Trabecular Metal™ Reverse Shoulder System Surgical Technique
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WARD-DOCUMENT-2020.Pdf (1.324Mb)
3D Printing Impact on the Orthopedic Shoulder Replacement Global Supply Chain The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Ward, Abner. 2020. 3D Printing Impact on the Orthopedic Shoulder Replacement Global Supply Chain. Master's thesis, Harvard Extension School. Citable link https://nrs.harvard.edu/URN-3:HUL.INSTREPOS:37365004 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA 3D Printing Impact on the Orthopedic Shoulder Replacement Global Supply Chain Abner M. Ward, MD, MBA, FACS, FAAOS A Thesis in the Field of Biotechnology Management for the Degree of Master of Liberal Arts in Extension Studies Harvard University May 2020 Copyright 2020 [Abner Ward] Abstract The goal of this work was to investigate a novel new technology being used to improve total shoulder replacements in patients with difficult to treat anatomy. The new technology is the use of three-dimensional (3D) implant creations that can be tailored to a patient’s specific shoulder defects as opposed to shelf, standard size implants. The project will help provide management direction to improve the efficiency in the global supply system so that surgeons in various parts of the world may have access to surgical components in the shortest time without significant delay. The study findings were that hindrances to 3D adoption for just-in-time surgical usage primarily include difficulties with sterilization and lack of a global validation metric when performed at multiple international centers, as opposed to one location in a single country. -
Tailoring Series TECHNIQUES for TAILORING UNDERLINING a TAILORED GARMENT—Underlining Is a Second Layer of Fabric. It Is Cut By
tailoring series TECHNIQUES FOR TAILORING UNDERLINING A TAILORED GARMENT—Underlining is a second layer of fabric. It is cut by the garment pattern pieces and staystitched to the wrong side of the corresponding outer sections before any seams are joined. The two layers are then handled as one. As a general guide, most suit jackets and coats look more pro- fessional when underlined. Underlining is especially recommended for lightweight wool materials, loosely woven materials and light- colored materials. For additional information on selecting fabrics for underlining and applying the underlining, see Lining a Shirt 01' Dress HE 72, N. C. Agricultural Extension Service. STAYSTITCHING—Staystitch all outer garment pieces before construction begins. If garment is underlined, stays-titching is done when the two layers of fabric are sewn together. Staystitch 1/3 in. outside seamline (on the seam allowance). Stay- stitch “ with matching cotton thread on all curved *areas that may stretch during construction such as necklines, side seams, shoulder seams, armholes, and side seams of skirt. Use directional stitching always to prevent stretching of fabric and to prevent one layer of fabric from riding. The direction to stitch is indicated by small arrows on the pattern on the seamlines. INTERFACINGS—Select a high quality hair canvas for the front and collar of coats and jackets. The percentage of wool indicates the quality—the higher the wool content of the canvas the better the quality. Since a high percentage of wool makes the hair canvas fairly dark in color, it cannot be used successfully under light-colored fabrics. In these cases use an interfacing lighter in color and lower in wool content. -

That Was a T-Shirt!!! We Need Tops! While Cotton Tops Are Easy to Make, Knit Tops Are the Most Versatile Due to the Forgiving Stretch
