Fauldhouse and the Breich Valley Health Inequalities Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Retirement Housing
Blackfaulds Court BLACKFAULDS COURT Fauldhouse EH47 9DR Answering your questions You’ll find our properties are built on a small scale and are very welcoming. Isn’t it time to discover for yourself what makes Bield different? What does the accommodation comprise What facilities are available? of? There is a communal lounge where residents and their The flats are fully self-contained with a living room, family and friends can meet and chat over a cuppa. bedroom, separate kitchen and bathroom. All Social activities are often held here. accommodation has central heating and is double Purpose built laundries with fast automatic washing glazed throughout. machines and tumble driers are available for all. Will I have privacy? Who maintains these areas and gardens? Yes. You have your own front door with additional Bield maintains the gardens, all external areas and sets of keys available for your family. Post is delivered internal communal spaces. The cost is included in your to your door. rent. Can I bring my own furniture? Can I bring my pet? Flats are rented unfurnished but you may qualify for We are more than happy to welcome well behaved a decorating allowance to help you make your home pets but please check with our staff first. your own. Friends and families are always What will I do if I need a repair to my property? welcome at Blackfaulds Court. Contact your Local Manager or Property Officer to arrange all repairs. The cost of repairs is included in your rent payment. What happens if I want to carry out improvements/ alterations to my property? Contact your Bield Property Officer who will visit you to discuss your plans. -

Pdf X22, X23 Shotts
X22 X23 Shotts - Edinburgh Serving: Harthill (X22 ) Whitburn (X22 ) Blackburn (X22 ) Deans (X23 ) Eliburn (X23 ) Livingston Dedridge East Mid Calder East Calder Hermiston Park & Ride Bus times from 27 January 2020 GET A DOWNLOAD OF THIS. NEW EASY APP THE NEW FIRST BUS APP IS THE SMARTER WAY TO GET WHERE YOU’RE GOING. IT’S HERE TO HELP WITH EVERY PART OF YOUR JOURNEY. Real-time bus updates and simple, secure mTicket purchasing on the new First Bus App mean you can be on your way even quicker. Simply download the Running late? No problem! The First Bus App, and you’ll be First Bus App also lets you know able to securely buy and store when your next bus is arriving. tickets on your phone. You Simply hop on board, pay using never have to worry about your First Bus App, contactless losing your pass or forgetting card, Apple Pay or Google Pay, your change again! and you’re ready to go! TECH THE BUS WITH LESS FUSS Thanks for choosing to travel with First. Our gu ide will help you plan your next bus journey or for more information visit: www.firstscotlandeast.com Customer Services 0345 646 0707 (Mon-Fri 7am-7pm & weekends 9am-5pm) @FirstScotland FirstScotlandEast Carmuirs House, 300 Stirling Road, Larbert, FK5 3NJ A ch o ice of tickets We offer a range of tickets to suit your travelling needs. As well a s singles and returns , we have tickets offering unlimited travel such as First Day , First Week , First 4Week and First Year . Contact our Customer Services team for more information. -

Fauldhouse Together Issue 44
The latest news on developments in the village, from the F&BV CDT Team Fauldhouse Together Issue 44, Winter/Spring 2020 It’s that Spring Hunt time again! The Fauldhouse and Breich Valley Community Development Trust is holding a Fauldhouse Spring Hunt again this year. The hunt is aimed at primary school aged children, so if your child would like to take part in the Fauldhouse Spring Hunt, why not pick up a clue sheet from The Hub between Thursday 2 April and Thursday 9 April (from 10am - 2pm)? Entry costs £1.50 per clue sheet/per child. It’s during the school’s Spring holidays so why not get out and about with your children? When you have picked up your entry sheet from The Hub, you can then hunt around Fauldhouse looking for the clues. Once you have found all the clues, answered the questions and completed your sheet, please hand it back into The Hub and you will receive a chocolate egg. Hand in your finished sheet before Photo: Ann Holloway 2pm on Thursday 9 April to claim your prize. Get hunting! We are also having a free raffle for the children who take part, to give them the opportunity to win extra goodies. Kids will be given a raffle ticket when they hand in their completed sheet. If you need more information, contact F&BV CDT, The Hub, 10 Main Street, Fauldhouse, EH47 9HX. Tel: 01501 773 699 or email [email protected] Fauldhouse Together is published by the Fauldhouse and Breich Valley Community Development Trust Ltd, 10 Main Street, Fauldhouse, West Lothian, EH47 9HX. -

