Testimony Medicaid and CHIP in the U.S. Territories
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

District of Columbia Statehood and Voting Representation
Updated June 29, 2020 District of Columbia Statehood and Voting Representation On June 26, 2020, the U.S. House of Representatives have included full statehood or more limited methods of considered and passed the Washington, D.C. Admission providing DC residents the ability to vote in congressional Act, H.R. 51. This marked the first time in 27 years a elections. Some Members of Congress have opposed these District of Columbia (DC) statehood bill was considered on legislative efforts and recommended maintaining the status the floor of the House of Representatives, and the first time quo. Past legislative proposals have generally aligned with in the history of Congress a DC statehood bill was passed one of the following five options: by either the House or the Senate. 1. a constitutional amendment to give DC residents voting representation in This In Focus discusses the political status of DC, identifies Congress; concerns regarding DC representation, describes selected issues in the statehood process, and outlines some recent 2. retrocession of the District of Columbia DC statehood or voting representation bills. It does not to Maryland; provide legal or constitutional analysis on DC statehood or 3. semi-retrocession (i.e., allowing qualified voting representation. It does not address territorial DC residents to vote in Maryland in statehood issues. For information and analysis on these and federal elections for the Maryland other issues, please refer to the CRS products listed in the congressional delegation to the House and final section. Senate); 4. statehood for the District of Columbia; District of Columbia and When ratified in 1788, the U.S. -

Environmental Assessment for the Replacement of the Pier and Boat Ramp at the U.S
Draft Environmental Assessment for the Repairs and Replacement of the Boat Ramp and Pier at the US Border Patrol Air and Marine Facility, Ponce, Puerto Rico Environmental Assessment for the Replacement of the Pier and Boat Ramp at the U.S. Border Patrol & Air and Marine Facility, Ponce, Puerto Rico U.S. Customs and Border Protection February 2019 Draft Environmental Assessment for the Repairs and Replacement of the Boat Ramp and Pier at the US Border Patrol Air and Marine Facility, Ponce, Puerto Rico Environmental Assessment for the Replacement of the Pier and Boat Ramp at the U.S. Border Patrol & Air and Marine Facility, Ponce, Puerto Rico Environmental Assessment for the Replacement of the Pier and Boat Ramp at the U.S. Border Patrol & Air and Marine Facility, Ponce, Puerto Rico Lead Agency: U.S. Customs and Border Protection (CBP) Proposed Action: The demolition and removal of the temporary structure, removal of the original pier, construction of a new pier, and replacement of the boat ramp at 41 Bonaire Street in the municipality of Ponce, Puerto Rico. The replacement boat ramp would be constructed in the same location as the existing boat ramp, and the pier would be constructed south of the Ponce Marine Unit facility. For Further Information: Joseph Zidron Real Estate and Environmental Branch Chief Border Patrol & Air and Marine Program Management Office 24000 Avila Road, Suite 5020 Laguna Niguel, CA 92677 [email protected] Date: February 2019 Abstract: CBP proposes to remove the original concrete pier, demolish and remove the temporary structure, construct a new pier, replace the existing boat ramp, and continue operation and maintenance at its Ponce Marine Unit facility at 41 Bonaire Street, Ponce, Puerto Rico. -
Ruling America's Colonies: the Insular Cases Juan R
YALE LAW & POLICY REVIEW Ruling America's Colonies: The Insular Cases Juan R. Torruella* INTRODUCTION .................................................................. 58 I. THE HISTORICAL BACKDROP TO THE INSULAR CASES..................................-59 11. THE INSULAR CASES ARE DECIDED ......................................... 65 III. LIFE AFTER THE INSULAR CASES.......................... .................. 74 A. Colonialism 1o ......................................................... 74 B. The Grinding Stone Keeps Grinding........... ....... ......................... 74 C. The Jones Act of 1917, U.S. Citizenship, and President Taft ................. 75 D. The Jones Act of 1917, U.S. Citizenship, and ChiefJustice Taft ............ 77 E. Local Self-Government v. Colonial Status...........................79 IV. WHY THE UNITED STATES-PUERTO Rico RELATIONSHIP IS COLONIAL...... 81 A. The PoliticalManifestations of Puerto Rico's Colonial Relationship.......82 B. The Economic Manifestationsof Puerto Rico's ColonialRelationship.....82 C. The Cultural Manifestationsof Puerto Rico's Colonial Relationship.......89 V. THE COLONIAL STATUS OF PUERTO Rico Is UNAUTHORIZED BY THE CONSTITUTION AND CONTRAVENES THE LAW OF THE LAND AS MANIFESTED IN BINDING TREATIES ENTERED INTO BY THE UNITED STATES ............................................................. 92 CONCLUSION .................................................................... 94 * Judge, United States Court of Appeals for the First Circuit. The substance of this Article was presented in -

