Acute Bronchitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Caring for Children with Special Needs ALLERGIES and ASTHMA
caring for children with special needs ALLERGIES AND ASTHMA We don’t usually think of children with allergies or asthma as children with “special needs,” but they certainly are. In fact, children with these conditions are probably the most frequently encountered “special needs” children. Child care providers can do a great deal to help individual children manage their specific allergy or asthma needs and feel more comfortable in a child care setting. Allergies wastes. Every house has them, no matter how clean. Other inhaled Children with allergies face the allergens include mold, pollen (hay same social difficulties as do adults, fever), animal dander (especially but they have less maturity and from cats), chemicals, and per emotional resources to deal with fumes. them. Children find that they cannot eat what their friends eat or The most common allergy symp cannot play outside during some toms are seasons. Until a child is mature � a clear, runny nose and enough to understand why she sneezing, cannot do something, you must be � itchy or stuffed-up nose or careful to help the child through the itchy, runny eyes, and difficulties. Start teaching a child early on about what he is allergic to; � asthma (remember that not all you will not always be able to people with asthma have monitor everything. allergies and not all allergies Some foods can cause a life cause or develop into asthma). threatening reaction. The mouth, throat, and bronchial tubes swell enough to interfere with breathing. Strategies for inclusion The person may wheeze or faint. Some parents have found that by Often there are generalized hives volunteering to bring food to and/or a swollen face. -

Allergic Bronchopulmonary Aspergillosis Revealing Asthma
CASE REPORT published: 22 June 2021 doi: 10.3389/fimmu.2021.695954 Case Report: Allergic Bronchopulmonary Aspergillosis Revealing Asthma Houda Snen 1,2*, Aicha Kallel 2,3*, Hana Blibech 1,2, Sana Jemel 2,3, Nozha Ben Salah 1,2, Sonia Marouen 3, Nadia Mehiri 1,2, Slah Belhaj 3, Bechir Louzir 1,2 and Kalthoum Kallel 2,3 1 Pulmonary Department, Hospital Mongi Slim, La Marsa, Tunisia, 2 Faculty of Medicine, Tunis El Manar University, Tunis, Tunisia, 3 Parasitology and Mycology Department, La Rabta Hospital, Tunis, Tunisia Allergic bronchopulmonary aspergillosis (ABPA) is an immunological pulmonary disorder caused by hypersensitivity to Aspergillus which colonizes the airways of patients with asthma and cystic fibrosis. Its diagnosis could be difficult in some cases due to atypical Edited by: presentations especially when there is no medical history of asthma. Treatment of ABPA is Brian Stephen Eley, frequently associated to side effects but cumulated drug toxicity due to different molecules University of Cape Town, South Africa is rarely reported. An accurate choice among the different available molecules and Reviewed by: effective on ABPA is crucial. We report a case of ABPA in a woman without a known Shivank Singh, Southern Medical University, China history of asthma. She presented an acute bronchitis with wheezing dyspnea leading to an Richard B. Moss, acute respiratory failure. She was hospitalized in the intensive care unit. The Stanford University, United States bronchoscopy revealed a complete obstruction of the left primary bronchus by a sticky *Correspondence: Houda Snen greenish material. The culture of this material isolated Aspergillus fumigatus and that of [email protected] bronchial aspiration fluid isolated Pseudomonas aeruginosa. -

