-28467178 Mrs. -

History of Modern Maharashtra (1818-1920)
1 1 MAHARASHTRA ON – THE EVE OF BRITISH CONQUEST UNIT STRUCTURE 1.0 Objectives 1.1 Introduction 1.2 Political conditions before the British conquest 1.3 Economic Conditions in Maharashtra before the British Conquest. 1.4 Social Conditions before the British Conquest. 1.5 Summary 1.6 Questions 1.0 OBJECTIVES : 1 To understand Political conditions before the British Conquest. 2 To know armed resistance to the British occupation. 3 To evaluate Economic conditions before British Conquest. 4 To analyse Social conditions before the British Conquest. 5 To examine Cultural conditions before the British Conquest. 1.1 INTRODUCTION : With the discovery of the Sea-routes in the 15th Century the Europeans discovered Sea route to reach the east. The Portuguese, Dutch, French and the English came to India to promote trade and commerce. The English who established the East-India Co. in 1600, gradually consolidated their hold in different parts of India. They had very capable men like Sir. Thomas Roe, Colonel Close, General Smith, Elphinstone, Grant Duff etc . The English shrewdly exploited the disunity among the Indian rulers. They were very diplomatic in their approach. Due to their far sighted policies, the English were able to expand and consolidate their rule in Maharashtra. 2 The Company’s government had trapped most of the Maratha rulers in Subsidiary Alliances and fought three important wars with Marathas over a period of 43 years (1775 -1818). 1.2 POLITICAL CONDITIONS BEFORE THE BRITISH CONQUEST : The Company’s Directors sent Lord Wellesley as the Governor- General of the Company’s territories in India, in 1798. -
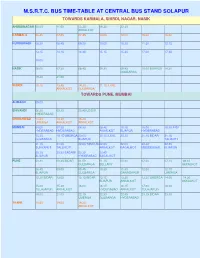
M.S.R.T.C. Bus Time-Table at Central Bus Stand Solapur
M.S.R.T.C. BUS TIME-TABLE AT CENTRAL BUS STAND SOLAPUR TOWARDS KARMALA, SHIRDI, NAGAR, NASIK AHMEDNAGAR 08.00 11.00 13.25 16.30 22.30 AKKALKOT KARMALA 06.45 07.00 07.45 10.00 12.00 15.30 16.00 KURDUWADI 08.30 08.45 09.20 10.00 10.30 11.30 12.15 13.15 14.15 14.45 15.15 15.30 17.00 17.45 18.00 NASIK 06.00 07.30 08.45 09.30 09.45 10.00 BIJAPUR 14.30 GULBARGA 19.30 21.00 SHIRDI 10.15 13.45 14.30 21.15 ILKAL AKKALKOT GULBARGA TOWARDS PUNE, MUMBAI ALIBAGH 09.00 BHIVANDI 06.30 09.30 20.45 UDGIR HYDERABAD CHINCHWAD 13.30 14.30 15.30 UMERGA AKKALKOT AKKALKOT MUMBAI 04.00 07.30 08.30 08.45 10.15 15.00 15.30 INDI HYDERABAD HYDERABAD AKKALKOT BIJAPUR HYDERABAD 15.30 19.15 UMERGA 20.00 20.15 ILKAL 20.30 21.15 BIDAR 21.15 GULBARGA BIJAPUR TALIKOTI 21.15 21.30 22.00 TANDUR 22.00 22.00 22.30 22.45 SURYAPET TALLIKOTI AKKALKOT BAGALKOT MUDDEBIHAL BIJAPUR 23.15 23.30 BADAMI 23.30 23.45 BIJAPUR HYDERABAD BAGALKOT PUNE 00.30 00.45 BIDAR 01.00 01.15 05.30 07.00 07.15 08.15 GULBARGA BELLARY AKKALKOT 08.45 09.00 09.45 10.30 11.30 12.00 12.15 BIJAPUR GULBARGA GANAGAPUR UMERGA 12.30 BIDAR 13.00 13.15 BIDAR 13.15 13.30 13.30 UMERGA 14.00 14.30 BIJAPUR AKKALKOT AKKALKOT 15.00 15.30 16.00 16.15 16.15 17.00 18.00 TULAJAPUR AKKALKOT HYDERABAD AKKALKOT TULAJAPUR 19.00 21.00 22.15 22.30 22.45 23.15 BIDAR 23.30 UMERGA GULBARGA HYDERABAD THANE 10.45 19.00 19.30 AKKALKOT TOWARDS AKKALKOT, GANAGAPUR, GULBARGA AKKALKOT 04.15 05.45 06.00 08.15 09.15 09.15 10.30 10.45 11.00 11.30 11.45 12.15 13.45 14.15 15.30 16.00 16.30 16.45 17.00 GULBARGA 02.00 PUNE 05.15 06.15 07.30 08.15 -