FAULDHOUSE, BATHGATE, WEST LOTHIAN, EH47 9DD Fauldhouse BATHGATE, WEST LOTHIAN, EH47 9DD
7 Caledonian Road FAULDHOUSE, BATHGATE, WEST LOTHIAN, EH47 9DD Fauldhouse BATHGATE, WEST LOTHIAN, EH47 9DD he village of Fauldhouse is well located within West Lothian and is convenient for travel in and around the region. A train station within T the village offers a regular service to both Edinburgh and Glasgow. The A71 and M8 are also within easy reach. The village is served by a choice of shops and primary schooling, with the nearest secondary schools a short bus ride away. Other everyday amenities are available nearby including a library and health centre. A more comprehensive range of everyday facilities can be found in nearby Whitburn, with further recreational facilities in the larger town of Livingston. LOCATION 7 Caledonian Road FAULDHOUSE, BATHGATE, WEST LOTHIAN, EH47 9DD ituated within this quiet location in the village of Fauldhouse, is this four/ five-bedroom, detached bungalow, all on one level and positioned on a good-sized plot, which was constructed around 1990 and has been S professionally extended on two separate occasions since. Room usage can be adapted to meet individual purchasers’ needs and will comfortably provide for a larger family. The property itself is deceptively spacious (141 m2) and provides a highly successful marriage of traditionally proportioned apartments. The property sits within well-maintained gardens, which have been designed for ease. This provides a private and safe environment for children and/or pets. Al-fresco dining and relaxing are thoroughly recommended on the patio in the rear garden. The property can be accessed via a private driveway, which offers off-road parking for two/three vehicles. -