Excavations at Maruca, a Preceramic Site in Southern Puerto Rico
EXCAVATIONS AT MARUCA, A PRECERAMIC SITE IN SOUTHERN PUERTO RICO Miguel Rodríguez ABSTRACT A recent set of radiocarbon dated shows that the Maruca site, a preceramic site located in the southern coastal plains of Puerto Rico, was inhabited between 5,000 and 3,000 B.P. bearing the earliest dates for human habitation in Puerto Rico. Also the discovery in the site of possible postmolds, lithic and shell workshop areas and at least eleven human burials strongly indicate the possibility of a permanent habitation site. RESUME Recientes fechados indican una antigüedad entre 5,000 a 3000 años antes de del presente para Maruca, una comunidad Arcaica en la costa sur de Puerto Rico. Estos son al momento los fechados más antiguos para la vida humana en Puerto Rico. El descubrimiento de socos, de posible talleres líticos, de áreas procesamiento de moluscos y por lo menos once (11) enterramientos humanos sugieren la posibilidad de que Maruca sea un lugar habitation con cierta permanence. KEY WORDS: Human Remains, Marjuca Site, Preceramic Workshop. INTRODUCTION During the 1980s archaeological research in Puerto Rico focused on long term multidisciplinary projects in early ceramic sites such as Sorcé/La Hueca, Maisabel and Punta Candelera. This research significantly expanded our knowledge of the life ways and adaptive strategies of Cedrosan and Huecan Saladoid cultures. Although the interest in these early ceramic cultures has not declined, it seems that during the 1990s, archaeological research began to develop other areas of interest. With the discovery of new preceramic sites of the Archaic age found during construction projects, the attention of specialists has again been focused on the first in habitants of Puerto Rico. -

