An Analysis of Knowledge on and Responses to Climate Change Induced Health Hazards: the Case of Mt Darwin District in Zimbabwe B
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Ports of Entry and Routes) (Amendment) Order, 2020
Statutory Instrument 55 ofS.I. 2020. 55 of 2020 Customs and Excise (Ports of Entry and Routes) (Amendment) [CAP. 23:02 Order, 2020 (No. 20) Customs and Excise (Ports of Entry and Routes) (Amendment) “THIRTEENTH SCHEDULE Order, 2020 (No. 20) CUSTOMS DRY PORTS IT is hereby notifi ed that the Minister of Finance and Economic (a) Masvingo; Development has, in terms of sections 14 and 236 of the Customs (b) Bulawayo; and Excise Act [Chapter 23:02], made the following notice:— (c) Makuti; and 1. This notice may be cited as the Customs and Excise (Ports (d) Mutare. of Entry and Routes) (Amendment) Order, 2020 (No. 20). 2. Part I (Ports of Entry) of the Customs and Excise (Ports of Entry and Routes) Order, 2002, published in Statutory Instrument 14 of 2002, hereinafter called the Order, is amended as follows— (a) by the insertion of a new section 9A after section 9 to read as follows: “Customs dry ports 9A. (1) Customs dry ports are appointed at the places indicated in the Thirteenth Schedule for the collection of revenue, the report and clearance of goods imported or exported and matters incidental thereto and the general administration of the provisions of the Act. (2) The customs dry ports set up in terms of subsection (1) are also appointed as places where the Commissioner may establish bonded warehouses for the housing of uncleared goods. The bonded warehouses may be operated by persons authorised by the Commissioner in terms of the Act, and may store and also sell the bonded goods to the general public subject to the purchasers of the said goods paying the duty due and payable on the goods. -

Mozambique Zambia South Africa Zimbabwe Tanzania
UNITED NATIONS MOZAMBIQUE Geospatial 30°E 35°E 40°E L a k UNITED REPUBLIC OF 10°S e 10°S Chinsali M a l a w TANZANIA Palma i Mocimboa da Praia R ovuma Mueda ^! Lua Mecula pu la ZAMBIA L a Quissanga k e NIASSA N Metangula y CABO DELGADO a Chiconono DEM. REP. OF s a Ancuabe Pemba THE CONGO Lichinga Montepuez Marrupa Chipata MALAWI Maúa Lilongwe Namuno Namapa a ^! gw n Mandimba Memba a io u Vila úr L L Mecubúri Nacala Kabwe Gamito Cuamba Vila Ribáué MecontaMonapo Mossuril Fingoè FurancungoCoutinho ^! Nampula 15°S Vila ^! 15°S Lago de NAMPULA TETE Junqueiro ^! Lusaka ZumboCahora Bassa Murrupula Mogincual K Nametil o afu ezi Namarrói Erego e b Mágoè Tete GiléL am i Z Moatize Milange g Angoche Lugela o Z n l a h m a bez e i ZAMBEZIA Vila n azoe Changara da Moma n M a Lake Chemba Morrumbala Maganja Bindura Guro h Kariba Pebane C Namacurra e Chinhoyi Harare Vila Quelimane u ^! Fontes iq Marondera Mopeia Marromeu b am Inhaminga Velha oz P M úngu Chinde Be ni n è SOFALA t of ManicaChimoio o o o o o o o o o o o o o o o gh ZIMBABWE o Bi Mutare Sussundenga Dondo Gweru Masvingo Beira I NDI A N Bulawayo Chibabava 20°S 20°S Espungabera Nova OCE A N Mambone Gwanda MANICA e Sav Inhassôro Vilanculos Chicualacuala Mabote Mapai INHAMBANE Lim Massinga p o p GAZA o Morrumbene Homoíne Massingir Panda ^! National capital SOUTH Inhambane Administrative capital Polokwane Guijá Inharrime Town, village o Chibuto Major airport Magude MaciaManjacazeQuissico International boundary AFRICA Administrative boundary MAPUTO Xai-Xai 25°S Nelspruit Main road 25°S Moamba Manhiça Railway Pretoria MatolaMaputo ^! ^! 0 100 200km Mbabane^!Namaacha Boane 0 50 100mi !\ Bela Johannesburg Lobamba Vista ESWATINI Map No. -

