Development of Pandemic Vaccines: ERVEBO Case Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The 1947 Smallpox Vaccination Campaign in New York City, Revisited
LETTERS The 1947 Smallpox Two days later, epidemiologic contrast, the Army and Navy had investigation indicated that all given almost 800,000 doses, and the Vaccination patients with diagnosed cases were city’s public health laboratories had Campaign in New related and that, in all likelihood, the made the remaining 400,000. York City, Revisited outbreak had been successfully halted During the shortage, the Times through tracing the movements of the noted, “hundreds of eager men, To the Editor: In 1947, millions of various patients and vaccinating any- women, and children queued up at New Yorkers received smallpox vacci- one who had contact with them, so- Bellevue Hospital at dawn, although nations, an accomplishment still appro- called “ring” vaccination (4). Despite vaccinations were not scheduled to priately held up as an example of pub- this halt of the outbreak, the city begin until 10 a.m. At some stations, lic health planning and mobilization. pushed forward. The campaign to “Be the crowds did not take kindly to the Although now mythological, a review sure, be safe, get vaccinated!” had news that the doctors had run out of of the events of April 1947, from proven successful. By city estimate, vaccine and the police had a little dif- copies of The New York Times (1–9), >600,000 persons had received vac- ficulty dispersing a crowd of several tells of a more recognizably human cine in the first week. hundred” outside one vaccine station response: pushing, jawing, deceit, Vaccine side effects, which domi- (5). shortages, surpluses, and perhaps a nate coverage of today’s vaccination On April 17, the situation bright- unusual way of counting vaccinees. -

Evidence Assessment STRATEGIC ADVISORY GROUP of EXPERTS (SAGE) on IMMUNIZATION Meeting 15 March 2021
Evidence Assessment STRATEGIC ADVISORY GROUP OF EXPERTS (SAGE) ON IMMUNIZATION Meeting 15 March 2021 FOR RECOMMENDATION BY SAGE Prepared by the SAGE Working Group on COVID-19 vaccines EVIDENCE ASSESSMENT: Ad26.COV2.S COVID-19 vaccine Key evidence to inform policy recommendations on the use of Ad26.COV2.S COVID-19 vaccine Evidence retrieval • Based on WHO and Cochrane living mapping and living systematic review of Covid-19 trials (www.covid-nma.com/vaccines) Retrieved evidence Majority of data considered for policy recommendations on Ad26.COV2.S Covid-19 vaccine are published in scientific peer reviewed journals: • Interim Results of a Phase 1–2a Trial of Ad26.COV2.S Covid-19 Vaccine. NEJM. February 2021. DOI: 10.1056/NEJMoa2034201. Jerald Sadoff, Mathieu Le Gars, Georgi Shukarev, et al. • FDA briefing document Janssen Ad26.COV2.S (COVID-19) Vaccine • Ad26 platform literature: Custers et al. Vaccines based on the Ad26 platform; Vaccine 2021 Quality assessment Type of bias Randomization Deviations from Missing outcome Measurement of Selection of the Overall risk of intervention data the outcome reported results bias Working Group Low Low Low Low Low LOW judgment 1 EVIDENCE ASSESSMENT The SAGE Working Group specifically considered the following issues: 1. Trial endpoints used in comparison with other vaccines Saad Omer 2. Evidence on vaccine efficacy in the total population and in different subgroups Cristiana Toscano 3. Evidence of vaccine efficacy against asymptomatic infections, reducing severity, hospitalisations, deaths, and efficacy against virus variants of concern Annelies Wilder-Smith 4. Vaccination after SARS-CoV2 infection. 5. Evidence on vaccine safety in the total population and in different subgroups Sonali Kochhar 6. -

Issues to Consider: Smallpox Response Plans
ISSUES TO CONSIDER: SMALLPOX RESPONSE PLANS Smallpox is one of history’s greatest scourges, and its eradication is one of medicine’s greatest triumphs. Because it is both highly contagious and highly lethal, smallpox presents a preeminent threat as a biological weapon. While all the countries represented in Atlantic Storm have smallpox response plans, which vary widely in their substance and length, all address roughly the same set of key issues: 1. Alert Levels • Most countries have developed a system of “alert levels” that direct their actions for preparedness and response. • Alert levels generally start at “zero,” which signifies no cases of smallpox anywhere in the world, and progress upward through levels determined according to the number and location of suspected and/or confirmed smallpox cases. • The most vigorous responses are triggered when smallpox cases appear within a given country’s boundaries. 2. Smallpox Vaccine and Vaccination Strategies • Countries have varying amounts of smallpox vaccine stockpiled for use in an emergency. Some countries have enough vaccine to cover every person in the nation, while others have minimal amounts that would cover less than 5% of their population. • Most countries, and the World Health Organization, consider “ring vaccination” to be the preferred strategy for controlling the spread of disease. Ring vaccination is typically characterized by an effort to identify and vaccinate all of the direct contacts of confirmed smallpox victims, including friends, family members, and co- workers. • Most countries indicate that if it appears that a smallpox epidemic cannot be controlled through ring vaccination, they would switch to mass vaccination, which is the vaccination of all individuals in an area (city, region, or entire country) regardless of exposure to the smallpox virus. -