Puerto Rico, Colonialism In
University at Albany, State University of New York Scholars Archive Latin American, Caribbean, and U.S. Latino Latin American, Caribbean, and U.S. Latino Studies Faculty Scholarship Studies 2005 Puerto Rico, Colonialism In Pedro Caban University at Albany, State Univeristy of New York, [email protected] Follow this and additional works at: https://scholarsarchive.library.albany.edu/lacs_fac_scholar Part of the Latin American Studies Commons Recommended Citation Caban, Pedro, "Puerto Rico, Colonialism In" (2005). Latin American, Caribbean, and U.S. Latino Studies Faculty Scholarship. 19. https://scholarsarchive.library.albany.edu/lacs_fac_scholar/19 This Encyclopedia Entry is brought to you for free and open access by the Latin American, Caribbean, and U.S. Latino Studies at Scholars Archive. It has been accepted for inclusion in Latin American, Caribbean, and U.S. Latino Studies Faculty Scholarship by an authorized administrator of Scholars Archive. For more information, please contact [email protected]. 516 PUERTO RICO, COLONIALISM IN PUERTO RICO, COLONIALISM IN. Puerto Rico They automatically became subjects of the United States has been a colonial possession of the United States since without any constitutionally protected rights. Despite the 1898. What makes Puerto Rico a colony? The simple an humiliation of being denied any involvement in fateful swer is that its people lack sovereignty and are denied the decisions in Paris, most Puerto Ricans welcomed U.S. fundamental right to freely govern themselves. The U.S. sovereignty, believing that under the presumed enlight Congress exercises unrestricted and unilateral powers over ened tutelage of the United States their long history of Puerto Rico, although the residents of Puerto Rico do not colonial rule would soon come to an end. -
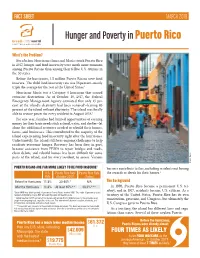
Hunger and Poverty in Puerto Rico
FACT SHEET MARCH 2019 Hunger and Poverty in Puerto Rico What’s the Problem? Even before Hurricanes Irma and Maria struck Puerto Rico in 2017, hunger and food insecurity were much more common among Puerto Ricans than among their fellow U.S. citizens in the 50 states. Before the hurricanes, 1.5 million Puerto Ricans were food insecure. The child food insecurity rate was 56 percent—nearly triple the average for the rest of the United States.1 Hurricane Maria was a Category 4 hurricane that caused extensive destruction. As of October 10, 2017, the Federal Emergency Management Agency estimated that only 15 per- cent of the island’s electricity had been restored2—leaving 85 percent of the island without electricity. The island was finally able to restore power for every resident in August 2018.3 For one year, families had limited opportunities of earning money for their basic needs such as food, water, and shelter—let alone the additional resources needed to rebuild their homes, farms, and businesses. This contributed to the majority of the island experiencing food insecurity right after the hurricanes. Unfortunately, the island still faces ongoing challenges to help residents overcome hunger. Recovery has been slow, in part, because assistance from FEMA to repair bridges and roads, clean debris, and rebuild homes has been difficult for some parts of the island, and for every resident, to access. Various iStock photo 5 PUERTO RICANS ARE FAR MORE LIKELY TO BE FOOD INSECURE barriers contribute to this, including residents not having U.S. Puerto Rico Rate Puerto Rico Rate the records or deeds for their homes.4 Rate (October 2017) (Today) Before the Hurricanes 11.8% 30-60%* N/A The Background After the Hurricanes 11.8% At least 85%** 38.3%*** In 1898, Puerto Rico became a permanent U.S. -

The Status of Puerto Rico Revisited: Does the Current U.S.-Puerto Rico Relationship Uphold International Law?
Fordham International Law Journal Volume 17, Issue 4 1993 Article 5 The Status of Puerto Rico Revisited: Does the Current U.S.-Puerto Rico Relationship Uphold International Law? Dorian A. Shaw∗ ∗ Copyright c 1993 by the authors. Fordham International Law Journal is produced by The Berke- ley Electronic Press (bepress). http://ir.lawnet.fordham.edu/ilj The Status of Puerto Rico Revisited: Does the Current U.S.-Puerto Rico Relationship Uphold International Law? Dorian A. Shaw Abstract This Note argues that the establishment of the Commonwealth government fails to fulfill the requirements of a free associated territory as detailed in United Nations General Assembly Resolu- tions 742 (“Resolution 742”) and 1541 (“Resolution 1541”) because the Puerto Rico Constitution remains subject to the Territorial Clause of the U.S. Constitution. The Territorial Clause gives the U.S. Congress plenary authority to govern territories of the United States. Part I of this Note introduces the factual and legal background of Puerto Rico’s hybrid legal status. Part II describes the different interpretations regarding the validity of Puerto Rico’s status in international law. Part III argues that the present status of Puerto Rico requires that the U.S. Congress enact legislation that allows a binding plebiscite to define the status of Puerto Rico in a manner consistent with U.N. General Assembly Resolutions 742 and 1541. Finally, this Note concludes that the U.S. Congress should act to prevent the continuation of a system of government where unequal treatment of U.S. citizens in Puerto Rico is allowed under the U.S. -
PUERTO RICO Information on How Statehood Would Potentially Affect Selected Federal Programs and Revenue Sources
United States Government Accountability Office Report to Congressional Requesters March 2014 PUERTO RICO Information on How Statehood Would Potentially Affect Selected Federal Programs and Revenue Sources GAO-14-31 March 2014 PUERTO RICO Information on How Statehood Would P otentially Affect S elected Federal Programs and Revenue Highlights of GAO-14-31, a report to Sources congressional requesters Why GAO Did This Study What GAO Found Puerto Rico has access to many Of the 29 federal programs GAO reviewed (which accounted for about 86 federal programs, and is subject to percent of federal program spending for states or their residents in fiscal year certain federal tax laws; however, for 2010), statehood would likely affect 11 programs. For 3 other programs, while some programs and for some aspects the programs themselves would likely not change under statehood, eligibility of tax law, Puerto Rico is treated determinations for these programs could be affected indirectly by changes that differently than the states. Options for could occur to benefits in other programs. Statehood would not likely affect the Puerto Rico’s political status include 15 remaining programs. See figure below. statehood. GAO was asked to review potential fiscal implications for federal programs if Puerto Rico were to become a state. This report examines potential changes to selected federal programs and related spending changes, and changes to selected federal revenue sources that would be expected should Puerto Rico become a state. This report also discusses economic and fiscal factors under statehood that could influence changes in spending and revenues. To evaluate potential changes to selected federal programs and revenue sources, GAO reviewed federal laws and regulations and interviewed federal and Puerto Rico agency officials. -