Zimbabwean Government Gazette
A I SET ZIMBABWEAN GOVERNMENT GAZETTE Published by Authority Vol. LXXI, No. 44 2nd JULY. 1993 Price $2,50 i General Notice 384 of 1993. Zimbabwe United Passenger Company. ^^0/226/93. Permit: 15723. Motor-omnibus. Passenger-capacity: ROAD MOTOR TRANSPORTATION ACT [CHAPTER 262] Route 1: As d^ned in the agreonent between the holder and Applications in Connexion with Road Service Permits the Harare Municipality, approved by the Minister in terms of section 18 of the Road Motor Transportation Act [Chapter 262]. IN terms of subsection (4) of section 7 of the Road Motor Transportation Act [Chapter 262], notice is hereby given that Route 2:' Throu^out Zimbabwe. the applications detailed in the Sdiedule, for ue issue or Route 3: Harare - Darwendale - Banket - Chinhoyi - Aladta amendment of road service permits, have been received for the Compoimd - Sheckleton Mine - lions Den. consideration of the Controller of Road Motor Transportation. Condition: Any person wishing to object to any such application must Route 2: lodge with the Controller of Road Motor Transportation, (a) For private hire and for advertised or organized P.O. Box 8332, Causeway— tours, provided no stage carriage service is operated (a) a notice, in writing, of his intention to object, so as along any route. to reach the Controller’s ofiSce not later than the 23rd (b) No private Hire or any advertised or organized tour July, 1993; shall be operated under authority of this permit, (b) his objection and the grounds therefor, on form RAl.T. during ^e times for which a scheduled stage carriage 24, together with two copies tiiereof, so as to tetaxHa. -

The Spatial Dimension of Socio-Economic Development in Zimbabwe
THE SPATIAL DIMENSION OF SOCIO-ECONOMIC DEVELOPMENT IN ZIMBABWE by EVANS CHAZIRENI Submitted in fulfillment of the requirements for the degree of MASTER OF ARTS in the subject GEOGRAPHY at the UNIVERSITY OF SOUTH AFRICA SUPERVISOR: MRS AC HARMSE NOVEMBER 2003 1 Table of Contents List of figures 7 List of tables 8 Acknowledgements 10 Abstract 11 Chapter 1: Introduction, problem statement and method 1.1 Introduction 12 1.2 Statement of the problem 12 1.3 Objectives of the study 13 1.4 Geography and economic development 14 1.4.1 Economic geography 14 1.4.2 Paradigms in Economic Geography 16 1.4.3 Development paradigms 19 1.5 The spatial economy 21 1.5.1 Unequal development in space 22 1.5.2 The core-periphery model 22 1.5.3 Development strategies 23 1.6 Research design and methodology 26 1.6.1 Objectives of the research 26 1.6.2 Research method 27 1.6.3 Study area 27 1.6.4 Time period 30 1.6.5 Data gathering 30 1.6.6 Data analysis 31 1.7 Organisation of the thesis 32 2 Chapter 2: Spatial Economic development: Theory, Policy and practice 2.1 Introduction 34 2.2. Spatial economic development 34 2.3. Models of spatial economic development 36 2.3.1. The core-periphery model 37 2.3.2 Model of development regions 39 2.3.2.1 Core region 41 2.3.2.2 Upward transitional region 41 2.3.2.3 Resource frontier region 42 2.3.2.4 Downward transitional regions 43 2.3.2.5 Special problem region 44 2.3.3 Application of the model of development regions 44 2.3.3.1 Application of the model in Venezuela 44 2.3.3.2 Application of the model in South Africa 46 2.3.3.3 Application of the model in Swaziland 49 2.4. -