Improving the Regulatory Response to Vaccine Development During a Public Health Emergency
Every Minute Matters: Improving the Regulatory Response to Vaccine Development During a Public Health Emergency RASHMI BORAH* ABSTRACT In recent months, our lives have been turned upside down by the novel coronavirus (COVID-19) emergency. With no cure or vaccine in sight, millions of people have contracted the virus, and the death toll has surpassed that of World War I in a fraction of the time. In fact, the past decade has been marked by a series of highly publicized public health emergencies, including the devastating Ebola and Zika virus global outbreaks. Some of this panic arose from a failure to manufacture and distribute vaccines in a timely fashion. This failure occurred despite having several viable vaccine candidates, adequate funding, and strong public support for the vaccines. This Article explains how these failures are the consequence of a complex network of existing regulatory pathways and insufficient incentives to produce affordable vaccinations during a public health emergency. Fortunately, there are several ways that both the U.S. Patent and Trademark Office and the U.S. Food and Drug Administration can improve and streamline the process of patenting, approving, manufacturing, and distributing a vaccination. The last decade has demonstrated that public health emergencies occur quickly, and affected communities cannot afford the delays and mishaps that characterized the vaccine response to COVID-19, Ebola, and Zika. This Article explores three ways to facilitate the development and distribution of vaccinations during a public health emergency. First, the U.S. Patent and Trademark Office can establish a dedicated public health emergency patent pathway for vaccine technology developed specifically in response to a public health emergency. -
Candidate SARS-Cov-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D
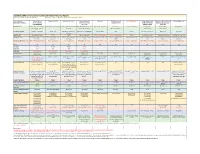
Candidate SARS-CoV-2 Vaccines in Advanced Clinical Trials: Key Aspects Compiled by John D. Grabenstein, RPh, PhD All dates are estimates. All Days are based on first vaccination at Day 0. Vaccine Sponsor Univ. of Oxford ModernaTX USA BioNTech with Pfizer Johnson & Johnson Novavax Sanofi Pasteur with CureVac with Bayer CanSino Biologics with Sinopharm (China National Sinovac Biotech Co. [with Major Partners] (Jenner Institute) (Janssen Vaccines & GlaxoSmithKline Academy of Military Biotec Group) (Beijing IBP, with AstraZeneca Prevention) Medical Sciences Wuhan IBP) Headquarters Oxford, England; Cambridge, Cambridge, Massachusetts Mainz, Germany; New York, New Brunswick, New Jersey Gaithersburg, Maryland Lyon, France; Tübingen, Germany Tianjin, China; Beijing, China; Beijing, China England, Gothenburg, New York (Leiden, Netherlands) Brentford, England Beijing, China Wuhan, China Sweden Product Designator ChAdOx1 or AZD1222 mRNA-1273 BNT162b2, tozinameran, Ad26.COV2.S, JNJ-78436735 NVX-CoV2373 TBA CVnCoV Ad5-nCoV, Convidecia BBIBP-CorV CoronaVac Comirnaty Vaccine Type Adenovirus 63 vector mRNA mRNA Adenovirus 26 vector Subunit (spike) protein Subunit (spike) protein mRNA Adenovirus 5 vector Inactivated whole virus Inactivated whole virus Product Features Chimpanzee adenovirus type Within lipid nanoparticle Within lipid nanoparticle Human adenovirus type 26 Adjuvanted with Matrix-M Adjuvanted with AS03 or Adjuvanted with AS03 Human adenovirus type 5 Adjuvanted with aluminum Adjuvanted with aluminum 63 vector dispersion dispersion vector AF03 -