Puerto Ricans in Orlando and Central Florida
Centro de Estudios Puertorriqueños Hunter College (CUNY) Policy rePort | VOLUMe 1 | No. 1 |sPriNg 2006 Puerto Ricans in Orlando and Central Florida Jorge Duany Félix V. Matos-roDríguez Puerto Ricans in Orlando and Central Florida Jorge Duany Department of sociology and Anthropology University of Puerto rico, río Piedras This report was sponsored by the Orlando Regional Chamber of Commerce and Orange County Government. Félix V. Matos-roDríguez centro de estudios Puertorriqueños Hunter college, city University of New york Contents Summary of Main Findings . 2 Acknowledgments . 5 Introduction . 5 Changing Settlement Patterns . 8 Historical Background . 12 Centro de Estudios Puertorriqueños A Contemporary Socioeconomic Portrait . 15 Hunter College (CUNY) Political Incorporation . 22 695 Park Avenue, Room E-1429 New York, New York 10021 Cultural Identities . 24 212.772.5686 Toward a New Research Agenda . 26 www.centropr.org Conclusion . 29 Notes . 30 References . 33 Biographical Sketches . 39 ...2... ...1... SUMMARY OF MAIN FINDINGS • Between 1990 and 2000, the city of orlando experienced the largest increase (142 percent) in the number of Puerto ricans • During the 1990s, Florida displaced New Jersey as the second largest stateside. today, orlando is the fourth-largest metropolitan concentration of Puerto ricans in the U.s. mainland (after New york). area for Puerto ricans in the United states, after New york city, Florida’s Puerto rican population grew from slightly more than 2 percent Philadelphia, and chicago. of all stateside Puerto ricans in 1960 to more than 14 percent in the year • Puerto rican migration to central Florida is not highly selective by sex. 2000. Furthermore, the number of Puerto rican residents in Florida island-born and mainland-born residents have very similar proportions rose from 482,027 in 2000 to 571,755 persons in 2003. -

Political Status of Puerto Rico: Brief Background and Recent Developments for Congress
Political Status of Puerto Rico: Brief Background and Recent Developments for Congress R. Sam Garrett Specialist in American National Government June 12, 2017 Congressional Research Service 7-5700 www.crs.gov R44721 Political Status of Puerto Rico: Brief Background and Recent Developments for Congress Summary Puerto Rico lies approximately 1,000 miles southeast of Miami and 1,500 miles from Washington, DC. Despite being far outside the continental United States, the island has played a significant role in American politics and policy since the United States acquired Puerto Rico from Spain in 1898. Puerto Rico’s political status—referring to the relationship between the federal government and a territorial one—is an undercurrent in virtually every policy matter on the island. In a June 11, 2017, plebiscite (popular vote), 97.2% of voters chose statehood when presented with three options on the ballot. Turnout for the plebiscite was 23.0% of eligible voters. Some parties and other groups opposing the plebiscite had urged their bases to boycott the vote. (These data are based on 99.5% of precincts reporting results.) After initially including only statehood and free association/independence options, an amended territorial law ultimately permitted three options on the plebiscite ballot: statehood, free association/independence, or current territorial status. Before the latest plebiscite, Puerto Ricans most recently reconsidered their status through a 2012 plebiscite. On that occasion, voters were asked two questions: whether to maintain the status quo, and if a change were selected, whether to pursue statehood, independence, or status as a “sovereign free associated state.” Majorities chose a change in the status quo in answering the first question, and statehood in answering the second. -