12, Harthill Road , Fauldhouse, Bathgate, Eh47
HOME REPORT 12 HARTHILL ROAD FAULDHOUSE BATHGATE EH47 9HR ENERGY PERFORMANCE CERTIFICATE YouEnergy can use this Performance document to: Certificate (EPC) Scotland Dwellings 12 HARTHILL ROAD, FAULDHOUSE, BATHGATE, EH47 9HR Dwelling type: End-terrace house Reference number: 0170-2598-2210-2690-0255 Date of assessment: 18 September 2020 Type of assessment: RdSAP, existing dwelling Date of certificate: 21 September 2020 Approved Organisation: Elmhurst Total floor area: 104 m2 Main heating and fuel: Boiler and radiators, mains Primary Energy Indicator: 285 kWh/m2/year gas You can use this document to: • Compare current ratings of properties to see which are more energy efficient and environmentally friendly • Find out how to save energy and money and also reduce CO2 emissions by improving your home Estimated energy costs for your home for 3 years* £3,309 See your recommendations report for more Over 3 years you could save* £789 information * based upon the cost of energy for heating, hot water, lighting and ventilation, calculated using standard assumptions Very energy efficient - lower running costs Current Potential Energy Efficiency Rating (92 plus) A This graph shows the current efficiency of your home, (81-91) B taking into account both energy efficiency and fuel 83 costs. The higher this rating, the lower your fuel bills (69-80) C are likely to be. (55-68) D 67 Your current rating is band D (67). The average rating for EPCs in Scotland is band D (61). (39-54 E (21-38) The potential rating shows the effect of undertaking all F of the improvement measures listed within your (1-20) G recommendations report. -
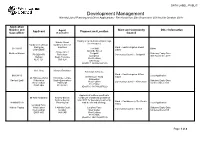
Development Management Weekly List of Planning and Other Applications - Received from 30Th September 2019 to 6Th October 2019
DATA LABEL: PUBLIC Development Management Weekly List of Planning and Other Applications - Received from 30th September 2019 to 6th October 2019 Application Number and Ward and Community Other Information Applicant Agent Proposal and Location Case officer (if applicable) Council Display of an illuminated fascia sign Natalie Gaunt (in retrospect). Cardtronics UK Ltd, Cardtronic Service trading as Solutions Ward :- East Livingston & East 0877/A/19 The Mall Other CASHZONE Calder Adelaide Street 0 Hope Street Matthew Watson Craigshill Statutory Expiry Date: PO BOX 476 Rotherham Community Council :- Craigshill Livingston 30th November 2019 Hatfield South Yorkshire West Lothian AL10 1DT S60 1LH EH54 5DZ (Grid Ref: 306586,668165) Ms L Gray Maxwell Davidson Extenison to house. Ward :- East Livingston & East 0880/H/19 Local Application 20 Hillhouse Wynd Calder 20 Hillhouse Wynd 19 Echline Terrace Kirknewton Rachael Lyall Kirknewton South Queensferry Statutory Expiry Date: West Lothian Community Council :- Kirknewton West Lothian Edinburgh 1st December 2019 EH27 8BU EH27 8BU EH30 9XH (Grid Ref: 311789,667322) Approval of matters specified in Mr Allan Middleton Andrew Bennie conditions of planning permission Andrew Bennie 0462/P/17 for boundary treatments, Ward :- Fauldhouse & The Breich 0899/MSC/19 Planning Ltd road details and drainage. Local Application Valley Longford Farm Mahlon Fautua West Calder 3 Abbotts Court Longford Farm Statutory Expiry Date: Community Council :- Breich West Lothian Dullatur West Calder 1st December 2019 EH55 8NS G68 0AP West Lothian EH55 8NS (Grid Ref: 298174,660738) Page 1 of 8 Approval of matters specified in conditions of planning permission G and L Alastair Nicol 0843/P/18 for the erection of 6 Investments EKJN Architects glamping pods, decking/walkway 0909/MSC/19 waste water tank, landscaping and Ward :- Linlithgow Local Application Duntarvie Castle Bryerton House associated works. -

With a History of the Blacks of Breich Water District
Digitized by the Internet Archive in 2012 with funding from National Library of Scotland http://www.archive.org/details/melodiesmemoriesOOblac Melodies and Memories. : BROXBURN PRINTED BY A. F. STEEL. Aelodies AND Aeavories WITH A HISTORY OP THE BLACKS OF BREICH WATER DISTRICT. By John Black GLASGOW A. M'LAREN & SON, Argyle Street 1909 c \ e^» ^ y ? in % 1964 '^ Biographical Sketch. JOHN BLACK, author of many poems and prose sketches, came upon the stage of life just as the year of grace 1849 was drawing to a close. He is the eighth of a family of four sons and eight daughters, who were brought up at the farm of East Handaxwood, in West Calder Parish, and near Fauldhouse, Linlithgowshire, the district which, as Bentybrae, he has sung and depicted with tenderness and fidelity. Mr Black comes of a rhyming family, one of his brothers and two of his sisters being capable of expressing their thoughts in verse. Early last century his maternal great- grandfather, James Smith, published a volume of verses, and was well known in Lanarkshire as " the quaint Wishaw poet." It is, however, to Robert Tennant, the postman poet, that Mr Black attributes the influence which moved him in the direction of the muse, and, being fond of reading, many of our standard poets won his esteem, and doubtless influenced his thoughts. When about twenty-three years of age, Mr Black com- menced to contribute to the poet's corner of various news- papers and magazines. A large number of his pieces have appeared in The Hamilton Advertiser. In enumerating books which have especially helped him, our friend humorously includes the Pronouncing Dictionary, which he carried in his pocket. -