PLAAS RR46 Smeadzim 1.Pdf
Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Faculty of Economic and Management Sciences Research Report 46 Space, Markets and Employment in Agricultural Development: Zimbabwe Country Report Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Published by the Institute for Poverty, Land and Agrarian Studies, Faculty of Economic and Management Sciences, University of the Western Cape, Private Bag X17, Bellville 7535, Cape Town, South Africa Tel: +27 21 959 3733 Fax: +27 21 959 3732 Email: [email protected] Institute for Poverty, Land and Agrarian Studies Research Report no. 46 June 2015 All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means without prior permission from the publisher or the authors. Copy Editor: Vaun Cornell Series Editor: Rebecca Pointer Photographs: Pamela Ngwenya Typeset in Frutiger Thanks to the UK’s Department for International Development (DfID) and the Economic and Social Research Council’s (ESRC) Growth Research Programme Contents List of tables ................................................................................................................ ii List of figures .............................................................................................................. iii Acronyms and abbreviations ...................................................................................... v 1 Introduction ........................................................................................................ -

Promotion of Climate-Resilient Lifestyles Among Rural Families in Gutu
Promotion of climate-resilient lifestyles among rural families in Gutu (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts | Zimbabwe Sahara and Sahel Observatory 26 November 2019 Promotion of climate-resilient lifestyles among rural families in Gutu Project/Programme title: (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts Country(ies): Zimbabwe National Designated Climate Change Management Department, Ministry of Authority(ies) (NDA): Environment, Water and Climate Development Aid from People to People in Zimbabwe (DAPP Executing Entities: Zimbabwe) Accredited Entity(ies) (AE): Sahara and Sahel Observatory Date of first submission/ 7/19/2019 V.1 version number: Date of current submission/ 11/26/2019 V.2 version number A. Project / Programme Information (max. 1 page) ☒ Project ☒ Public sector A.2. Public or A.1. Project or programme A.3 RFP Not applicable private sector ☐ Programme ☐ Private sector Mitigation: Reduced emissions from: ☐ Energy access and power generation: 0% ☐ Low emission transport: 0% ☐ Buildings, cities and industries and appliances: 0% A.4. Indicate the result ☒ Forestry and land use: 25% areas for the project/programme Adaptation: Increased resilience of: ☒ Most vulnerable people and communities: 25% ☒ Health and well-being, and food and water security: 25% ☐ Infrastructure and built environment: 0% ☒ Ecosystem and ecosystem services: 25% A.5.1. Estimated mitigation impact 399,223 tCO2eq (tCO2eq over project lifespan) A.5.2. Estimated adaptation impact 12,000 direct beneficiaries (number of direct beneficiaries) A.5. Impact potential A.5.3. Estimated adaptation impact 40,000 indirect beneficiaries (number of indirect beneficiaries) A.5.4. Estimated adaptation impact 0.28% of the country’s total population (% of total population) A.6. -
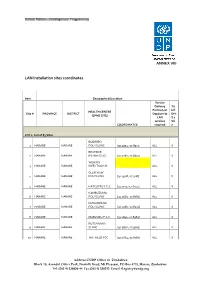
LAN Installation Sites Coordinates