That was a t-shirt!!! We need tops! While cotton tops are easy to make, knit tops are the most versatile due to the forgiving stretch. Because of the challenges in working with knit fabric, updating a t-shirt is the perfect compromise. Our goal is to have someone look at our top and say “that was a t-shirt?!” All hemlines need to be removed and restyled and the neckline needs to be either ruffled (size small and some medium) or trimmed. Here are some guidelines that we are looking for. Simply sewing a decorative stitch or zigzag over the existing hemline (sleeves and bottom hem) does not make visual changes to the t-shirt. Please cut off the existing hemline and if you like, you can make it shorter. If you have a serger, you can finish the edge prior to hemming but because the knit does not ravel it is not necessary. You also do not need to turn over the edge prior to hemming. Sleeves Match the sleeves and cut off both hems at the same time. You can cut straight or at an angle and make it a cap sleeve Use a decorative stitch for the hemming, variegated thread looks great! Use either white or black thread in the bottom as variegated thread is expensive. Remember to sew on the right side with your finger on the bottom feeling for the fabric edge. Watch for those sales and coupons!! Sulky blendables, 30 weight, 100% cotton is very nice to use. If you hem with a straight stitch, make it a little longer perhaps 3.0 and add some elastic to make it gathered at the hem edge. -

Lesson Guide Princess Bodice Draping: Beginner Module 1 – Prepare the Dress Form
Lesson Guide Princess Bodice Draping: Beginner Module 1 – Prepare the Dress Form Step 1 Apply style tape to your dress form to establish the bust level. Tape from the left apex to the side seam on the right side of the dress form. 1 Module 1 – Prepare the Dress Form Step 2 Place style tape along the front princess line from shoulder line to waistline. 2 Module 1 – Prepare the Dress Form Step 3A On the back, measure the neck to the waist and divide that by 4. The top fourth is the shoulder blade level. 3 Module 1 – Prepare the Dress Form Step 3B Style tape the shoulder blade level from center back to the armhole ridge. Be sure that your guidelines lines are parallel to the floor. 4 Module 1 – Prepare the Dress Form Step 4 Place style tape along the back princess line from shoulder to waist. 5 Lesson Guide Princess Bodice Draping: Beginner Module 2 – Extract Measurements Step 1 To find the width of your center front block, measure the widest part of the cross chest, from princess line to centerfront and add 4”. Record that measurement. 6 Module 2 – Extract Measurements Step 2 For your side front block, measure the widest part from apex to side seam and add 4”. 7 Module 2 – Extract Measurements Step 3 For the length of both blocks, measure from the neckband to the middle of the waist tape and add 4”. 8 Module 2 – Extract Measurements Step 4 On the back, measure at the widest part of the center back to princess style line and add 4”. -
Evicore Musculoskeletal Imaging Guidelines
CLINICAL GUIDELINES Musculoskeletal Imaging Policy Version 2.1 Effective October 1, 2020 eviCore healthcare Clinical Decision Support Tool Diagnostic Strategies: This tool addresses common symptoms and symptom complexes. Imaging requests for individuals with atypical symptoms or clinical presentations that are not specifically addressed will require physician review. Consultation with the referring physician, specialist and/or individual’s Primary Care Physician (PCP) may provide additional insight. CPT® (Current Procedural Terminology) is a registered trademark of the American Medical Association (AMA). CPT® five digit codes, nomenclature and other data are copyright 2020 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values or related listings are included in the CPT® book. AMA does not directly or indirectly practice medicine or dispense medical services. AMA assumes no liability for the data contained herein or not contained herein. © 2020 eviCore healthcare. All rights reserved. Musculoskeletal Imaging Guidelines V2.1 Musculoskeletal Imaging Guidelines Procedure Codes associated with Musculoskeletal Imaging 3 MS-1: General Guidelines 5 MS-2: Imaging Techniques 8 MS-3: 3D Rendering 12 MS-4: Avascular Necrosis (AVN)/Osteonecrosis 13 MS-5: Fractures 16 MS-6: Foreign Body 20 MS-7: Ganglion Cysts 22 MS-8: Gout/Calcium Pyrophosphate Deposition Disease (CPPD)/ Pseudogout/Chondrocalcinosis 24 MS-9: Infection/Osteomyelitis 26 MS-10: Soft Tissue Mass or Lesion of Bone 29 MS-11: Muscle/Tendon Unit -