Population and Household Projections for Scottish Sub-Council Areas (2012-Based)
Population and Household Projections for Scottish Sub-Council Areas (2012-based) Population projections by age and sex, and household projections by age group and household type, at sub-council area level Published on 23 March 2016 Experimental Statistics: data being developed These statistics are currently being developed and have been published to involve users and stakeholders in their development, and to build in quality and understanding at an early stage. Contents Main Points .......................................................................................................................... 5 1. Background ............................................................................................................ 8 2. Uses and limitations of projections ....................................................................... 15 3. Sub-council area projection results ...................................................................... 17 4. Methodology and assumptions ............................................................................. 55 5. Further information ............................................................................................... 77 6. Notes on statistical publications ......................................................................... 142 7. Related organisations......................................................................................... 144 List of Tables Table A: Project milestones.............................................................................................. -

Park View, Fauldhouse, Bathgate, West Lothian Offers Over £120,000
Park View, Fauldhouse, Bathgate, West Lothian Offers Over £120,000 Park View, Fauldhouse, Property Description Our View This is a well proportioned semi-detached villa set This is your chance to purchase this semi-detached Bathgate, West Lothian within large garden ground. The spacious accommodation villa which is in good order throughout. We strongly comprises: entrance hall, bright and sunny lounge with recommend viewing at your earliest convenience to feature fireplace with multi fuel burner, modern fitted appreciate what is on offer. Offers Over £120,000 kitchen with base and wall mounted units with integrated oven, hob and hood and there are French doors leading out to the rear. This floor is completed by the tiled shower Location room. On the upper level there are 3 good sized bedrooms Fauldhouse is a small village but benefits from a train and (all of which have built-in storage facilities) and the family bus station servicing both Edinburgh and Glasgow. This bathroom with WC, wash hand basin and bath. Externally property is well placed for access to all local amenities there is large garden ground to the front, side and rear including the Fauldhouse Partnership Centre and both which has been laid mostly to lawn with flower boarders. nursery and schooling facilities. There are good transport There is also a chipped driveway to the rear and a large links and access to the M8/M9 motorway are close by. shed area. The property comes complete with gas central heating and double glazing. EPC Rating = Band C. EPC = C For full EPC please contact the branch IMPORTANT NOTE TO PURCHASERS: We endeavour to make our sales particulars accurate and reliable, however, they do not constitute or form part of an offer or any contract and none is to be relied upon as statements of representation or fact. -

The Edinburgh Gazette, May 23, 1950
242 THE EDINBURGH GAZETTE, MAY 23, 1950. Leszcznk, Piotr Fawel (known as Peter Paul Leszczuk); Wolczek, Wladyslaw (known as Wladek Wolczek); Poland; Poland; Chemist; 9 Cherrybank, Dnnfermline, Fife. 14th Mechanic (Motors); Ard Beath, Pitlessie, by Ladybank, March 1950. Fife. 27th March 1950. Link, Wlpdzimierz Jozef; Poland; Student (Electrical Wolff, Else Fanny. See Dobrowolska, Else Fanny. Engineering); 30 Shamrock Street, Dundee. 17th April Zielinski, Stanislaw; Poland; Poultry Farmer; Sommerville 1950. Park, East Hemming Street, Letham, Angus. 14th April Lnbinski, Leonard; Poland; Coal Miner; 46 Sutherland 1950. Street, Kirkcaldy, Fife. 24th March 1950. Zotto, Alberto Edoardo del; Italy; Terrazzo Worker; 104 Ludwig, Richard. See Ludwig, Ryszzard Bartlomiej. The Oval, Stamperland, Clarkston, Renfrewshire. 22nd Ludwig, Ryszard Bartlomiej (known as Richard Ludwig); March 1950. Poland; Student Teacher; 7 Abbotsford Place, Dundee. 16th March 1950. Marczewski, Stanislaw; Poland; Mushroom Grower; 71 Jessie Street, Blairgowrie, Perthshire. 21st March 1950. Markowski, Edmund Stanislaw; Poland; Engineer; Hostel of Messrs. A. M. M. B. U. Limited, Kinnell, by Arbroath, POST OFFICE TELEPHONES. Adfus.. 29th March 1950. Matlacz, Eugeniusz; Poland; Labourer; 3 Yew Terrace, His Majesty's Postmaster-General hereby gives notice that Westquarter, by Falkirk, Stirlingshire. 12th April 1950. a telephone service between the United Kingdom, the Isle of Michaluuio, Tadeusz Stanislaw; Poland; Watch and Clock Man, and the Channel Isles, on the one hand and the Federa- Repairer; West Kinnaird Cottage, Pitlochry, Perthshire. tion of Malaya and Singapore on the other hand will be 16th March 1950. opened on the 22nd day of May 1950, and will be available Modlinski, Leon; Poland; Operative (Paper Mill); 18 from 9 a.m. -

