Developing Nova Scotian Community Clusters for Health Service Planning and Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dartmouth Assessment of Street Involved Population Using an Evidence-Based Framework
Dartmouth Assessment of street involved population using an evidence-based framework October 2018 Objective What are the needs of the street involved population in Dartmouth? Does Dartmouth need a shelter/crisis centre? This research has been initiated to apply an evidence- based rationale for addressing the needs of street involved populations in the community of Dartmouth, Nova Scotia Produced by: Affordable Housing Association of Nova Scotia Claudia Jahn- Program Director David Harrison, MCIP-Researcher Charlene Gagnon- Researcher Methodology A framework for moving forward • Literature review • Statistical Data Scan • Stakeholder interviews • Homeless Surveys Literature Review Harm Reduction in Dartmouth North: The Highfield/Pinecrest Neighbourhood planning for addiction, April 2018 Housing Initiative: A Working Proposal, September 2016 Housing Trilogy, Dartmouth North Report, November 2017 Click here to access analysis and report including tables. “Report #3: Summary of Dartmouth North Studies” Statistics Data review and analysis A review and analysis of available, relevant data was conducted. Report #1 provides information on housing and income variables for the federal riding of Dartmouth-Cole Harbour. Statistics Canada 2016 census information was used to create a profile of housing and income factors for Dartmouth-Cole Harbour. Data sub-sets were generated to help highlight geographical areas and populations at- risk of homelessness; and other determinants, for example, housing and income factors that may have a bearing on affordable housing. Best efforts were made to compile data at the Provincial riding level. Click here to access analysis and report including tables. “Report #1: Housing and Income Indicators” All three levels of government are increasingly involved in addressing affordable housing and homelessness. -

Supplement to the Public Accounts 7
SUPPLEMENT TO THE PUBLIC ACCOUNTS 7 Agriculture and Marketing — (Continued) Trueman, Brian C........................... 1,115 95 Accounts Payable Adjustment .... 28,597 71 Walsh, Frederick A........................... 2,160 55 Less Recoveries ................................ 1^19 95 Wilson, Harold G.............................. 1,782 96 Accounts under $1,000 ................... 27,953 75 $ 283,673 32 Dykv.land Rehabilitation : Advocate Marsh Body ...................$ 1,137 25 Accounts under $1,000 ......... .. 2,632 64 Grand Prc Marsh Body ................. 10,876 17 Accounts Payable Adjustment ..... 1,256 54 Minudic Marsh Body .................... 2,329 85 Less Recoveries ........................... 3,010 70 Truro Dykcland Park Marsh Body 1,136 75 Wellington Marsh Body ............ 1,879 50 $ 18.238 00 Cumin to Societies and Organizations ; Agricultural Economic Research N. S. Mink Breeder’s Association 1,000 00 Council of Canada ....................$ 2,500 00 N. S. Poultry Council .................... 1,000 00 Annapolis Co. Exhibition ......... .... 2,500 00 N. S. Provincial Exhibition ........... 4,000 00 Atlantic Winter Fair ..................... 8,000 00 N. S. Society for Prevention of Canadian Council on 4-H Clubs .... 1,517 00 Cruelty to Animals ................. 1,000 00 Cape Breton Co. Exhibition ......... 2,500 00 Western N. S. Exhibition ........... 2,500 00 Central N. S. Holstein Club .... 1,400 00 Pictou Co. Exhibition .................. 2,500 00 Cumberland Co. Exhibition 2,500 00 Queens Co. Exhibition ................. 1,000 00 Digby Co. Exhibition .................... 1,000 00 Royal Winter Fair .......................... 1,000 00 Eastern N. S. Exhibition .... 2,500 00 Shelburne Co. Exhibition ........... 1,000 00 Halifax Co. Exhibition .... 1,000 00 South Shore Exhibition ............. 4,000 00 Hants Co. Exhibition .................... 4,000 00 Weed Control Act Expenses .......... -