What Clinicians Need to Know About Johnson & Johnson's Janssen COVID-19 Vaccine
Centers for Disease Control and Prevention Center for Preparedness and Response What Clinicians Need to Know About Johnson & Johnson’s Janssen COVID-19 Vaccine Clinician Outreach and Communication Activity (COCA) Webinar Tuesday, March 2, 2021 To Ask a Question ▪ All participants joining us today are in listen-only mode. ▪ Using the Webinar System – Click the “Q&A” button. – Type your question in the “Q&A” box. – Submit your question. ▪ The video recording of this COCA Call will be posted at https://emergency.cdc.gov/coca/calls/2021/callinfo_030221.asp and available to view on-demand a few hours after the call ends. ▪ If you are a patient, please refer your questions to your healthcare provider. ▪ For media questions, please contact CDC Media Relations at 404-639-3286, or send an email to [email protected]. Today’s Presenters ▪ Sarah Mbaeyi, MD, MPH CDR, U.S. Public Health Service Medical Officer National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention ▪ Sara Oliver, MD LCDR, U.S. Public Health Service Co-lead, Advisory Committee for Immunization Practices COVID-19 Vaccines Work Group COVID-19 Response Centers for Disease Control and Prevention ▪ Kathleen Dooling, MD, MPH Medical Officer Co-lead, Advisory Committee for Immunization Practices COVID-19 Vaccines Work Group COVID-19 Response Centers for Disease Control and Prevention ACIP COVID-19 Vaccines What Clinicians Need to Know about Johnson and Johnson’s Janssen COVID-19 vaccine Sara Oliver MD, MSPH Sarah Mbaeyi MD, MPH Kathleen Dooling MD, MPH March 2, 2021 For more information: www.cdc.gov/COVID19 Outline: 1) Safety and efficacy of Janssen COVID-19 vaccines Dr. -

Smallpox: Should Everyone Be Vaccinated?
10/25/2019 WebMD/Lycos - Article - Smallpox: Should Everyone Be Vaccinated? Lycos Home | Site Map | My Lycos SEARCH HEALTH FOR: Search Health Home Smallpox: Should Everyone Be Health News Vaccinated? Conditions A-Z Drugs & Herbs Study Says 'Yes' -- If Biological Terrorist Attack Has Occurred Wellness Topics By Jeanie Davis Medical Library Resource Center Health Calculators July 10, 2002 -- America is gearing up for the worst-case scenario - Find a Physician - a deadly smallpox attack. The best defense is mass inoculation, Chat & Events with all U.S. residents rolling up their sleeves as soon as there's Message Boards evidence of exposure, says one Yale epidemiologist. Member Columns The Yale report comes on the heels of a new federal announcement -- one calling for vaccination of emergency personnel and Sign In healthcare workers, some 500,000 people. Each state would Post a message, designate teams to receive the shots, teams that will consist of chat... doctors, disease trackers, nurses, lab workers, and law enforcement Join officers -- the first to respond in case of bioterrorism attack, Free newsletters according to the Department of Health and Human Services. and more Volunteers at four sites around the country are already being Event Highlight inoculated with diluted doses of two vaccines to test their effectiveness. A vaccine known as Dryvax was made 20 years ago; Monday, August 15 million doses of it are available. Another vaccine by Aventis 26, 2002 9:00 Pasteur, Inc., was donated to the government; the company has a.m. stockpiled it for decades. Virtual Vacation: Lake Austin Spa "I think it makes sense to vaccinate emergency responders pre- Resort attack, precisely so that there will be a pool of persons who can protect the rest of us," says Edward H. -
COVID-19 Vaccine Communication Guide Presented By
COVID-19 Vaccine Communication Guide Presented by In collaboration with Table of Contents Purpose ......................................................................................................................................................... 3 What vaccines are available for COVID-19? ................................................................................................... 3 How do the vaccines work? ............................................................................................................................ 3 How many shots will I need? .......................................................................................................................... 4 How effective are the different vaccines? ....................................................................................................... 4 How do we know if the COVID-19 vaccines are safe? ..................................................................................... 4 What are side-effects of the vaccine? ............................................................................................................. 5 Vaccine Hesitancy .......................................................................................................................................... 5 COVID Vaccine Communication Strategies ..................................................................................................... 5 Reflection ................................................................................................................................................................ -

Ring Vaccination and Smallpox Control Mirjam Kretzschmar,* Susan Van Den Hof,* Jacco Wallinga,* and Jan Van Wijngaarden†
RESEARCH Ring Vaccination and Smallpox Control Mirjam Kretzschmar,* Susan van den Hof,* Jacco Wallinga,* and Jan van Wijngaarden† We present a stochastic model for the spread of small- We investigated which conditions are the best for effec- pox after a small number of index cases are introduced into tive use of ring vaccination, a strategy in which direct con- a susceptible population. The model describes a branching tacts of diagnosed cases are identified and vaccinated. We process for the spread of the infection and the effects of also investigated whether monitoring contacts contributes intervention measures. We discuss scenarios in which ring to the success of ring vaccination. We used a stochastic vaccination of direct contacts of infected persons is suffi- cient to contain an epidemic. Ring vaccination can be suc- model that distinguished between close and casual con- cessful if infectious cases are rapidly diagnosed. However, tacts to explore the variability in the number of infected because of the inherent stochastic nature of epidemic out- persons during an outbreak, and the time until the outbreak breaks, both the size and duration of contained outbreaks is over. We derived expressions for the basic reproduction are highly variable. Intervention requirements depend on number (R0) and the effective reproduction number (Rυ). the basic reproduction number (R0), for which different esti- We investigated how effectiveness of ring vaccination mates exist. When faced with the decision of whether to rely depends on the time until diagnosis of a symptomatic case, on ring vaccination, the public health community should be the time to identify and vaccinate contacts in the close con- aware that an epidemic might take time to subside even for tact and casual contact ring, and the vaccination coverage an eventually successful intervention strategy. -

