(Wisdom Tooth) Extraction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Different Types of Flaps in the Surgical Relations of the Third
tist Blanco et al., Dentistry 2017, 7:4 Den ry DOI: 10.4172/2161-1122.1000425 Dentistry ISSN: 2161-1122 Review Article Open Access The Different Types of Flaps in the Surgical Relations of the Third Impacted Molars–Literature Review Guillermo Blanco*, Dianorys Lora and Clovys Marzola Dentistry University Foundation, Hospital Heli Moreno Blanco, Brazil Abstract Third molars can present themselves completely and or partially retained and may be mucosal, submucosal, or completely retained within the jaws or jaw. The surgical technique includes an incision type, playing a key role in wound healing, presenting a series of incisions described over time, by different researchers and authors, in an attempt to minimize their impact, employ professional judgment one according to your needs and convenience. Keywords: Third molar; Impaction; Flap design To Nageshwar, The incision should not be performed on bone defects, or cut the muscle or tendon, the incisions should not be Introduction very long, and they could influence the unfortunate consequences of The impacted third molar surgery and/or partially impacted is extraction [123]. the most common procedure in oral surgery and maxillofacial [1-18], The flap design according Karaca et al., used during surgery for ranging from therapeutic indications, previous history of infection removal of impacted third molars prevents complications related to [19-22] periodontal disease [23], pericoronitís [30-33],operating an 2 molar periodontal status [125]. Suarez et al. believe that this design inexplicable [34] pain associated with the third molar [35-36], pain, influences healing primary [122]. This prevents wound dehiscence and intractable caries prevention caries [37-43], tooth root resorption evaluated the suture technique to achieve this closure to Sanchis et al. -

Tooth Size Proportions Useful in Early Diagnosis
#63 Ortho-Tain, Inc. 1-800-541-6612 Tooth Size Proportions Useful In Early Diagnosis As the permanent incisors begin to erupt starting with the lower central, it becomes helpful to predict the sizes of the other upper and lower adult incisors to determine the required space necessary for straightness. Although there are variations in the mesio-distal widths of the teeth in any individual when proportions are used, the sizes of the unerupted permanent teeth can at least be fairly accurately pre-determined from the mesio-distal measurements obtained from the measurements of already erupted permanent teeth. As the mandibular permanent central breaks tissue, a mesio-distal measurement of the tooth is taken. The size of the lower adult lateral is obtained by adding 0.5 mm.. to the lower central size (see a). (a) Width of lower lateral = m-d width of lower central + 0.5 mm. The sizes of the upper incisors then become important as well. The upper permanent central is 3.25 mm.. wider than the lower central (see b). (b) Size of upper central = m-d width of lower central + 3.25 mm. The size of the upper lateral is 2.0 mm. smaller mesio-distally than the maxillary central (see c), and 1.25 mm. larger than the lower central (see d). (c) Size of upper lateral = m-d width of upper central - 2.0 mm. (d) Size of upper lateral = m-d width of lower central + 1.25 mm. The combined mesio-distal widths of the lower four adult incisors are four times the width of the mandibular central plus 1.0 mm. -

Bone Induction of Human Tooth and Bone Crushed by Newly Developed Automatic Mill
Journal of the Ceramic Society of Japan 118 [6] 434-437 2010 Paper Bone induction of human tooth and bone crushed by newly developed automatic mill Masaru MURATA,³ Toshiyuki AKAZAWA,* Masahiko TAKAHATA,** Manabu ITO,** Junichi TAZAKI,*** Jun HINO,*** Katsuo NAKAMURA,* Norimasa IWASAKI,** Takanori SHIBATA*** and Makoto ARISUE Oral and Maxillofacial Surgery, School of Dentistry, Health Sciences University of Hokkaido, 1757 Kanazawa, Tobetsu, Hokkaido 061–0293 *Materials Technology, Hokkaido Industrial Research Institute, Kita 19 Nishi 11, Kita-ku, Sapporo, Hokkaido 060–0819 **Orthopaedic Surgery, Hokkaido University Graduate School of Medicine, Kita 14 Nishi 7, Kita-ku, Sapporo, Hokkaido 060–8586 ***Reconstructive Surgery for Oral and Maxillofacial Region, School of Dentistry, Health Sciences University of Hokkaido, 1757 Kanazawa, Tobetsu, Hokkaido 061-0293 A novel automaticmill of teeth and bone has been developed for bone engineering. A human frozen-tooth and/or a human frozen-bone block were put into the Zirconium oxide (ZrO2) ceramics vessel of the machine, and crushed for 1 minwith 20 saline- 3 ice blocks (1 © 1 © 1cm /block) at 12000 rpm of ZrO2 blade. The crushed granules were demineralized completely in2% HNO3 solution for 20 min, and rinsed incoldsaline. We named each biomaterial after the acid treatment and washing, demineralized dentin matrices (DDM), demineralized bone matrices (DBM). Five wisdom teeth (total wet volume: 10.0 g) were crushed, decalcified, and lyophilized. The distribution offreeze-dried DDM granules was fine granules (0.51.0 mm: 0.27 g), moderate (1.02.0 mm: 0.46 g), and large (2.05.0 mm: 0.64 g). The fine granules of human DDM or DBM were implanted into the subcutaneous tissue of 4 week-old nude mice, and theirtissue-inductive properties were estimated at 4 weeks after implantation histologically. -