PC Candidate
Political Contributions Regime Annual Report, January 1, 2016 to December 31, 2016 Disclosure Statement of Registered Canddiates: The Progressive Conservative Association of Nova Scotia 01 Annapolis No registered candidate 02 Antigonish Candidate: Ray Mattie Official Agent: Rachel MacDonald Date Filed: march 29 2017 Contributions: NIL Last Name of Individual First Name Community Amount ($) Total of all contributions $200 or less Total NIL 03 Argyle-Barrington No registered candidate 04 Bedford Candidate: Valerie White Official Agent: Sandy Stevens Date Filed: March 16 2017 Contributions: NIL Last Name of Individual First Name Community Amount ($) Total of all contributions $200 or less Total NIL 05 Cape Breton Centre No registered candidate 06 Cape Breton-Richmond No registered candidate 07 Chester-St. Margaret’s No registered candidate 08 Clare-Digby No registered candidate 09 Clayton Park West Candidate: Paul Kimball Official Agent: Len MacKeigan Date Filed: March 16 2017 Contributions: NIL Last Name of Individual First Name Community Amount ($) Total of all contributions $200 or less Total NIL 10 Colchester-Musquodoboit Valley Candidate: William Harrison Official Agent: Penny Gilbert Date Filed: March 24 2017 Contributions: NIL Last Name of Individual First Name Community Amount ($) Total of all contributions $200 or less Total NIL 11 Colchester North No registered candidate Disclosure Statement of Registered Candidates: The Progressive Conservative Association of Nova Scotia, Continued 12 Cole Harbour-Eastern Passage Candidate: Barbara -

Electoral District of Halifax Chebucto
Map 1 of 1 28 - Electoral District of Halifax Chebucto 30 - Halifax Needham 2 6 - H a l i f a x A r m d a l e Windsor St Hood St 30 - Stanbury St 28 - HalifaxH Chebucto al Claremont St ifa x N e e Warren St d 28 - Halifax Chebucto h a 2 m 6 - H a l i f Wolfe Cres a x Maxwell Ave A t r S m ey Ashton Ln dl d u a D l e Connolly St es Cr re efi m Ho Windsor St 030 Hawk Terr Dr ne re sca Ma L a u r ie Hemp Rope Ln D r Barracks Dr Macdougall St Watch Dog Watch Rd Windsor St 30 - Halifax Needham 2 8 Connolly St - H a lif Chester Ave ax Edgewood Ave Cloverdale Rd C Bayers Rd 022 h eb uc Young St to Oxford St Beresford Rd Cork St 029 Connaught Ave Glendale Rd Liverpool St Dublin St t Roslyn Rd S n do on 023 L W in rr ds Te or t S s t re c d Deacon St in Edinburgh St W d R rs ye Ba Almon St Young St 021 Connolly St 024 Summit St Cork St Connaught Ave Liverpool St 020 Dublin St London St Charles St Ll ham oy 026 Need d Willow St fax F ali o - H x St Matthias St 0 A 3 ve Berlin St 28 - Halifax Chebucto Edinburgh St 019 o Vienna St Seaforth St North St t c G Oxford St u e b o rg e e St h D n W C a o Compton Ave u lm in x p h A d a i Connolly St s f n o i e l r e S a A t H ve - 8 26 - Halifax Armdale 025 2 Summit St 017 018 Chebucto Rd Williams St Duncan St R o Jack b Fer i guss e on Ave Welsford St S Edward Arab Ave t 028 015 Chebucto Ln Lawrence St Swaine St Connaught Ave Parker St R a d l n p 031 la h s D # I e le v Allan St b Robert li a n S D l- e D r d o a e u M it v g u C M Winston Pl S r x u A m p 027 30 - Halifaxa Needham m h if e i y 016 -