Evolving Pharmacovigilance Requirements with Novel Vaccines and Vaccine Components
Analysis BMJ Glob Health: first published as 10.1136/bmjgh-2020-003403 on 19 May 2021. Downloaded from Evolving pharmacovigilance requirements with novel vaccines and vaccine components 1 2 3 4 Patrick L F Zuber , Marion Gruber, David C Kaslow, Robert T Chen, Brigitte K Giersing,5 Martin H Friede5 To cite: Zuber PLF, Gruber M, ABSTRACT Summary box Kaslow DC, et al. Evolving This paper explores the pipeline of new and upcoming pharmacovigilance requirements vaccines as it relates to monitoring their safety. Compared ► Novel vaccine technologies include genetic mod- with novel vaccines and vaccine with most currently available vaccines, that are constituted components. BMJ Global Health ifications of micro- organisms, viral vectors, use of live attenuated organisms or inactive products, future 2021;6:e003403. doi:10.1136/ of nucleic acids or novel adjuvants, they also in- vaccines will also be based on new technologies. Several bmjgh-2020-003403 clude increased valences and different routes of products that include such technologies are either administration. already licensed or at an advanced stage of clinical Handling editor Seye Abimbola ► Those new characteristics will modify untoward development. Those include viral vectors, genetically reactions, specific and non- specific, and will also attenuated live organisms, nucleic acid vaccines, novel Received 9 July 2020 require new pharmaco-epidemiological approaches. Revised 4 August 2020 adjuvants, increased number of antigens present in a ► The risk management plans for those products will Accepted 9 August 2020 single vaccine, novel mode of vaccine administration and have to factor those new theoretical concerns and thermostabilisation. The Global Advisory Committee on propose ways of monitoring them during the prod- Vaccine Safety (GACVS) monitors novel vaccines, from the ucts life- cycle. -

Modelling the Impact of a Smallpox Attack in India and Influence of Disease Control Measures
Open access Original research BMJ Open: first published as 10.1136/bmjopen-2020-038480 on 13 December 2020. Downloaded from Modelling the impact of a smallpox attack in India and influence of disease control measures Biswajit Mohanty,1 Valentina Costantino ,2 Jai Narain,1 Abrar Ahmad Chughtai,1 Arpita Das,2 C Raina MacIntyre 2 To cite: Mohanty B, ABSTRACT Strengths and limitations of this study Costantino V, Narain J, et al. Objectives To estimate the impact of a smallpox attack Modelling the impact of a in Mumbai, India, examine the impact of case isolation ► The model takes into account heterogeneity of age, smallpox attack in India and ring vaccination for epidemic containment and test and influence of disease disease transmission and immunological levels. the health system capacity under different scenarios with control measures. BMJ Open ► Age- specific rates of immunosuppressive condi- available interventions. 2020;10:e038480. doi:10.1136/ tions were estimated for Mumbai and included in Setting The research is based on Mumbai, India bmjopen-2020-038480 the model. population. ► This study does not include different route of trans- ► Prepublication history and Interventions We tested 50%, 70%, 90% of case mission than airborne. additional material for this paper isolation and contacts traced and vaccinated (ring is available online. To view these ► Other aspects that could influence transmission in- vaccination) in the susceptible, exposed, infected, files, please visit the journal clude seasonality, or vaccination effectiveness such recovered model and varied the start of intervention online (http:// dx. doi. org/ 10. as vaccine refusal were not included in the model. -
(GEVIT) Practical Guidance on the Use of Ebola Vaccine in an Outbreak Response
EBOLA STRATEGY Global Ebola Vaccine Implementation Team (GEVIT) Practical guidance on the use of Ebola vaccine in an outbreak response Draft Guidance, May 2016 Draft - Not for Implementation This guidance is being distributed for comment purposes only. © World Health Organization 2016. All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. Draft-Not for Implementation Contents Contents ......................................................................................................................................... 2 Abbreviations and acronyms ........................................................................................................... 4 Acknowledgements ........................................................................................................................