Third Molar (Wisdom) Teeth
Third molar (wisdom) teeth This information leaflet is for patients who may need to have their third molar (wisdom) teeth removed. It explains why they may need to be removed, what is involved and any risks or complications that there may be. Please take the opportunity to read this leaflet before seeing the surgeon for consultation. The surgeon will explain what treatment is required for you and how these issues may affect you. They will also answer any of your questions. What are wisdom teeth? Third molar (wisdom) teeth are the last teeth to erupt into the mouth. People will normally develop four wisdom teeth: two on each side of the mouth, one on the bottom jaw and one on the top jaw. These would normally erupt between the ages of 18-24 years. Some people can develop less than four wisdom teeth and, occasionally, others can develop more than four. A wisdom tooth can fail to erupt properly into the mouth and can become stuck, either under the gum, or as it pushes through the gum – this is referred to as an impacted wisdom tooth. Sometimes the wisdom tooth will not become impacted and will erupt and function normally. Both impacted and non-impacted wisdom teeth can cause problems for people. Some of these problems can cause symptoms such as pain & swelling, however other wisdom teeth may have no symptoms at all but will still cause problems in the mouth. People often develop problems soon after their wisdom teeth erupt but others may not cause problems until later on in life. -

The Australian Schedule of Dental Services and Glossary
The Australian Schedule of Dental Services and Glossary Twelfth Edition The Australian Schedule of Dental Services and Glossary Australian Dental Association Twelfth Edition Published by the Australian Dental Association 12–14 Chandos St, St Leonards, NSW 2065 Australia © Australian Dental Association, 2017 First published 1986 An Australian Glossary of Dental Terms Second Edition 1990 An Australian Glossary of Dental Terms Third Edition 1992 An Australian Glossary of Dental Terms Fourth Edition 1994 An Australian Glossary of Dental Terms Fifth Edition 1996 An Australian Schedule of Dental Services and Glossary Sixth Edition 2000 An Australian Schedule of Dental Services and Glossary Seventh Edition 2002 The Australian Schedule of Dental Services and Glossary Eighth Edition 2004 The Australian Schedule of Dental Services and Glossary Ninth Edition 2009 The Australian Schedule of Dental Services and Glossary Tenth Edition 2013 The Australian Schedule of Dental Services and Glossary Eleventh Edition 2016 The Australian Schedule of Dental Services and Glossary Twelfth Edition 2017 The Australian Schedule of Dental Services and Glossary All rights reserved. No part of this work covered by copyright may be reproduced or copied in any form or by any means (graphic, electronic or mechanical, including photocopying, recording, taping, or information and retrieval systems) without the written permission of the publisher. ISBN 0 909961 31 X ii The Australian Schedule of Dental Services and Glossary Contents Twelfth Edition Updates vi Introduction -
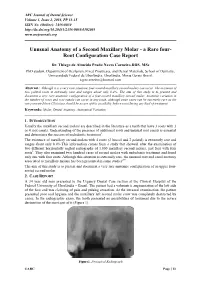
Unusual Anatomy of a Second Maxillary Molar - a Rare Four- Root Configuration Case Report
ARC Journal of Dental Science Volume 1, Issue 2, 2016, PP 13-15 ISSN No. (Online): 2456-0030 http://dx.doi.org/10.20431/2456-0030.0102003 www.arcjournals.org Unusual Anatomy of a Second Maxillary Molar - a Rare four- Root Configuration Case Report Dr. Thiago de Almeida Prado Naves Carneiro,DDS, MSc PhD student, Department of Occlusion, Fixed Prostheses, and Dental Materials, School of Dentistry, Universidade Federal de Uberlândia, Uberlândia, Minas Gerais Brazil. [email protected] Abstract: Although it is a very rare situation, four-rooted maxillary second molars can occur. The existence of two palatal roots is extremely rare and ranges about only 0.4%. The aim of this study is to present and document a very rare anatomic configuration of a four-rooted maxillary second molar. Anatomic variation in the number of roots and root canals can occur in any tooth, although some cases can be extremely rare as the one presented here.Clinicians should be aware of this possibility before considering any kind of treatment. Keywords: Molar, Dental Anatomy, Anatomical Variation 1. INTRODUCTION Usually the maxillary second molars are described in the literature as a teeth that have 3 roots with 3 or 4 root canals. Understanding of the presence of additional roots and unusual root canals is essential and determines the success of endodontic treatment1. The existence of maxillary second molars with 4 roots (2 buccal and 2 palatal) is extremely rare and ranges about only 0.4%.This information comes from a study that showed, after the examination of two different horizontally angled radiographs of 1,000 maxillary second molars, just four with four roots2. -