Dartmouth South (2013) Electoral History for Dartmouth South (2013)
Electoral History for Dartmouth South (2013) Electoral History for Dartmouth South (2013) Including Former Electoral District Names Report Created for by the Nova Scotia Legislative Library The returns as presented here are not official. Every effort has been made to make these results as accurate as possible. Return information was compiled from official electoral return reports and from newspapers of the day. The number of votes is listed as 0 if there is no information or the candidate won by acclamation. Wednesday, June 14, 2017 Page 1 of 34 Electoral History for Dartmouth South (2013) Dartmouth South (2013) In 2013 following the recommendations of the 2012 Electoral Boundaries Commission, this district was renamed from Dartmouth South-Portland Valley and lost the area south of Russell Lake and east of Highway 111 to Cole Harbour-Eastern Passage. Member Elected Election Date Party Elected Chender, Claudia 30-May-2017 New Democratic Party Majority: (197) Candidate Party Votes Chender, ClaudiaNew Democratic Party 3545 Bhardwaj, VishalLiberal 3348 Crnogorac, JadIndependent 1418 Trenholm, JuneGreen Party 506 Murray, James Anthony (Jim)Atlantica 123 Jad Crnogorac was removed from the Progressive Conservative slate of candidates prior to the election. Because she was dropped too late for changes to be made to the ballot, she appeared as PC candidate. Mancini, Marian 14-Jul-2015 (By-election) New Democratic Party Majority: (88) Candidate Party Votes Mancini, MarianNew Democratic Party 2274 Rissesco, Timothy WayneLiberal 2186 Gamble, Gord -
Development of Heritage Properties Within South End Secondary Plan Area of Halifax Peninsula
P.O. Box 1749 Halifax, Nova Scotia B3J 3A5 Canada Item No. 11.5.1 Halifax Regional Council February 23, 2021 TO: Mayor Savage and Members of Halifax Regional Council Original Signed SUBMITTED BY: For Jenny Lugar, Chair, Heritage Advisory Committee DATE: February 2, 2021 SUBJECT: Case H00500: Development of Heritage Properties within South End Secondary Plan Area of Halifax Peninsula ORIGIN January 27, 2021 special meeting of the Heritage Advisory Committee, Item 9.1.4. LEGISLATIVE AUTHORITY Heritage Property Act, R.S.N.S. 1989, c. 199 Heritage Conservation Districts Regulations By-law H-200, Heritage Property By-law RECOMMENDATION It is recommended that Halifax Regional Council direct the Chief Administrative Officer to identify additional heritage conservation district study areas within the South End Secondary Plan Area, as per Option 3 of the December 22, 2020 report, for potential inclusion in the Regional Centre Secondary Municipal Planning Strategy. BACKGROUND The Heritage Advisory Committee received a staff recommendation report dated December 22, 2020, at their January 27, 2021 special meeting respecting Case H00500. For further information on the background of this item, refer to the staff report dated December 22, 2020. DISCUSSION The Heritage Advisory Committee reviewed the December 22, 2020 staff report, and received a staff presentation at their January 27, 2021 special meeting. Following a discussion of the item, the Committee approved the recommendation as outlined in the “Recommendation” portion of this report. For further discussion on this item, refer to the staff report dated December 22, 2020. H00500: Development within Heritage Properties in the South End Council Report - 2 - February 23, 2021 FINANCIAL IMPLICATIONS Refer to the staff report dated December 22, 2020. -

October 8, 2013 Nova Scotia Provincial General
47.1° N 59.2° W Cape Dauphin Point Aconi Sackville-Beaver Bank Middle Sackville Windsor μ Alder Junction Point Sackville-Cobequid Waverley Bay St. Lawrence Lower Meat Cove Capstick Sackville Florence Bras d'Or Waverley- North Preston New Waterford Hammonds Plains- Fall River- Lake Echo Aspy Bay Sydney Mines Dingwall Lucasville Beaver Bank Lingan Cape North Dartmouth White Point South Harbour Bedford East Cape Breton Centre Red River Big Intervale Hammonds Plains Cape North Preston-Dartmouth Pleasant Bay Bedford North Neils Harbour Sydney Preston Gardiner Mines Glace Bay Dartmouth North South Bar Glace Bay Burnside Donkin Ingonish Minesville Reserve Mines Ingonish Beach Petit Étang Ingonish Chéticamp Ferry Upper Marconi Lawrencetown La Pointe Northside- Towers Belle-Marche Clayton Cole Point Cross Victoria-The Lakes Westmount Whitney Pier Park Dartmouth Harbour- Halifax Sydney- Grand Lake Road Grand Étang Wreck Cove St. Joseph Leitches Creek du Moine West Portland Valley Eastern Shore Whitney Timberlea Needham Westmount French River Fairview- Port Morien Cap Le Moine Dartmouth Pier Cole Balls Creek Birch Grove Clayton Harbour Breton Cove South Sydney Belle Côte Kingross Park Halifax ^ Halifax Margaree Harbour North Shore Portree Chebucto Margaree Chimney Corner Beechville Halifax Citadel- Indian Brook Margaree Valley Tarbotvale Margaree Centre See CBRM Inset Halifax Armdale Cole Harbour-Eastern Passage St. Rose River Bennet Cape Dauphin Sable Island Point Aconi Cow Bay Sydney River Mira Road Sydney River-Mira-Louisbourg Margaree Forks Egypt Road North River BridgeJersey Cove Homeville Alder Point North East Margaree Dunvegan Englishtown Big Bras d'Or Florence Quarry St. Anns Eastern Passage South West Margaree Broad Cove Sydney New Waterford Bras d'Or Chapel MacLeods Point Mines Lingan Timberlea-Prospect Gold Brook St. -