Symptoms Related to Asthma and Chronic Bronchitis in Three Areas of Sweden
Eur Respir J, 1994, 7, 2146–2153 Copyright ERS Journals Ltd 1994 DOI: 10.1183/09031936.94.07122146 European Respiratory Journal Printed in UK - all rights reserved ISSN 0903 - 1936 Symptoms related to asthma and chronic bronchitis in three areas of Sweden E. Björnsson*, P. Plaschke**, E. Norrman+, C. Janson*, B. Lundbäck+, A. Rosenhall+, N. Lindholm**, L. Rosenhall+, E. Berglund++, G. Boman* Symptoms related to asthma and chronic bronchitis in three areas of Sweden. E. Björnsson, *Dept of Lung Medicine and Asthma P. Plaschke, E. Norrman, C. Janson, B. Lundbäck, A. Rosenhall, N. Lindholm, L. Research Center, Akademiska sjukhu- Rosenhall, E. Berglund, G. Boman. ERS Journals Ltd 1994. set, Uppsala University, Uppsala, Sweden. ABSTRACT: Does the prevalence of respiratory symptoms differ between regions? **Asthma and Allergy Research Center, Sahlgren's Hospital, University of Göteborg, As a part of the European Community Respiratory Health Survey, we present data Göteborg, Sweden. +Dept of Pulmonary from an international questionnaire on asthma symptoms occurring during a 12 Medicine and Allergology, Univer- month period, smoking and symptoms of chronic bronchitis. The questionnaire was sity Hospital of Northern Sweden, Umeå, mailed to 10,800 persons aged 20–44 yrs living in three regions of Sweden (Västerbotten, Sweden. ++Dept of Pulmonary Medicine, Uppsala and Göteborg) with different environmental characteristics. The total Sahlgrenska University Hospital, Göteborg, response rate was 86%. Sweden. Wheezing was reported by 20.5%, and the combination of wheezing without a Correspondence: E. Björnsson, Dept of cold and wheezing with breathlessness by 7.4%. The use of asthma medication was Lung Medicine, Akademiska sjukhuset, S- reported by 5.3%. -

Keeping Your Gut in Check Healthy Options to Stay on Tract Your Digestive System Is Busy
May 2017 National Institutes of Health • Department of Health and Human Services • newsinhealth.nih.gov Inside News: 3 Bronchitis vs. Pneumonia... 4 Eating Habits and Disease... Spanish Health Materials... Human Genome Keeping Your Gut in Check Healthy Options to Stay on Tract Your digestive system is busy. What you eat can help or When you eat something, your hurt your digestive system, and food takes a twisty trip that influence how you feel. “Increas- starts with being chewed up ing fiber is really important for and ends with you going to constipation,” says Chang. “Most the bathroom. A lot happens in Americans do not eat a lot of between. The health of your gut fiber so you have to gradually plays a key role in your overall increase the fiber in your diet. health and well-being. You can Otherwise you might get gas make choices to help your body and more bloating, and won’t stay on tract. stick with [the changes].” Your digestive, or Chang says you should eat at gastrointestinal (GI), tract is a least 20–30 grams of fiber a day long, muscular tube that runs for constipation. You can spread from your mouth to your anus. out your fiber in small amounts It’s about 30 feet long and throughout the day. Start with works with other parts of your small servings and gradually digestive system to break food increase them to avoid gas, and drink down into smaller bloating, and discomfort. molecules of nutrients. The Try to eat fruits and vege- blood absorbs these and carries them Chang, a GI expert at the University tables at every meal. -
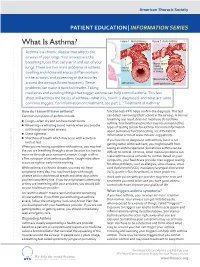
What Is Asthma? Figure 1
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES What Is Asthma? Figure 1. Normal Airway Figure 2. Acute Asthma Asthma is a chronic disease that affects the airways of your lungs. Your airways are the breathing tubes that carry air in and out of your Muscle spasm causing lungs. There are two main problems in asthma: relaxed narrowing muscles swelling and increased mucus (inflammation) of airways in the airways, and squeezing of the muscles Mucus build up around the airways (bronchospasm). These open airways Swelling/inammation problems can make it hard to breathe. Taking medicines and avoiding things that trigger asthma can help control asthma. This fact sheet will address the basics of asthma—what it is, how it is diagnosed, and what are some common triggers. For information on treatment, see part 2, “Treatment of Asthma”. How do I know if I have asthma? function test–PFT) helps confirm the diagnosis. This test Common symptoms of asthma include: can detect narrowing (obstruction) in the airways. A normal breathing test result does not mean you do not have ■ Cough—often dry and can have harsh bursts asthma. Your healthcare provider may recommend other ■ Wheezing—a whistling sound mainly when you breathe types of testing to look for asthma. For more information out through narrowed airways about pulmonary function testing, see ATS Patient ■ Chest tightness Information series at www.thoracic.org/patients. ■ Shortness of breath which may occur with activity or If you have been diagnosed with asthma, but it is not even at rest getting better with treatment, you might benefit from When you are having a problem with asthma, you may feel CLIP AND COPY AND CLIP seeing an asthma specialist. -