Community Council Office Bearers – Revised May 2017
COMMUNITY COUNCIL OFFICE BEARERS – REVISED MAY 2017 For further information about Community Councils in West Lothian please visit www.westlothian.gov.uk/communitycouncils ADDIEWELL & LOGANLEA COMMUNITY COUNCIL FAULDHOUSE & THE BREICH VALLEY WARD Chair Vice Chair Treasurer Secretary Fiona Duncan David Fitzcharles Lesley Martin Anne Walsh 14 Ross Court Hawthorn Cottage Elm Cottage, Muirhall 8 Faraday Place Addiewell Muirhall Addiewell Addiewell West Lothian Addiewell West Lothian West Lothian EH55 8HE EH55 8NL EH55 8NL EH55 8NG 01501 763839 [email protected] ARMADALE COMMUNITY COUNCIL ARMADALE & BLACKRDIGE WARD Chair Vice Chair Treasurer Secretary John McKee John Watson Alison Muir Hugh Cockburn 28 Glenside Gardens 16 Millburn Crescent 2 Baird Road c/o 28 Glenside Gardens Armadale Armadale Armadale Armadale West Lothian West Lothian West Lothian West Lothian EH48 3RA EH48 3RB EH48 3 EH48 3RE 07743 672 092 07801 792 917 [email protected] [email protected] 15/5/2017 BATHGATE COMMUNITY COUNCIL BATHGATE WARD Chair Vice Chair Treasurer Secretary Ronald MacLeod Billy Johnston Donald Stavert Debbie Halloran 11 Inch Crescent 3 Avon Road 43 Bruce Street 71 Cardross Avenue Bathgate Bathgate Bathgate Broxburn West Lothian West Lothian West Lothian West Lothian EH48 1EU EH48 4HP EH48 2TJ EH52 6HD 01506 630914 07841 700 074 [email protected] [email protected] BELLSQUARRY & ADAMBRAE COMMUNITY COUNCIL LIVINGSTON SOUTH WARD Chair Vice Chair Treasurer Secretary Kenneth Logan Jill Wilkie James Wilkie Christine -

Fauldhouse and Breich Valley Together Issue 45
The Hub closed, staff remote working Fauldhouseand Breich Valley Together The Hub may be closed but F&BV CDT is still supporting Fauldhouse and the Breich Valley communities through difficult times Issue 45, Spring 2020 Fantastic response to lock down across Fauldhouse and Breich Valley communities There have been so many good things happening within the Fauldhouse and Breich Valley communities during these unprecedented times. F&BV CDT thought it would be helpful to produce a small extra edition of the F&BV Together newsletter, to keep everyone up to date, share information within our communities about the work of F&BV CDT and a range of other community led/local groups and projects. We also want to highlight some of the ways local people are pulling together during these hugely challenging times to support their communities: And to say thank you to everyone for their hard work and commitment. F&BV CDT believe, like many others within our communities, that by pulling together (as active local communities) and helping each other, we will get Useful contacts through this terrible crisis. There are local action groups (some outlined F&BV CDT have compiled a list within this newsletter) and generous local people who are volunteering their of local and West Lothian wide time, skills and energy to help us all prepare. Volunteers are also delivering useful numbers should you, or precooked meals food parcels, prescriptions, shopping and much more. anyone you know, need help, The communities of F&BV are (primarily) ex mining communities. Historically advice or support. You can our communities have shown that we have the resilience, commitment and call F&BV CDT directly or you knowledge required to ensure we can tackle the problems we know our can call one of the numbers communities will face when the full impact of the current crisis hits.