Fairview-Clayton Park Electoral History for Fairview-Clayton Park
Electoral History for Fairview-Clayton Park Electoral History for Fairview-Clayton Park Including Former Electoral District Names Report Created for Nova Scotia Legislature Website by the Nova Scotia Legislative Library The returns as presented here are not official. Every effort has been made to make these results as accurate as possible. Return information was compiled from official electoral return reports and from newspapers of the day. The number of votes is listed as 0 if there is no information or the candidate won by acclamation. September 1, 2021 Page 1 of 44 Electoral History for Fairview-Clayton Park Fairview-Clayton Park In 2013, following the recommendation of the Electoral Boundaries Commission, this district was created by merging the area north of Bayers Road and west of Connaught Avenue from Halifax Chebucto; the area south of Mount St Vincent University and Lacewood Drive as well as the Washmill Drive area from Halifax Clayton Park; and the area north of Highway 102 and east of Northwest Arm Drive / Dunbrack street from Halifax Fairview. In 2021, the district lost that portion east of Joseph Howe Drive and Elliot Street to Connaught Avenue to Halifax Armdale. Member Elected Election Date Party Elected Arab, Patricia Anne 17-Aug-2021 Liberal Majority: (105) Candidate Party Votes Arab, Patricia Liberal 2892 Hussey, Joanne New Democratic Party 2787 Mosher, Nicole Progressive Conservative 1678 Richardson, Sheila G. Green Party 153 Arab, Patricia Anne 30-May-2017 Liberal Majority: (735) Candidate Party Votes Arab, Patricia -

Nova Scotia Greens Email Contacts (Current to 2021-02-21)
Nova Scotia Greens Email contacts (Current to 2021-02-21) General General contact address [email protected] Contact point for prospective candidates [email protected] Contact point for media [email protected] Leadership Leader Thomas Trappenberg [email protected] Deputy Leader Jessica Alexander [email protected] Officers President (term ending 2021) Ashley Morton [email protected] President (term ending 2022) Judy N Green [email protected] Governance Director Emanuel Jannasch [email protected] Membership Director Bill Matheson [email protected] Finance Director Keith Towse [email protected] Policy Convenor (term ending 2021) Anthony Edmonds [email protected] Policy Convenor (term ending 2022) Carolyn Marshall [email protected] Other Roles Communications Chair Michael Uhlarik [email protected] Official Agent Keith Towse [email protected] Committees & Groups Executive [email protected] Financial Committee [email protected] Human Resources Working Group [email protected] Officer Elections Team [email protected] Policy Committee [email protected] Provincial Nominations Committee [email protected] Points of Contact - Regions Bedford Basin Convenor Laura Eamon [email protected] Bedford Basin Regional Committee mailing list [email protected] Dartmouth Convenor June Trenholm [email protected] -

NS Royal Gazette Part I
Nova Scotia Published by Authority PART 1 VOLUME 220, NO. 6 HALIFAX, NOVA SCOTIA, WEDNESDAY, FEBRUARY 9, 2011 NOTICE TO CREDITORS, HEIRS AND Lynn Knockwood and Michael Halliday OTHER CLAIMANTS Signatures of Co-Executors In the Matter of the Indian Act, R.S.C., CH. 1-5 and 290 February 9-2011 - (8iss) amendments thereto, and in the Matter of the Estate of Janis Maria Walker, registration number 0300004801 PROVINCE OF NOVA SCOTIA of the Glooscap First Nation, deceased, who died on or DEPARTMENT OF JUSTICE about the 19th day of September, 2010, in the Province of Nova Scotia, and who at the time of death had been The Minister of Justice and Attorney General, Ross ordinarily resident of Glooscap. Landry, under the authority vested in him by clause 2(b) of Chapter 23 of the Acts of 1996, the Court and NOTICE is hereby given pursuant to Section 8 of the Administrative Reform Act, Order in Council 2004-84, the Indian Estates Regulations; Assignment of Authority Regulations, and Sections 6 and 7 of Chapter 312 of the Revised Statutes of Nova Scotia, THAT ALL CREDITORS, heirs and other claimants 1989, the Notaries and Commissioners Act, is hereby having demands or claims against the estate of Janis pleased to advise of the following: Maria Walker, who died on or about the 19th day of September, 2010, are required to produce on or before To be revoked as a Commissioner pursuant to the April 6th, 2011 to: Notaries and Commissioners Act: Valerie Britten of Sydney, in the County of Cape Lynn Knockwood Breton (no longer employed with Citizenship and PO Box 346 Immigration Canada). -