Acute (Serious) Bronchitis
Acute (serious) Bronchitis This is an infection of the air tubes that go down to your lungs. It often follows a cold or the flu. Most people do not need treatment for this. The infection normally goes away in 7-10 days. We make every effort to make sure the information is correct (right). However, we cannot be responsible for any actions as a result of using this information. Getting Acute Bronchitis How the lungs work Your lungs are like two large sponges filled with tubes. As you breathe in, you suck oxygen through your nose and mouth into a tube in your neck. Bacteria and viruses in the air can travel into your lungs. Normally, this does not cause a problem as your body kills the bacteria, or viruses. However, sometimes infection can get through. If you smoke or if you have had another illness, infections are more likely to get through. Acute Bronchitis Acute bronchitis is when the large airways (breathing tubes) to the lungs get inflamed (swollen and sore). The infection makes the airways swell and you get a build up of phlegm (thick mucus). Coughing is a way of getting the phlegm out of your airways. The cough can sometimes last for up to 3 weeks. Acute Bronchitis usually goes away on its own and does not need treatment. We make every effort to make sure the information is correct (right). However, we cannot be responsible for any actions as a result of using this information. Symptoms (feelings that show you may have the illness) Symptoms of Acute Bronchitis include: • A chesty cough • Coughing up mucus, which is usually yellow, or green • Breathlessness when doing more energetic activities • Wheeziness • Dry mouth • High temperature • Headache • Loss of appetite The cough usually lasts between 7-10 days. -

Octreotide Treatment of Idiopathic Pulmonary Fibrosis: a Proof-Of-Concept Study
drugs, while two patients underwent surgery in addition to Roncaccio 16, 21049, Tradate, Italy. E-mail: giovannibattista. chemotherapy. [email protected] As in other reference centres, the E. Morelli Hospital needs to transfer out all admitted cases to the hospitals referring them for Support Statement: This study was supported by the current specialised treatment, when culture conversion and clinical research funds of the participating institutions. For this stability have been achieved. Patients were transferred out after publication, the research leading to these results has received a median (IQR) hospital stay of 75.5 (51.5–127.5) days; 12 (100%) funding from the European Community’s Seventh Framework out of 12 and nine (75%) out of 12 achieved sputum-smear and Programme (FP7/2007-2013) under grant agreement FP7- culture conversion, after a median (IQR) time of 40.5 (24–64) and 223681. 70 (44–95) days, respectively. As of June 2011, one patient was cured, two had died and nine were still under treatment. Statement of Interest: None declared. Four (33.3%) cases reported adverse events, two being major (16.7%; neuropathy and low platelet count, needing temporary REFERENCES interruption of linezolid) and two minor (neuropathy and mild 1 Villar M, Sotgiu G, D’Ambrosio L, et al. Linezolid safety, anaemia). All adverse events were reversible. tolerability and efficacy to treat multidrug- and extensively drug-resistant tuberculosis. Eur Respir J 2011; 38: 730–733. In conclusion, despite the intrinsic difficulty of evaluating the 2 World Health Organization. Multidrug and extensively drug safety and tolerability of linezolid (administered within different resistant TB (M/XDR-TB): 2010 global report on surveillance and regimens including multiple anti-TB drugs guided by drug response. -

Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation
Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation Dr Rohit Bazaz National Aspergillosis Centre, UK Manchester University NHS Foundation Trust/University of Manchester ~ ABPA -a41'1 Severe asthma wl'th funga I Siens itisat i on Subacute IA Chronic pulmonary aspergillosjs Simp 1Ie a:spe rgmoma As r§i · bronchitis I ram une dysfu net Ion Lun· damage Immu11e hypce ractivitv Figure 1 In t@rarctfo n of Aspergillus Vliith host. ABP A, aHerg tc broncho pu~ mo na my as µe rgi ~fos lis; IA, i nvas we as ?@rgiH os 5. MANCHl·.'>I ER J:-\2 I Kosmidis, Denning . Thorax 2015;70:270–277. doi:10.1136/thoraxjnl-2014-206291 Allergic Fungal Airway Disease Phenotypes I[ Asthma AAFS SAFS ABPA-S AAFS-asthma associated with fu ngaIsensitization SAFS-severe asthma with funga l sensitization ABPA-S-seropositive a llergic bronchopulmonary aspergi ll osis AB PA-CB-all ergic bronchopulmonary aspergi ll osis with central bronchiectasis Agarwal R, CurrAlfergy Asthma Rep 2011;11:403 Woolnough K et a l, Curr Opin Pulm Med 2015;21:39 9 Stanford Lucile Packard ~ Children's. Health Children's. Hospital CJ Scanford l MEDICINE Stanford MANCHl·.'>I ER J:-\2 I Aspergi 11 us Sensitisation • Skin testing/specific lgE • Surface hydroph,obins - RodA • 30% of patients with asthma • 13% p.atients with COPD • 65% patients with CF MANCHl·.'>I ER J:-\2 I Alternar1a• ABPA •· .ABPA is an exagg·erated response ofthe imm1une system1 to AspergUlus • Com1pUcatio n of asthm1a and cystic f ibrosis (rarell·y TH2 driven COPD o r no identif ied p1 rior resp1 iratory d isease) • ABPA as a comp1 Ucation of asth ma affects around 2.5% of adullts. -

Influenza (PDF)
INFLUENZA Outbreaks of influenza, or “flu”, typically occur every winter. Colds may occur at any time of year with seasonal peaks occurring in fall and spring. Influenza is a respiratory illness usually caused by infection with one of two influenza viruses – influenza A or influenza B. Outbreaks of influenza (flu) typically occur every winter. Influenza is characterized by an abrupt onset of fever, chills, headache, body aches, and lack of energy accompanied by respiratory symptoms, most frequently cough and sore throat. Most people are largely recovered in one week, although many feel fatigued for several weeks. Serious complications of flu, such as pneumonia, however, can occur, especially if the body’s defenses are weakened by age or disease. Influenza is spread by inhaling the influenza virus which is usually carried on tiny, invisible water droplets in the air generated by coughs and sneezes. Hand-to-hand contact as well as contact with infected secretions on a hard surface may also cause transmission of the virus. Each year influenza viruses change and new vaccines are made to combat the particular strains that are expected to cause illness that year. The flu vaccine may reduce the chance of getting the flu by 60-80%, and lessen the severity of illness in the person who does get the flu. According to the Centers for Disease Control (CDC), everyone 6 months or order should get a yearly flu vaccine. The following people are at high risk for complications of flu and are especially urged to get vaccinated: Individuals with chronic heart or lung problems that have required regular medical follow-up or hospitalization during the last year. -