Impoved Family Manual.Pdf
FORM 7129 . July 7, 1891. Supersedes Form 7006 . DIRECTIONS FOR USING THE 1MPKO),7r,D IAPXIL~q SIXGER st.-AWING ACHINE1 THE SINGER MANUFACTURING GO., NEW YORK. 1891 . DIRECTIONS FOR USING ~ ~- ~ ~~- -~~ e~ == " ~~ ~ . ce ca ~ ~ c . ~~-- ' -- m_--' B . ..................... ~ a 8 w ~ ~ ~ ~ ~ ~ " THE IMPROVED FAMILY SINGER . FIG. 2. ~1E4 __._Stop Motion _.,.Right Lag IMPROVED FAMILY MACHINE, WITH STAND. DIRECTIONS FOR USING FIG. 3. OILING PLACES SHOWN BY ARROWS . AILING PLACES SHOWN BY ARROWS. DIRECTIONS FOR USENG THE 11112er Y rr+peoved Parr,Iiy t4achile. To Oil the Machine. Be sure that every part is clean before you commence to sew. If the machine runs hard at any time, IT IS CERTAIN that someplace has not been oiled. Oil holes will be found for all bearings which cannot be reached without them. Each place requiring oil is indicated by an arrow head in the cuts on the opposite page. The shuttle should be oiled sparingly, but often, if the machine is in constant use ; always be careful to use no more oil than is needed, a single drop being sufficient at any point. If the machine runs hard after standing idle for some time, use a little kero- sene oil or benzine on the wearing points, run rapidly, zvi~e clean, and then oil with the BEST slerni oil, which should always be used. To make sure of getting good oil, buy it at at any of the Company's offices or from its authorized representatives. The genuine oil is put up in bottles which have The Singer Manufacturing Company's " trade-mark " blown in their panel, and bear the Company's label. -

Clinical Guidelines
CLINICAL GUIDELINES Joint Services Guidelines Version 1.0.2019 Clinical guidelines for medical necessity review of comprehensive musculoskeletal management services. © 2019 eviCore healthcare. All rights reserved. Regence: Comprehensive Musculoskeletal Management Guidelines V1.0.2019 Large Joint Services CMM-311: Knee Replacement/Arthroplasty 3 CMM-312: Knee Surgery-Arthroscopic and Open Procedures 14 CMM-313: Hip Replacement/Arthroplasty 35 CMM-314: Hip Surgery-Arthroscopic and Open Procedures 46 CMM-315: Shoulder Surgery-Arthroscopic and Open Procedures 47 CMM-318: Shoulder Arthroplasty/ Replacement/ Resurfacing/ Revision/ Arthrodesis 62 ______________________________________________________________________________________________________ © 2019 eviCore healthcare. All Rights Reserved. Page 2 of 69 400 Buckwalter Place Boulevard, Bluffton, SC 29910 (800) 918-8924 www.eviCore.com Regence: Comprehensive Musculoskeletal Management Guidelines V1.0.2019 CMM-311: Knee Replacement/Arthroplasty CMM-311.1: Definition 4 CMM-311.2: General Guidelines 5 CMM-311.3: Indications and Non-Indications 5 CMM-311.4 Experimental, Investigational, or Unproven 9 CMM-311.5: Procedure (CPT®) Codes 10 CMM-311.6: References 10 ______________________________________________________________________________________________________ © 2019 eviCore healthcare. All Rights Reserved. Page 3 of 69 400 Buckwalter Place Boulevard, Bluffton, SC 29910 (800) 918-8924 www.eviCore.com Regence: Comprehensive Musculoskeletal Management Guidelines V1.0.2019 CMM-311.1: Definition -

Predictors of Outcome Following Standardized Rehabilitation for Patients with Shoulder Pain