Two Sets of Teeth in a Lifetime
Two sets of teeth in a lifetime Two sets of teeth in a lifetime Deciduous teeth: They are the first set of teeth we have and there are altogether 20 of them. They usually start to erupt from around the age of six months until 3 years of age. Permanent teeth: At the age of 6, they sequentially erupt to replace the deciduous teeth which become loose and shed. Deciduous teeth: Space retainer for permanent teeth Normally, underneath the root of each deciduous tooth, there is a developing permanent successor tooth. When it is time for the permanent successor tooth to erupt, the root of the deciduous tooth will resorb and the deciduous tooth will become loose. The place is then taken up by its permanent successor tooth. Deciduous tooth retains the space for its permanent successor tooth. No tooth is dispensable If the deciduous tooth, especially the second deciduous molar, is lost early due to tooth decay, the consequences can be serious: Poor alignment of the teeth The second deciduous molar is already lost The first permanent molar Since the first permanent molar erupts behind the second deciduous molar at the age of 6, the space of the lost second deciduous molar will gradually close up as the first permanent molar moves forward. The permanent tooth is crowded out of the arch when it erupts Later, when the second permanent premolar erupts to replace the second deciduous molar, the permanent tooth will either be crowded out of the dental arch or be impacted and is unable to erupt, leading to poor alignment of the teeth. -

A Comparative Study of One Implant Versus Two Replacing a Single Molar Thomas J
JOMI on CD-ROM, 1996 Mar (372-378 ): A Comparative Study of One Implant Versus … Copyrights © 1997 Quinte… A Comparative Study of One Implant Versus Two Replacing a Single Molar Thomas J. Balshi, DDS, FACP/Ramon E. Hernandez, DMD/Maria Claudia Pryszlak, DMD/Bo Rangert, PhD, MechEng A comparative study between one and two Brånemark implants replacing a single molar was conducted. Forty-seven individuals comprised two groups of 22 patients treated with one implant and 25 with two implants. A total of 72 implants were placed, 66 (92%) in the mandible and six (8%) in the maxilla. After the first year of function, the success rate was 99%, with only one implant lost. Between the second- and third-year follow-ups, 100% of the implants continued to function in the remaining 46 patients, giving a 3-year cumulative success rate of 99%. The marginal bone loss between 1 and 3 years of function was 0.10 mm (SD 0.20) for the group with one implant and 0.24 mm (SD 0.20) for the group with two implants. No changes were observed in the Sulcus Bleeding Index during the 3-year follow-up. Prosthesis mobility or screw loosening was the most frequent complication and was predominant in the group using one implant (48%), but was substantially reduced in the group using two implants (8%). These mechanical problems, using one implant only, seem to be preventable using a stronger screw joint (CeraOne abutment). Precise centric occlusal contact was established and maintained over the study period, which was thought to contribute to the very high success rate for the single-implant-supported molars, despite their high degree of mechanical problems. -