Obliterative Bronchiolitis, Cryptogenic Organising Pneumonitis and Bronchiolitis Obliterans Organizing Pneumonia: Three Names for Two Different Conditions
Eur Reaplr J EDITORIAL 1991, 4, 774-775 Obliterative bronchiolitis, cryptogenic organising pneumonitis and bronchiolitis obliterans organizing pneumonia: three names for two different conditions R.M. du Bois, O.M. Geddes Over the last five years, increasing confusion has has been applied to conditions in which airflow obstruc developed over the use of the terms "bronchiolitis tion is prominent and in which response to treatment is obliterans" and "bronchiolitis obliterans organizing poor. pneumonia". The confusion stems largely from the common use of the term "bronchiolitis obliterans" or "obliterative bronchiolitis" in the diagnostic labels applied "Cryptogenic organizing pneumonitis" or "bronchi· to two entities which are quite distinct clinically but which otitis obliterans organizing pneumonia" (BOOP) bear certain resemblances histologically. Cryptogenic organizing pneumonitis was first described by DAVISON et al. [7] in 1983. The clinical syndrome ObUterative bronchiolitis consisted of breathlessness, malaise, fever, high erythrocyte sedimentation rate (ESR), pneumonic In 1977, GEODES et al. [1] reported the case histories shadowing on chest radiograph with a restrictive of six patients whose clinical condition was characterized pulmonary function defect and low gas transfer coeffi by airways obliteration in association with rheumatoid cient. On histological examination of lung biopsy mate· arthritis. The striking clinical features were of rapidly rial, the typical and distinguishing feature was the progressive breathlessness and the fmding on examination presence of connective tissue within the alveoli, alveolar of a high-pitched mid-inspiratory squeak heard over the ducts and, occasionally, in respiratory bronchioles. This lung fields. Chest radiographs showed hyperinflated lungs connective tissue consisted of "loosely woven fibres of but were otherwise normal. -

Diseases of the Respiratory System (J00-J99) ICD-10-CM
Diseases of the Respiratory System (J00-J99) ICD-10-CM Coverage provided by Amerigroup Inc. This publication contains proprietary information. This material is for informational purposes only. Reference the Centers for Medicare and Medicaid Services (CMS) for more information on Risk Adjustment and the CMS-HCC Model. Redistribution or other use is strictly forbidden This publication is for informational purposes only and is not guaranteed to be without defect. Please reference the current version(s) of the ICD-10-CM codebook, CMS-HCC Risk Adjustment Model, and AHA Coding Clinic for complete code sets and official coding guidance. AGPCARE-0080-19 63321MUPENABS 10/05/16 Diseases of the respiratory system are located in chapter Intermittent asthma which is defined as less 10 of the ICD-10-CM code book; this chapter includes than or equal to two occurrences per week. conditions such as asthma, pneumonia, and chronic Persistent asthma which includes three levels obstructive pulmonary disease (COPD). of severity: Mild: more than two times per week Reporting respiratory conditions Moderate: daily and may restrict Codes for reporting diseases of the respiratory physical activity system in ICD-10-CM feature relatively minor Severe: throughout the day with changes from ICD-9-CM. Most of the changes recurrent severe attacks limiting the involve understanding the medical terminology that ability to breathe the more specific codes include, as well as, the new The fourth character indicates severity, and the general coding structure and rules. fifth identifies whether status asthmaticus or At the beginning of chapter 10 for “Diseases of exacerbation is present. the Respiratory System (J00-J99),” an instructional note states, “When a respiratory condition is Asthma ICD-10-CM description described as occurring in more than one site and Category J45 Asthma is not specifically indexed, it should be classified Includes: to the lower anatomic site.” For example, Allergic: tracheobronchitis is classified to bronchitis with Asthma code J40. -

COPD (Chronic Obstructive Pulmonary Disease)
COPD (Chronic Obstructive Pulmonary Disease) A difficult problem explained in simple language. Introduction The normal lung Lung facts What is COPD? How does COPD damage your health? How can I tell if I am developing COPD? How can we tell if you are developing COPD? What can you do to help yourself? What can we do to help you? Conclusion INTRODUCTION So you want to find out more about the illness that we call COPD. It may be that your doctor has raised some concerns that you might have this condition but has not had a chance to explain what it is. You may have seen something in the press about COPD which describes symptoms that you have been getting such as cough, phlegm and breathlessness or you may have a loved one who is developing these symptoms and you are concerned to find out what the cause is. Make sure you read all the way through to the end of this description and we hope that you will have a much better understanding. The normal lung. As we travel through the voice box (larynx) into the main windpipe (trachea) we find the airways that we pass through get smaller and smaller with increasing numbers of branches until the tiniest tubes open into bubbles whose walls consist of a very fine membrane. These bubbles are arranged in bunches like grapes around which is a lace work of very fine blood vessels. In the healthy lung, when air reaches these bubbles (alveoli), oxygen passes readily through the bubble membrane into the blood stream.