Banks & Depository Institutions
SECTION 1 Banks & Depository Institutions Included in this section: • Domestic Banks: Schedule I...................................................3 • Foreign Banks: Schedule II..................................................144 • Foreign Bank Branches: Schedule III ..........................................150 • Foreign Bank Representative Offices..........................................153 • Savings Banks ...........................................................154 • Trust Companies..........................................................161 • Credit Unions/Caisses Populaires ............................................166 Chartered banks in Canada are incorporated by letters patent. They are governed by the Bank Act, which establishes the legislative framework for Canada’s banking system. The Bank Act pro- vides for the incorporation of banks. The Office of the Superintendent of Financial Insitutions Can- ada regulates and supervises the Canadian financial system. Domestic Banks, are federally regulated Canadian banks. The subsidiaries of Foreign Banks are federally regulated foreign banks. Both domestic and foreign banks have the same powers, restrictions and obligations under the Bank Act. Foreign Bank Branches are federally regulated foreign bank branches. They are permitted to establish specialized, commercially focused branches in Canada, in accordance with the Bank Act. Full service branches generally are not permitted to accept deposits of less than $150,000. Foreign Bank Representative Offices are established by foreign -
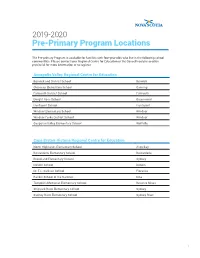
2019-2020 Pre-Primary Program Locations
2019-2020 Pre-Primary Program Locations The Pre-primary Program is available for families with four-year-olds who live in the following school communities. Please contact your Regional Centre for Education or the Conseil scolaire acadien provincial for more information or to register. Annapolis Valley Regional Centre for Education Berwick and District School Berwick Glooscap Elementary School Canning Falmouth District School Falmouth Dwight Ross School Greenwood Hantsport School Hantsport Windsor Elementary School Windsor Windsor Forks District School Windsor Gasperau Valley Elementary School Wolfville Cape Breton-Victoria Regional Centre for Education North Highlands Elementary School Aspy Bay Boularderie Elementary School Boularderie Brookland Elementary School Sydney Donkin School Donkin Dr. T.L. Sullivan School Florence Rankin School of the Narrows Iona Tompkins Memorial Elementary School Reserve Mines Shipyard River Elementary School Sydney Sydney River Elementary School Sydney River 1 Chignecto-Central Regional Centre for Education West Colchester Consolidated School Bass River Cumberland North Academy Brookdale Great Village Elementary School Great Village Uniacke District School Mount Uniacke A.G. Baillie Memorial School New Glasgow Cobequid District Elementary School Noel Parrsboro Regional Elementary School Parrsboro Salt Springs Elementary School Pictou West Pictou Consolidated School Pictou Scotsburn Elementary School Scotsburn Tatamagouche Elementary School Tatamagouche Halifax Regional Centre for Education Sunnyside Elementary School Bedford Alderney Elementary School Dartmouth Caldwell Road Elementary School Dartmouth Hawthorn Elementary School Dartmouth John MacNeil Elementary School Dartmouth Mount Edward Elementary School Dartmouth Robert K. Turner Elementary School Dartmouth Tallahassee Community School Eastern Passage Oldfield Consolidated School Enfield Burton Ettinger Elementary School Halifax Duc d’Anville Elementary School Halifax Elizabeth Sutherland Halifax LeMarchant-St.