ANNEX VIII LAN Installation sites coordinates Item Geographical/Location Service Delivery Tic Points (List k if HEALTH CENTRE Site # PROVINCE DISTRICT Dept/umits DHI (EPMS SITE) LAN S 2 services Sit COORDINATES required e LOT 1: List of 83 Sites BUDIRIRO 1 HARARE HARARE POLYCLINIC [30.9354,-17.8912] ALL X BEATRICE 2 HARARE HARARE RD.INFECTIO [31.0282,-17.8601] ALL X WILKINS 3 HARARE HARARE INFECTIOUS H ALL X GLEN VIEW 4 HARARE HARARE POLYCLINIC [30.9508,-17.908] ALL X 5 HARARE HARARE HATCLIFFE P.C.C. [31.1075,-17.6974] ALL X KAMBUZUMA 6 HARARE HARARE POLYCLINIC [30.9683,-17.8581] ALL X KUWADZANA 7 HARARE HARARE POLYCLINIC [30.9285,-17.8323] ALL X 8 HARARE HARARE MABVUKU P.C.C. [31.1841,-17.8389] ALL X RUTSANANA 9 HARARE HARARE CLINIC [30.9861,-17.9065] ALL X 10 HARARE HARARE HATFIELD PCC [31.0864,-17.8787] ALL X Address UNDP Office in Zimbabwe Block 10, Arundel Office Park, Norfolk Road, Mt Pleasant, PO Box 4775, Harare, Zimbabwe Tel: (263 4) 338836-44 Fax:(263 4) 338292 Email: [email protected] NEWLANDS 11 HARARE HARARE CLINIC ALL X SEKE SOUTH 12 HARARE CHITUNGWIZA CLINIC [31.0763,-18.0314] ALL X SEKE NORTH 13 HARARE CHITUNGWIZA CLINIC [31.0943,-18.0152] ALL X 14 HARARE CHITUNGWIZA ST.MARYS CLINIC [31.0427,-17.9947] ALL X 15 HARARE CHITUNGWIZA ZENGEZA CLINIC [31.0582,-18.0066] ALL X CHITUNGWIZA CENTRAL 16 HARARE CHITUNGWIZA HOSPITAL [31.0628,-18.0176] ALL X HARARE CENTRAL 17 HARARE HARARE HOSPITAL [31.0128,-17.8609] ALL X PARIRENYATWA CENTRAL 18 HARARE HARARE HOSPITAL [30.0433,-17.8122] ALL X MURAMBINDA [31.65555953980,- 19 MANICALAND -

Midlands Province
School Province District School Name School Address Level Primary Midlands Chirumanzu BARU KUSHINGA PRIMARY BARU KUSHINGA VILLAGE 48 CENTAL ESTATES Primary Midlands Chirumanzu BUSH PARK MUSENA RESETTLEMENT AREA VILLAGE 1 MUSENA Primary Midlands Chirumanzu BUSH PARK 2 VILLAGE 5 WARD 19 CHIRUMANZU Primary Midlands Chirumanzu CAMBRAI ST MATHIAS LALAPANZI TOWNSHIP CHIRUMANZU Primary Midlands Chirumanzu CHAKA NDARUZA VILLAGE HEAD CHAKA Primary Midlands Chirumanzu CHAKASTEAD FENALI VILLAGE NYOMBI SIDING Primary Midlands Chirumanzu CHAMAKANDA TAKAWIRA RESETTLEMENT SCHEME MVUMA Primary Midlands Chirumanzu CHAPWANYA HWATA-HOLYCROSS ROAD RUDUMA VILLAGE Primary Midlands Chirumanzu CHIHOSHO MATARITANO VILLAGE HEADMAN DEBWE Primary Midlands Chirumanzu CHILIMANZI NYONGA VILLAGE CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHIMBINDI CHIMBINDI VILLAGE WARD 5 CHIRUMANZU Primary Midlands Chirumanzu CHINGEGOMO WARD 18 TOKWE 4 VILLAGE 16 CHIRUMANZU Primary Midlands Chirumanzu CHINYUNI CHINYUNI WARD 7 CHUKUCHA VILLAGE Primary Midlands Chirumanzu CHIRAYA (WYLDERGROOVE) MVUMA HARARE ROAD WASR 20 VILLAGE 1 Primary Midlands Chirumanzu CHISHUKU CHISHUKU VILAGE 3 CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHITENDERANO TAKAWIRA RESETTLEMENT AREA WARD 11 Primary Midlands Chirumanzu CHIWESHE PONDIWA VILLAGE MAPIRAVANA Primary Midlands Chirumanzu CHIWODZA CHIWODZA RESETTLEMENT AREA Primary Midlands Chirumanzu CHIWODZA NO 2 VILLAGE 66 CHIWODZA CENTRAL ESTATES Primary Midlands Chirumanzu CHIZVINIRE CHIZVINIRE PRIMARY SCHOOL RAMBANAPASI VILLAGE WARD 4 Primary Midlands -

Faculty of Arts Department of History And