University of Kentucky UKnowledge Theses and Dissertations--Rehabilitation Sciences Rehabilitation Sciences 2013 Predictors of Outcome Following Standardized Rehabilitation for Patients with Shoulder Pain Stephanie D. Moore University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Recommended Citation Moore, Stephanie D., "Predictors of Outcome Following Standardized Rehabilitation for Patients with Shoulder Pain" (2013). Theses and Dissertations--Rehabilitation Sciences. 15. https://uknowledge.uky.edu/rehabsci_etds/15 This Doctoral Dissertation is brought to you for free and open access by the Rehabilitation Sciences at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Rehabilitation Sciences by an authorized administrator of UKnowledge. For more information, please contact [email protected]. STUDENT AGREEMENT: I represent that my thesis or dissertation and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained and attached hereto needed written permission statements(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine). I hereby grant to The University of Kentucky and its agents the non-exclusive license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. I agree that the document mentioned above may be made available immediately for worldwide access unless a preapproved embargo applies. -

Simplified Sewing: Hems
South Dakota State University Open PRAIRIE: Open Public Research Access Institutional Repository and Information Exchange SDSU Extension Fact Sheets SDSU Extension 1964 Simplified Sewing: Hems Cooperative Extension South Dakota State University Follow this and additional works at: https://openprairie.sdstate.edu/extension_fact Recommended Citation South Dakota State University, Cooperative Extension, "Simplified Sewing: Hems" (1964). SDSU Extension Fact Sheets. 865. https://openprairie.sdstate.edu/extension_fact/865 This Fact Sheet is brought to you for free and open access by the SDSU Extension at Open PRAIRIE: Open Public Research Access Institutional Repository and Information Exchange. It has been accepted for inclusion in SDSU Extension Fact Sheets by an authorized administrator of Open PRAIRIE: Open Public Research Access Institutional Repository and Information Exchange. For more information, please contact [email protected]. .. ... -~--- - --v · . --,-.-.- , -. ·. ..•, .. ·'··· .••,.,. - .t:\. --(. ......., • ... ·\•i• ....,.,•-•1•,··...- .,.. "\' ·,- • • • -:\. -: ·):.~\:,..,:}:,:.·,:,..,:;:,:.~:,-:-,:.0:.- ·,~\:,.!;;;; ··:,:.\!.t:,-;..:,t;.,:,:,:.i:1:,:.'.:.•; .-·F_:,~::::_:.~:~~~~~;.:::z~:;:'.·---~-~;:~~L ::·.1~~~~1::.:;.:_;~~: File Copy FS244 THE l-lE~I of your dress can have the "professional - Wearer should stand in a natural position with look" or the "homemade look." In general, the best arms at sides and weight on both feet. hem is the least conspicuous, and every step in making a hem is planned with this in mind There are several methods of marking a hem. You may use any one of these: The professional touch is recognize-cl by the follow- ing characteristics: Various types of chalk markers or pin markers - Inconspicuous from the right side Yardstick - Even distance from the floor Tailor's square. - Wide enough for good proportion and to gi\.re With some of these you can mark enough weight to hang well your own hem; others require a - Even in width help«. -
To Complete the Pattern Join Bodice #1 to #2 at Circle Front Bodice #1
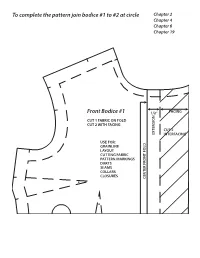
To complete the pattern join bodice #1 to #2 at circle Chapter 2 Chapter 4 Chapter 6 Chapter 19 Front Bodice #1 1/2” FACING N CUT 1 FABRIC ON FOLD CUT 2 WITH FACING CUT 2 EXTENSIO INTERFACING USE FOR: GRAINLINE LAYOUT CUTTING FABRIC PATTERN MARKINGS DARTS SEAMS COLLARS CLOSURES CENTER FRONT FOLD To completeTo the pattern join bodice #1 to #2 at circle TO COMPLETE THE PATTERN JOIN BODICE #1 TO #2 AT CIRCLE STITCH TO MATCHPOINTS FOR DART TUCK FRONT BODICE #2 Front Bodice #2 Chapter 2 Chapter 4 Chapter 6 Chapter 19 STITCH TO MATCHPOINTS FOR DART TUCKS To complete the pattern join bodice #3 to #4 at circle Chapter 2 Chapter 4 Chapter 6 Back Bodice #3 CUT 2 FABRIC USE FOR: CK SEAM GRAINLINE LAYOUT CUTTING FABRIC CK FOLD PATTERN MARKINGS DARTS SEAMS COLLARS CENTER BA CUT HERE FOR CENTER BA To completeTo the pattern join bodice #3 to #4 at circle STITCH TO MATCHPOINTS FOR DART TUCKS Back Bodice #4 Chapter 2 Chapter 4 Chapter 6 Chapter 4 Chapter 11 Chapter 14 Chapter 17 MATCHPOINT Front Skirt #5 CUT 1 FABRIC USE FOR: V SHAPED SEAM WAISTBAND WAIST FACING BIAS WAIST FINISH CURVED/ALINE HEM BIAS FALSE HEM CENTER FRONT FOLD Chapter 4 Chapter 11 Chapter 14 Front Yoke #6 CUT 1 FABRIC CUT 1 INTERFACING USE FOR: V SHAPE SEAM WAISTBAND WAIST FACING BIAS WAIST FINISH C. F. FOLD C. F. MATCHPOINT Chapter 4 Chapter 6 Chapter 10 Chapter 11 Chapter 14 Chapter 17 MARK DART POINT HERE Back Skirt #7 CUT 2 FABRIC USE FOR: SEAMS ZIPPERS WAISTBAND WAIST FACING BIAS WAIST FINISH CURVED ALINE HEM BIAS FALSE HEM Chapter 4 CUT ON FOLD Chapter 12 Chapter 17 H TC NO WHEN -