Problems with Erupting Wisdom Teeth: Signs, Symptoms, and Management
Clinical Intelligence Tara Renton and Nairn H F Wilson Problems with erupting wisdom teeth: signs, symptoms, and management INTRODUCTION event of relatively short duration (3–4days) Many patients, in particular those with a fear associated with normal eruption. Improved of dentistry, or fear of the possible cost of local oral hygiene by toothbrushing with dental treatment, consult their GP when they toothpaste, interdental cleaning, or the use develop a dental problem, in particular dental of a chlorhexidine-containing mouthwash pain.1 A very common cause of dental pain is can reverse the symptoms. Paracetamol erupting wisdom teeth. This article presents or ibuprofen may be prescribed to relieve and describes the management of painful the pain. Analgesic tablets should always and infected erupting wisdom teeth. be swallowed. Under no circumstances should analgesic tablets be placed adjacent WISDOM TEETH to the pericoronitis; a relatively common, Wisdom teeth or third molars (M3s) are the ill-informed mistake by patients. If the last, most posteriorly placed permanent pain persists for more than 3–4days, or teeth to erupt. They usually erupt into the intensifies, a dentist should be consulted. If mouth between 17 and 25 years of age. the symptoms persist extraction of the tooth They can, however, erupt many years later. is recommended.2 Most adults have four M3s; however, 8% Acute spreading pericoronitis is an acute of the UK population have missing or no spreading infection, often stemming from a M3s.2 Mandibular M3s often get impacted in recurrence of acute pericoronitis. Surgical a partially erupted, non-functional position removal of the erupting M3 is preferred to (Figure 1). -
CHAPTER 5Morphology of Permanent Molars
CHAPTER Morphology of Permanent Molars Topics5 covered within the four sections of this chapter B. Type traits of maxillary molars from the lingual include the following: view I. Overview of molars C. Type traits of maxillary molars from the A. General description of molars proximal views B. Functions of molars D. Type traits of maxillary molars from the C. Class traits for molars occlusal view D. Arch traits that differentiate maxillary from IV. Maxillary and mandibular third molar type traits mandibular molars A. Type traits of all third molars (different from II. Type traits that differentiate mandibular second first and second molars) molars from mandibular first molars B. Size and shape of third molars A. Type traits of mandibular molars from the buc- C. Similarities and differences of third molar cal view crowns compared with first and second molars B. Type traits of mandibular molars from the in the same arch lingual view D. Similarities and differences of third molar roots C. Type traits of mandibular molars from the compared with first and second molars in the proximal views same arch D. Type traits of mandibular molars from the V. Interesting variations and ethnic differences in occlusal view molars III. Type traits that differentiate maxillary second molars from maxillary first molars A. Type traits of the maxillary first and second molars from the buccal view hroughout this chapter, “Appendix” followed Also, remember that statistics obtained from by a number and letter (e.g., Appendix 7a) is Dr. Woelfel’s original research on teeth have been used used within the text to denote reference to to draw conclusions throughout this chapter and are the page (number 7) and item (letter a) being referenced with superscript letters like this (dataA) that Treferred to on that appendix page. -

Mammalian Molar Complexity Follows Simple, Predictable Patterns
Mammalian molar complexity follows simple, predictable patterns Keegan R. Seliga,1, Waqqas Khalida, and Mary T. Silcoxa aDepartment of Anthropology, University of Toronto Scarborough, Toronto, ON M1C 1A4, Canada Edited by Nils Chr. Stenseth, University of Oslo, Oslo, Norway, and approved November 19, 2020 (received for review May 4, 2020) Identifying developmental explanations for the evolution of com- been demonstrated that there are strong genetic controls that plex structures like mammalian molars is fundamental to studying account for the developmental cascade, with research linking the phenotypic variation. Previous study showed that a “morphoge- ICM and the sonic hedgehog (Shh) gene, among others (10). It netic gradient” of molar proportions was explained by a balance should be noted that there are cases where the ICM does between inhibiting/activating activity from earlier developing mo- not seem to account for molar size covariation. For example, lars, termed the inhibitory cascade model (ICM). Although this Roseman and Delezene (11) found that gorillas do not meet any model provides an explanation for variation in molar proportions, of the predictions of the ICM, and Carter and Worthington (12) what remains poorly understood is if molar shape, or specifically demonstrate that some hominoids and cercopithecins do not complexity (i.e., the number of cusps, crests), can be explained by meet all of the predictions either. However, Evans et al. (2) also the same developmental model. Here, we show that molar com- analyzed the ICM in apes and hominids and considered both the plexity conforms to the ICM, following a linear, morphogenetic deciduous premolars and a reversal of the inhibitory cascade gradient along the molar row. -

Identifying Features
Permanent maxillary second molar Dental Anatomy .د ـــن ا Lec.Lec.12121212 Permanent maxillary second molar Principal identifying features: 1. No fifth cusp is evident. 2. Roots are less divergent and may coalescent. 3. Disto-buccal and mesio-buccal cusps are less developed. 4. The crown is smaller in all dimensions than max. first molar. Buccal aspect: 1. The crown is smaller in all dimensions than max. first molar. 2. The disto-buccal cusp is smaller and allows part of distal marginal ridge and part of disto-buccal cusp to be seen. 3. The buccal roots are about the same length. They are nearly parallel and more inclined distally more than that of max. first molar. 4. The palatal root is the longest root (about 1 mm longer than buccal roots). Lingual aspect: 1 Permanent maxillary second molar Dental Anatomy 1. The disto-lingual cusp is smaller than that of max. first molar. 2. No fifth cusp. 3. The apex of palatal root is in a line with disto-lingual cusp tip . Mesial aspect: 1. Bucco-lingual dimension is the same as that of max. first molar but the crown length is smaller. 2. The roots are less divergent bucco-lingually. Distal aspect: The disto-buccal cusp is smaller than that of max. first molar. Occlusal aspect: 1. The crown has rhomboidal shape, with the acute angles are less and the obtuse angles are more than that of max. first molar. 2. The bucco-lingual diameter is the same but the mesio-distal diameter is smaller by about 1 mm than that of max.