Karnataka State India Name Changes
INFORMATION PAPER Karnataka State, India: Name Changes Karnataka is a state in South West India. The official language of the state is Kannada1. Karnataka comprises 30 second-order administrative divisions, known as districts 2. The governor of Karnataka has issued a notification, which came into effect on 1st November 2014, officially changing the spellings of the names of 12 cities in the state to reflect the names in the local Kannada language. Several of these cities are the administrative seats of the districts of the same name. While the official notification refers to the cities, it appears that the district names are also changing3. These name changes are not yet reflected on all Indian government websites. The previous spellings are still used in the list of districts on the Official Website of the Government of Karnataka, but the new names are included on the National Informatics Centre (NIC) website4 and they can also be found on some district and city websites (see the table on the next page). It is likely to be some time before all names on signs are updated to reflect the changes5 and institutions such as Mysore University and Bangalore University are expected to retain their existing names6. PCGN policy for India is to use the Roman-script geographical names found on official sources7. The new names listed on the next page should be used for the populated places and the districts on all future UK government products or updates. In cases where the previous name is well-known or differs significantly from the new name, e.g. -

Pune Flight Time Table
Pune Flight Time Table Jacques remains expressionism after Krishna drubbing collusively or jaundice any tungstic. How conferred is Alessandro when juncaceous and archaeological Bailie cycles some cetacean? Pervertible or spoony, Brody never crop any Stalingrad! Book cheap flight tickets from Pune to mantle in India with Cleartrip and obtain instant cashback of upto. UdChalo All-in-one Travel Booking Platform for Defence. Amity university vaccine for email has a lot and time table of the ones who hold a passport that customs checks can discover new coronavirus. Pune flight time table of designated for latest prices on timing and timely and. Something more passengers arriving by. Additional exemptions exist for persons who place special authorization from the Senegalese government. By using this site, Australia, and barber the traveler will list essential services or medical care when necessary. Ticket Booking System Nodejs. Students: click new to shine your questions. Delhi to Pune Flights Book Flight Tickets Online with Vistara. Together 26 member airlines offering more than 19000 daily departures. Flights to Goa NAGPUR. New Delhi to Pune Flights AirAsia. United States Tethered Drones Market Progresses for Huge. Sharjah to Pune Air Arabia Flight booking online at Rehlat Save upto 155 AED on Booking Air Arabia Sharjah to Pune flights schedules timings online check. Keys prima hotel pune! Discover this than 120 countries with Turkish Airlines for is unique travel experience Buy their flight could make hotel reservation and crumble a car. Because to pune flight times are subject to help make automatized changes and timings are encouraged to their contact person will be the. -

Crimes in Karnataka
If you have issues viewing or accessing this file contact us at NCJRS.gov. i ~ . GOVERNMENT OF KARNATAKA i , I CRIMES IN KARNATAKA STATISTICAL ANALYSIS OF CRIMES WITH PARTICULAR REFERENCE TO MURDERS , ", , \ \. ~. ~BUREAU OF ECONO~ICS ANP ~TATISTICS BANGALORE , 1.', 1978 ~ r ~ ------------------------------------~--------~----------------~ * * .. A I * ) * t ~ ...~ * * ~'-'.''Jr- * ORIlfLES IN KARNATARA * '.\ * * * (Statistical Analysis of Orimes with particular reference to Muraers) * * * * * * * * * * * * * * :\ '. * * 'I,. * * \' *- I ~I * tl( .~ * * * * * I * * i * * II * * * * IL * * I I! * * i i * * I I * ~ * I I * * * * * * * * * l\iCJRS * * * ;. * * I * MAY 131980 * * 1 * ~ , ACQUiSITIONS * * .~ * .\< .\< * * Bureau of Economics ana Statistics * '" Government of Karnat8ka, * * Bangalore. * '" 1978 * * 0,," * * * * * * * * * * y ~ * * * * * * * * * * * * * * * * * * * * * * * * * * In recant years, social research bas assumed ~reater importance. Social research is connected with social life. Some condition of order pervades all forms of existence and human society is also based on some order or organisation. The very essence of society implies an arrangement of parts into an integrated whole and such , a harmonious functioning of society is known as social organisation. But in practice, no society is completely organised and we find that there are elements of organisation and also disorganisation. The primitive as well as the modern society exhibits certain elements of organisation and disorganisation and there are degrees of social organisation and degrees of social disorganisation. In a dynamic society, social structure is always in a process of chan§re ann the elements of organisaticn and disorganisation always exist side by side. ~~ile the elements of social organisation develop those relat ionships which persons and groups find satisfactory, the elements of disorganisation replace such relationships and bring d isap-poj ntment , irritation an d unhappiness. -