Puerto Rico and Florida Manatees Represent Genetically Distinct Groups
Puerto Rico and Florida manatees represent genetically distinct groups Margaret E. Hunter, Antonio A. Mignucci-Giannoni, Kimberly Pause Tucker, Timothy L. King, Robert K. Bonde, Brian A. Gray, et al. Conservation Genetics ISSN 1566-0621 Conserv Genet DOI 10.1007/s10592-012-0414-2 1 23 Your article is protected by copyright and all rights are held exclusively by Springer Science +Business Media Dordrecht 2012 (outside the USA). This e-offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your work, please use the accepted author’s version for posting to your own website or your institution’s repository. You may further deposit the accepted author’s version on a funder’s repository at a funder’s request, provided it is not made publicly available until 12 months after publication. 1 23 Author's personal copy Conserv Genet DOI 10.1007/s10592-012-0414-2 RESEARCH ARTICLE Puerto Rico and Florida manatees represent genetically distinct groups Margaret E. Hunter • Antonio A. Mignucci-Giannoni • Kimberly Pause Tucker • Timothy L. King • Robert K. Bonde • Brian A. Gray • Peter M. McGuire Received: 10 January 2012 / Accepted: 24 September 2012 Ó Springer Science+Business Media Dordrecht 2012 (outside the USA) 2012 Abstract The West Indian manatee (Trichechus manatus) suggested reclassification of the species to a threatened or populations in Florida (T. m. latirostris) and Puerto Rico delisted status. However, the two populations are geo- (T. m. manatus) are considered distinct subspecies and are graphically distant, morphologically distinct, and habitat listed together as endangered under the United States degradation and boat strikes continue to threaten the Puerto Endangered Species Act. -

Redalyc.Borinki Identity in Hawai`I: Present and Future
Centro Journal ISSN: 1538-6279 [email protected] The City University of New York Estados Unidos López, Iris; Forbes, David Borinki identity in Hawai`i: present and future Centro Journal, vol. XIII, núm. 1, 2001, pp. 110-127 The City University of New York New York, Estados Unidos Disponible en: http://www.redalyc.org/articulo.oa?id=37711309008 Cómo citar el artículo Número completo Sistema de Información Científica Más información del artículo Red de Revistas Científicas de América Latina, el Caribe, España y Portugal Página de la revista en redalyc.org Proyecto académico sin fines de lucro, desarrollado bajo la iniciativa de acceso abierto CENTRO(Spring2001)final.qxd 7/22/07 2:34 PM Page 110 Jolly Babes 1953. Courtesy Raymond Pagán. Second Time Around 1990. Courtesy Raymond Pagán. At the CasitaWaipaliu Cultural Center. Courtesy Shirley Colón. Borinki Identity in Hawai`i: Present and Future Iris López and David Forbes Puerto Ricans in Hawai‘i, or Borinkis, as they like to call themselves, comprise a small ethnic group situated within a unique multiethnic society that is marked by a distinc- tive local history and culture. This “local culture” in turn lies within a world of global- izing forces driven by transnational corporations that impact the nature of everyday life. This configuration of forces raises at least three related questions about the mean- ing and future of Puerto Rican identity in Hawai‘i: 1) Are Puerto Ricans in Hawai‘i dis- appearing, as some argue (Carr 1987), given that so few of the residents of the state self- identify as Puerto Rican and they have such a high rate of intermarriage, or are they thriving? 2) Is Puerto Rican identity in Hawai‘i still “Puerto Rican” or is it becoming more “local”?1 And, 3) Are local Puerto Ricans able to maintain their local identity or is their identity becoming more influenced by the forces of globalization? In contemporary Hawai‘i, we can identify three levels of culture that co-exist and overlap: North American (global), local (inter-group), and ethnic (intra-group).