Taking Shape DARTS ADD SHAPE TURNING a FLAT PIECE of FABRIC INTO a THREE-DIMENSIONAL FORM to MATCH the CONTOURS of the BODY LINDA TURNER GRIEPENTROG
Techniques Taking Shape DARTS ADD SHAPE TURNING A FLAT PIECE OF FABRIC INTO A THREE-DIMENSIONAL FORM TO MATCH THE CONTOURS OF THE BODY LINDA TURNER GRIEPENTROG ustline, hip, waistline to tummy, elbow and shoulder. Darts can be horizontal, vertical or anywhere in between, straight or curved, but the stitching principles are the same. BThe goal of quality dart stitching is smooth, pucker-free points that don’t call attention to themselves. SHAPING A single-point dart is shaped like a triangle, and when stitched it takes a wedge of fabric out of the garment allowing for controlled fullness at the point. A single dart may be on the lengthwise fabric grain, angled or slightly curved. (1) A double-point or contour dart is diamond or rugby ball shaped, and is used to shape the waistline, leaving fullness at both ends for the bust and hip. (2) A French dart is a curved shape from the garment side seam to the bustline. This dart has cut edges joined like a seam. (3) V9082 Vintage Vogue, 1960. Misses’ A5(6-8-10-12-14) E5(14-16-18-20-22). Sew Rating: Average. Price code Orange. Illustrations: Theresa O’Connell Theresa Illustrations: 1 2 3 26 SEW TODAY May/June 2019 MARKING to anchor the stitches. Stitch (7) and stitch toward the point, Darts are indicated on the along the line, removing the A third technique for dart then repeat for the other pattern tissue by either solid pins as you get to them. Taper point, slightly overlapping or dashed lines and a dot the stitching to the point the beginning stitching lines at the point. -

Breakthrough in Shoulder Surgery Brings New Hope to Patients
Breakthrough in Shoulder Surgery Brings New Hope to Patients ll her life, Millie has been active – raising six children, bowling in a league, even skating in After a shoulder replacement, Millie Athe roller derby 60 years ago. But when is back to the job she loves at the 81-year-old from Chantilly began Louise Archer Elementary School. experiencing difficulty raising her arms to complete simple tasks such as brushing her hair or reaching up to a shelf, she knew something was wrong. Her limited range of motion also made it hard to do her office job at Louise Archer Elementary School in Vienna. Millie consulted Commonwealth surgeon David Novak, MD, who diagnosed advanced osteoarthritis in both her shoulders. When several months of cortisone shots failed to alleviate her symptoms, she opted for a total shoulder replacement on her left side. This procedure involves replacing the arthritic joint surfaces with a metal and plastic implant. The components come Dr. Novak is among just a handful of surgeons in the area who in various sizes and are either cemented or press fit into the bone. perform this advanced procedure. “Patients like Millie, with end-stage arthritis and intact rotator cuff tendons, who no longer respond to conservative treatment – such Following both of her surgeries, Millie wore a sling for four weeks. as NSAIDs, cortisone or physical therapy – are generally good She spent two months working with a physical therapist on exercises candidates for total shoulder replacement,” Dr. Novak explains. to regain range of motion and strengthen her shoulder joint. It was all part of a rigorous rehabilitation program that every patient goes The surgery restored function to Millie’s left shoulder and she was through.