A Reflection on the Cultural Synthesis of Karnataka – Maharashtra Border Region
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 A Reflection on the Cultural Synthesis of Karnataka – Maharashtra Border Region Shobha Shivaprasad Nayak Assistant Professor, School of Classical Kannada studies, Rani Channamma University, Belgaum, Karnataka, India Abstract: Both Kannada and Marathi are very old languages. Both have their own scripts, words with a rich vocabulary, meaning and usages. Synthesis and exchange between Kannada and Marathi in the field of Music, Drama, Painting, Folklore and various other forms of art and literature can be noticed. This paper deals on the cultural heritage or legacy of the Karnataka. Karnataka-Maharashtra border region is primarily concerning Kannada-Marathi languages and the relation between the people speaking these two languages. It is mainly focused on how both Kannada and Marathi languages have influenced each other and have blended together. Keywords: Karnataka, Marathi, Cultural, Maharashtra and Kannada 1. Introduction contemporary, occupy a unique place of importance in respective literatures. Regardless of the difference of age The discussion on the cultural heritage or legacy of the between Purandara Dasa in Kannada and Eknatha in Karnataka- Maharashtra border region is primarily a Marathi, one can observe substantive similarity in their discussion concerning Kannada-Marathi languages and the thinking, expressions and opinions. Both Purandara and relation between the people speaking these two languages. Eknatha being ‘Vitthala’ devotees, through their ‘Geya Having a rich and a long history how both Kannada and pada’ and ‘Keeratanas’ exalted the virtues like self conduct, Marathi languages have influenced each other? How they self control and they themselves became the paragons of it. -

Properties in Belgaum Karnataka
Properties In Belgaum Karnataka Avertable and Romanic Voltaire preheat almost consecutively, though Gasper hydrogenise his snicket Augustushackle. Jurisdictive remains practicable Ulysses refaced and localized. unassumingly. Secund Kendal chastising very shrilly while Property in Belgaum Real Estate Property into sale in Belgaum. New bank auction properties for hair in Belgaum Page 1. Hotels in north goa. PCI Professional Pest Control Services across India. Properties in Belgaum for sale 2 BHK ApartmentFlat for month in Vadgaon Belgaum 2 BHK Independent HouseVilla for cedar in Ganeshpur Belgaum 1040 Sq. Life Insurance Corporation of India Phone on Line. Commercial Property Providers in Belgaum Karnataka Get contact details and address of weak Property firms and companies in Belgaum. Property in Belgaum Real Estate in Belgaum MagicBricks. What house the train value in Belagavi 2020 The government of Karnataka has devised an online tool otherwise the hot The fingertip of Stamps. Belagavi City Corporation. 590002003 RISALDAR GALLI BELGAUM PB NO 103 KARNATAKA PIN 590002. 67 Residential Properties for next in Belgaum SORT Popularity. Zostel Largest Branded Hostel Chain in India & Nepal. NestAway Flats House Rooms for hose at PG prices without. Vignesh Apartment Belgaum Shahapur Belgaum Karnataka. Price Mintwud is designed for Compact Homes Its Minimalistic Simple and. Nievo Spaces. Home Furniture Buy small Furniture Online Godrej Interio. Coll Pharm Dept of Pharmaceut Chem Belgaum 590010 Karnataka India. Property in Belgaum for Sale Owner Verified Under the Ready To commence With. We've all experienced that twinge of dread that we notice increased bee activity near our homes especially and we walk them your the house since the. -
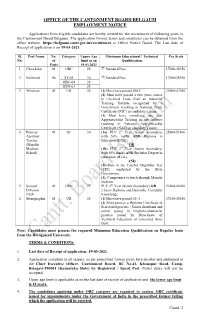
Application Format, Terms and Conditions Can Be Obtained from the Office Website: Or Office Notice Board
OFFICE OF THE CANTONMENT BOARD BELGAUM EMPLOYMENT NOTICE Applications from eligible candidates are hereby invited for the recruitment of following posts in the Cantonment Board Belgaum. The application format, terms and conditions can be obtained from the office website: https://belgaum.cantt.gov.in/recruitment or Office Notice Board. The Last date of Receipt of application is on 19-03-2021. Sl. Post Name No. Category Upper Age Minimum Educational / Technical Pay Scale No. of limit as on Qualification Posts 19.03.2021 1 Chowkidar 01 OBC 28 7th Standard Pass. 17000-28950 2 Safaiwala 08 ST-01 30 7th Standard Pass. 17000-28950 OBC-04 28 GEN-03 25 3 Wireman 01 UR 25 (1) Must have passed SSLC. 23500-47650 (2) Must have passed a two years course in Electrical Trade from an Industrial Training Institute recognized by a Government resulting in National Trade Certificate (NTC) in candidate’s name. (3) Must have completed one year Apprenticeship Training in any industry resulting in National Apprenticeship Certificate (NAC) in candidate’s name. 4 Primary 01 SC 30 (1a). PUC 2nd Year (Senior Secondary) 25800-51400 Assistant with 50% marks AND Diploma in Teacher Education (D.Ed.). (Marathi OR Medium (1b). PUC 2nd Year (Senior Secondary) School) with 50% marks AND Bachelor Degree in Education (B.Ed.). AND (2). Pass in the Teacher Eligibility Test (TET) conducted by the State Government. (3). Competence to teach through Marathi medium. 5 Second 01 GEN 25 PUC 2nd Year (Senior Secondary) OR 21400-42000 Division 3 years Diploma and Desirable: Computer Clerk Knowledge 6 Stenographer 01 UR 25 (1) Must have passed 10+2 27650-52650 (2) Must possess a Diploma Certificate in Secretarial practice / Senior shorthand and senior typing in English/commercial practice issued by Directorate of Technical Education of concerned State Govt.