FACULTY OF ARTS DEPARTMENT OF HISTORY AND INTERNATIONAL STUDIES RESOURCE NATIONALISM AND LOCAL EMPOWERMENT, THE CASE OF ZVISHAVANE COMMUNITY SHARE OWNERSIP TRUST, 2012 TO 2017. By FAITH MAFUNGA R147013M SUPERVISOR: DR T. MASHINGAIDZE A DISSERTATION SUBMITTED TO THE HISTORY DEPARTMENT OF THE MIDLANDS STATE UNIVERSITY IN PARTIAL FULFILMENT OF THE REQUIREMENTS OF THE BACHELOR OF ARTS IN HISTORY AND INTERNATIONAL STUDIES HONOURS DEGREE. ZVISHAVANE, ZIMBABWE JUNE 2018 Declaration I, Faith Mafunga declare that this dissertation hereby submitted for the Bachelor of Arts Honors Degree in History and International Studies at Midlands State University is my own effort. Information from published and unpublished work from other authors have been acknowledged. …………………………. ……………………………… Student Date i Approval form The undersigned certify that they have supervised and recommended to Midlands State University the student FAITH MAFUNGA dissertation entitled RESOURCE NATIONALISM AND LOCAL EMPOWERMENT, THE CASEOF ZVISHAVANE COMMUNITY SHARE OWNERSIP TRUST, 2012 TO 2017. The dissertation submitted in partial fulfillment of the requirements for the History and International Studies Department. …………………………. ……………………………… Supervisor Date …………………………… …………………………………. Chairperson Date …………………………. ……………………………………… External Examiner Date ii Dedication This piece of work is dedicated to my late father Mr. E.C Mafunga, my mother Mrs. E Mauto, my siblings Yvonne, Tanaka and Tafadzwa Mafunga. Thank you all for your constant love and support. God Bless you. iii Acknowledgements Utmost gratitude goes to God Almighty for he has been an unwavering source of strength throughout my academic years. I must pay tribute to my academic supervisor Doctor Mashingaidze who has given me supervision and motivation throughout this research. My exceptional gratefulness also goes to Mr. N.T Jinga the C.E.O of ZCSOT and the entire organization for helping me in crafting this dissertation. -

Grant Assistance for Grassroots Human Projects in Zimbabwe
Grant Assistance for Grassroots Human Projects in Zimbabwe Amount Amount No Year Project Title Implementing Organisation District (US) (yen) 1 1989 Mbungu Primary School Development Project Mbungu Primary School Gokwe 16,807 2,067,261 2 1989 Sewing and Knitting Project Rutowa Young Women's Club Gutu 5,434 668,382 3 1990 Children's Agricultural Project Save the Children USA Nyangombe 8,659 1,177,624 Mbungo Uniform Clothing Tailoring Workshop 4 1990 Mbungo Women's Club Masvingo 14,767 2,008,312 Project Construction of Gardening Facilities in 5 1991 Cold Comfort Farm Trust Harare 42,103 5,431,287 Support of Small-Scale Farmers 6 1991 Pre-School Project Kwayedza Cooperative Gweru 33,226 4,286,154 Committee for the Rural Technical 7 1992 Rural Technical Training Project Murehwa 38,266 4,936,314 Training Project 8 1992 Mukotosi Schools Project Mukotosi Project Committee Chivi 20,912 2,697,648 9 1992 Bvute Dam Project Bvute Dam Project Committee Chivi 3,558 458,982 10 1992 Uranda Clinic Project Uranda Clinic Project Committee Chivi 1,309 168,861 11 1992 Utete Dam Project Utete Dam Project Committee Chivi 8,051 1,038,579 Drilling of Ten Boreholes for Water and 12 1993 Irrigation in the Inyathi and Tsholotsho Help Age Zimbabwe Tsholotsho 41,574 5,072,028 PromotionDistricts of ofSocialForestry Matabeleland andManagement Zimbabwe National Conservation 13 1993 Buhera 46,682 5,695,204 ofWoodlands inCommunalAreas ofZimbabwe Trust Expansion of St. Mary's Gavhunga Primary St. Mary's Gavhunga Primary 14 1994 Kadoma 29,916 3,171,096 School School Tsitshatshawa -

For Human Dignity
ZIMBABWE HUMAN RIGHTS COMMISSION For Human Dignity REPORT ON: APRIL 2020 i DISTRIBUTED BY VERITAS e-mail: [email protected]; website: www.veritaszim.net Veritas makes every effort to ensure the provision of reliable information, but cannot take legal responsibility for information supplied. NATIONAL INQUIRY REPORT NATIONAL INQUIRY REPORT ZIMBABWE HUMAN RIGHTS COMMISSION ZIMBABWE HUMAN RIGHTS COMMISSION For Human Dignity For Human Dignity TABLE OF CONTENTS FOREWORD .................................................................................................................................................. vii ACRONYMS.................................................................................................................................................... ix GLOSSARY OF TERMS .................................................................................................................................. xi PART A: INTRODUCTION TO THE NATIONAL INQUIRY PROCESS ................................................................ 1 CHAPTER 1: INTRODUCTION ........................................................................................................................ 1 1.1 Establishment of the National Inquiry and its Terms of Reference ....................................................... 2 1.2 Methodology ..................................................................................................................................... 3 CHAPTER 2: THE NATIONAL INQUIRY PROCESS ......................................................................................... -

Small Grain Production As an Adaptive Strategy to Climate Change in Mangwe District, Matabeleland South in Zimbabwe
Jàmbá - Journal of Disaster Risk Studies ISSN: (Online) 2072-845X, (Print) 1996-1421 Page 1 of 9 Original Research Small grain production as an adaptive strategy to climate change in Mangwe District, Matabeleland South in Zimbabwe Authors: This article assesses the feasibility of small grains as an adaptive strategy to climate change in 1 Tapiwa Muzerengi the Mangwe District in Zimbabwe. The change in climate has drastically affected rainfall Happy M. Tirivangasi2 patterns across the globe and in Zimbabwe in particular. Continuous prevalence of droughts Affiliations: in Zimbabwe, coupled with other economic calamities facing the Southern African country, 1Department of Community has contributed to a larger extent to the reduction in grain production among communal Development, University of farmers, most of whom are in semi-arid areas. This has caused a sudden increase in food KwaZulu-Natal, Durban, South Africa shortages, particularly in the Mangwe District, as a result of erratic rainfall, which has negatively affected subsistence farming. This article was deeply rooted in qualitative research 2Department of Sociology methodologies. Purposive sampling was used to sample the population. The researchers used and Anthropology, University key informant interviews, focus group discussions and secondary data to collect data. Data of Limpopo, Sovenga, South were analysed using INVIVO software, a data analysis tool that brings out themes. The results Africa of the study are presented in the form of themes. The study established that small grains Corresponding author: contributed significantly to addressing food shortages in the Mangwe District. The study Happy Tirivangasi, results revealed that small grains were a reliable adaptive strategy to climate change as they [email protected] increased food availability, accessibility, utilisation and stability.